
Abstract
Introduction:
As the prevalence of obesity increases worldwide, an increasing proportion of surgical candidates have an elevated body mass index (BMI), with associated metabolic syndrome. Yet there exists limited evidence regarding the effect of elevated BMI on surgical outcomes in robotic surgeries. We examined whether obese patients had worse perioperative outcomes and postoperative renal function after robotic partial nephrectomies (RPNs).
Materials and Methods:
We performed a multi-institutional analysis of 1770 patients who underwent RPNs between 2008 and 2015, allowing time for the data set to mature. Associations between BMI, as a continuous and categorical variable, and perioperative outcomes, acute kidney injury (AKI, >25% reduction in estimated glomerular filtration rate [eGFR]) at discharge, and change in eGFR per month were analyzed. AKI and eGFR were evaluated using multivariable logistic and linear regression models adjusted for confounders, including age, Charlson comorbidity index, tumor size, and the identity of the surgeon.
Results:
In total 45.2% (n = 529) of patients were found to be obese, with a greater prevalence of hypertension and diabetes in overweight and obese patients. Obese patients were more likely to have malignant tumors (>77% vs 68%, p < 0.001) and trended toward having larger tumors (3.0 cm vs 2.8 cm; p = 0.061). Heavier patients required longer operative times (166–196 minutes vs 155 minutes; p < 0.001), although equivalent warm ischemia times (p = 0.873). Obesity did not correlate with an increased complication rate (p > 0.05). On multivariable analysis, obesity (odds ratio [OR] = 1.81; p = 0.031), male sex (OR = 1.54; p = 0.028), and larger tumor size (OR = 1.23; p < 0.001) were associated with a significant increase in the likelihood of AKI at discharge. BMI above normal weight was not associated with greater eGFR decline per month post-RPN.
Conclusions:
Obesity was associated with equivalent perioperative outcomes and long-term renal function. Further research is warranted into how obesity and metabolic syndrome may foster a more aggressive tumor environment. RPN appears to be an equally safe operative option for patients regardless of obesity status.
Introduction:
Obesity in the 21st century continues to pose a global health problem as its prevalence rises. 1 Obese (body mass index [BMI] >30) patients are more likely to have other major health issues, including associated metabolic syndrome, diabetes, and hypertension. In particular, obese patients are at increased risk of developing renal cell carcinoma (RCC). 2,3 The underlying mechanism between obesity and increased RCC is unclear but may be linked to increased insulin and insulin-like growth factor (IGF1R) 4 and risk of diabetes. 5 Interestingly, some studies have found RCC patients with higher BMI have improved survival—the suggested and controversial “obesity paradox.” 6 –8
Obesity's role in influencing perioperative outcomes across disciplines has generated considerable controversy. A large study from the National Surgical Quality Improvement Database (n = 141,802) across 16 common surgeries demonstrated the procedure-specific effects of BMI, with clear trends toward increased risk of wound complications, kidney injury, and thromboembolic events. 9 Paradoxically, in some of the examined surgeries obesity was associated with decreased risks. Notably, BMI had no effect on perioperative complications in nephrectomies. As the urologic community transitions to an increased use of the robotic partial nephrectomies (RPNs) for the treatment of suspected RCC, 10 it is imperative to have an understanding of the procedure-specific risks for adequate patient management and counseling. Previously, laparoscopic partial nephrectomies 11 and RPNs 12 have been shown to have similar outcomes to open partial nephrectomy in obese patients, as well as to each other. 13 As RPN has become an established treatment option for amenable masses across BMI types, we report a large, multi-institutional cohort of patients to examine the impact of BMI on perioperative outcomes or postoperative renal function after RPN.
Patients and Methods
Patient population
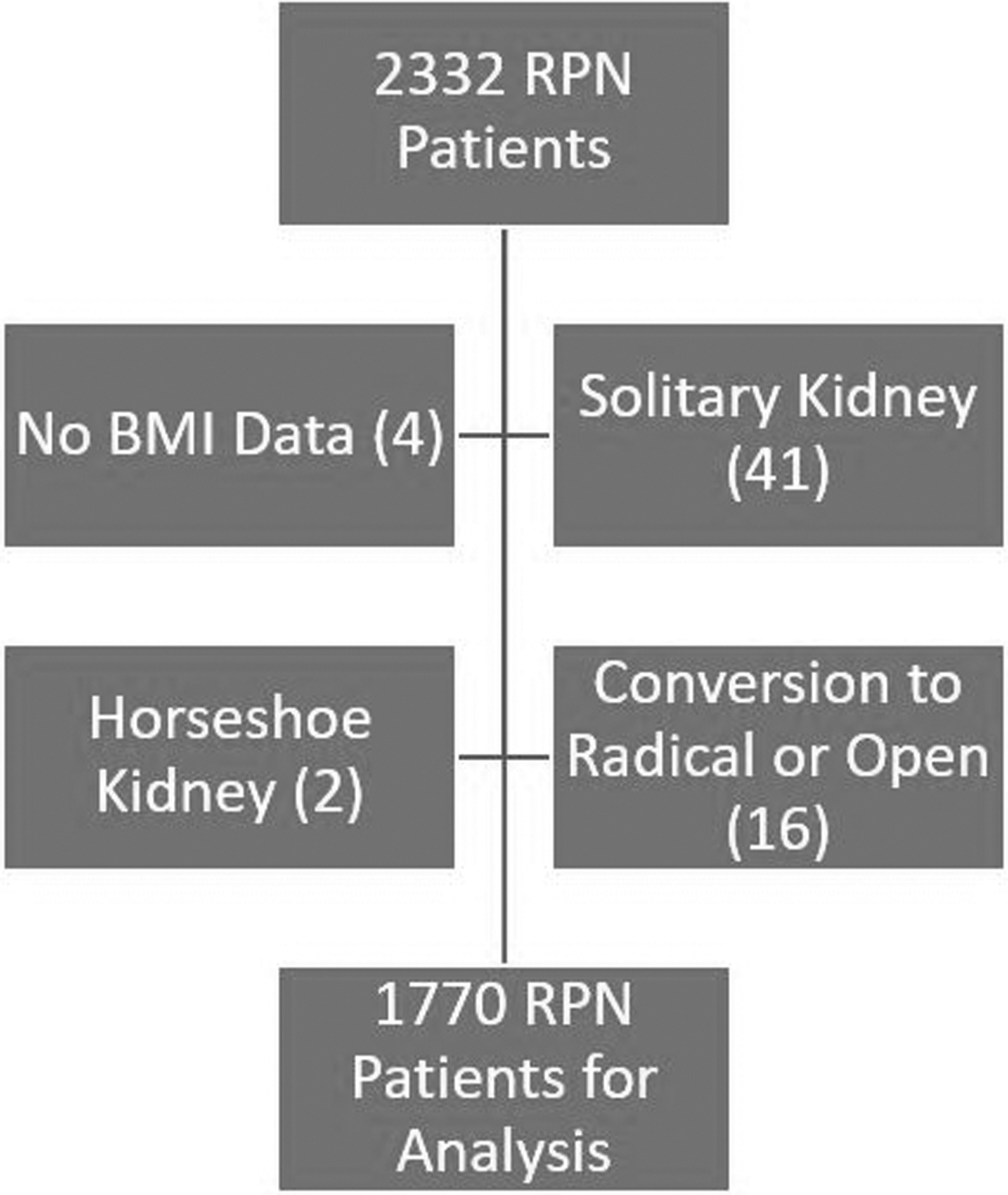
In total 2332 patients who underwent RPNs between 2008 and 2015, performed by one of six high-volume surgeons, were identified from a multi-institutional database, allowing time for postoperative outcomes from the data set to mature. Patients were excluded if they were missing estimated glomerular filtration rate (eGFR) outcomes (529), BMI data (4), had a solitary kidney (41), a horseshoe kidney (2), or their surgeries were converted to radical or open (16) (Fig. 1). A final cohort of 1770 patients remained in the data set for analysis (as some patients met more than one exclusion criteria). All data are stored in Research Electronic Data Capture (REDCap), an institutional review board (IRB)-approved online database with data merged from both individual institutional prospective databases before December 2015 and data recorded prospectively since that date. IRB approval was obtained before the commencement of the study.
Patient selection.
Surgical technique
As previously described, 14 all procedures were performed robotically using the da Vinci Robot (Intuitive Surgical, Inc., Sunnyvale, CA). A multiport approach was performed by all surgeons, with the use of transperitoneal vs retroperitoneal approach chosen based on the surgeon's preference. The decision to clamp the renal artery, vein, or both was made at the discretion of the surgeon. Renorrhaphy was performed in at least two layers and pure enucleation was not performed in any of the procedures.
Outcomes and statistical analysis
The cohort was divided into four subgroups, based on Center for Disease Control groups for obesity. 15 Baseline demographic, tumor characteristics, and perioperative characteristics and outcomes were recorded, as outlined in Table 1. Differences between the subgroups were compared using Kruskal–Wallis tests for continuous variables and chi-squared tests or Fisher's exact tests for categorical variables.
Distribution of Patient, Tumor, and Operative Characteristics According to Body Mass Index
Distribution of continuous variables compared with Kruskal–Wallis tests. Median presented with range in parenthesis.
Distribution of categorical variables compared with chi-squared tests of independence or Fisher's exact tests. Frequencies presented with % in parenthesis.
Comparisons are not adjusted for any covariates.
Bold values indicate significance at p < .05.
BMI = body mass index; CCI = Charlson comorbidity index; eGFR = estimated glomerular filtration rate; HTN = Hypertension.
The association between BMI and acute kidney injury (AKI) was examined using univariable and multivariable logistic regression models using BMI as a categorical variable and as a linear variable. Variables were included in the model if they were both associated with AKI at the p < 0.20 level and also associated with BMI at the p < 0.20 level. Variables included were BMI, sex, Charlson comorbidity index, diagnosis of hypertension, diabetes, tumor size, clamp type, and tumor location.
The association between BMI and eGFR at 3–24 months was examined using univariable and multivariable linear regression models using BMI as a categorical variable and as a linear variable. Variables were included in the model if they were both associated with AKI at the p < 0.20 level and also associated with BMI at the p < 0.20 level. Variables included were BMI, age, sex, Charlson comorbidity index, diagnosis of hypertension, diabetes, and tumor size.
Statistical analyses were conducted with R version 3.4.1 with statistical significance considered at the p < 0.05 level.
Results
Baseline characteristics and perioperative outcomes
Baseline demographics, tumor, and operative characteristics for the different BMI categories are presented in Table 1. A final cohort of 1770 patients with two kidneys underwent RPNs by one of six high-volume surgeons. Of these, 363 patients were considered normal weight (BMI <25 kg/m2), 607 were overweight (BMI 25–29.99 kg/m2), 633 were obese (BMI 30–39.99 kg/m2), and 167 were morbidly obese (BMI ≥40 kg/m2). In comparing BMI groups, significantly different characteristics included age, sex, BMI, hypertension, diabetes, malignancy, longer operative time, and greater blood loss (p < 0.001). There was also a trend toward increased tumor size with greater BMI (3.0 vs 2.8 cm, p = 0.061).
Kidney function outcomes: acute kidney injury and eGFR progression
AKI with BMI as categorical on the left and BMI as continuous on the right is presented in Table 2. In multivariable analysis with BMI as a categorical variable, AKI at discharge was associated with obese patients (odds ratio [OR] = 1.81, confidence interval [CI] = 1.07–3.16; p = 0.031), male sex (OR = 1.54, CI = 1.07–2.25; p = 0.028), and larger tumor size (OR = 1.23, CI = 1.10–1.38; p < 0.001), and approached statistical significance in morbidly obese patients (OR = 2.00, CI = 0.99–4.06). (Fig. 2). On subanalysis, there was a lower risk of AKI in off-clamp vs main artery clamping (OR = 0.41, CI = 0.19–0.83; p = 0.018). Being overweight was not significantly associated with AKI. In multivariable analysis with BMI as a continuous variable, AKI at discharge was similarly associated with BMI (OR = 1.03, CI = 1.00–1.06; p = 0.031), male sex (OR = 1.58, CI = 1.09–2.29; p = 0.016), and larger tumor size (OR = 1.22, CI = 1.09–1.37; p < 0.001). There was a lower risk of AKI in off-clamp vs main artery clamping (OR = 0.41, CI = 0.19–0.82; p = 0.017). Diabetes and hypertension were not significantly associated with AKI in either model. The predicted probability of AKI is displayed in Figure 2.
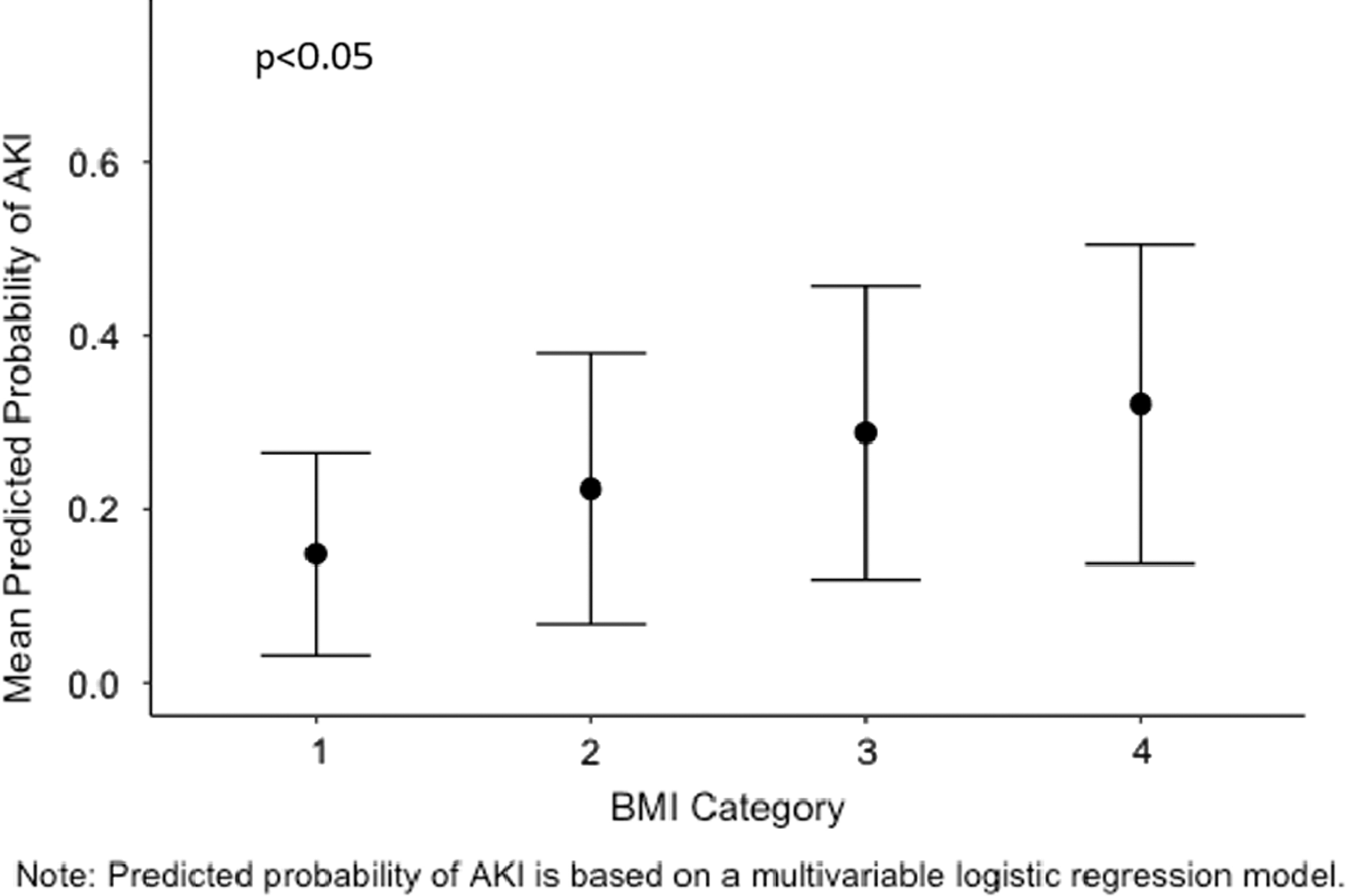
BMI and the predicted probability of acute kidney injury. BMI = body mass index.
Body Mass Index and Acute Kidney Injury at Discharge After Robotic Partial Nephrectomy
Variables were included in the model if they were both (a) associated with AKI at the p < 0.20 level and (b) associated with BMI categorically at the p < 0.20 level for the first model or BMI continuous at the p < 0.20 level for the second model.
Bold values indicate significance at p < .05.
AKI = acute kidney injury; OR = odds ratio; CI = confidence interval.
eGFR with BMI as categorical on the left and BMI as continuous on the right is presented in Table 3. In multivariable analysis with BMI as a categorical variable, age (p < 0.001), months post-RPN (p = 0.005), Charlson comorbidity index (p = 0.027), and hypertension (p = 0.023) were associated with a decline in eGFR. (Fig. 3) In BMI as a continuous variable, age (p < 0.001), months post-RPN (p = 0.031), Charlson comorbidity index (p = 0.024), and hypertension (p = 0.026) were similarly associated with a decline in eGFR. Tumor size, sex, and diabetes were not significantly associated with a change in eGFR in either model. The change in eGFR stratified by BMI category is displayed in Figure 3.
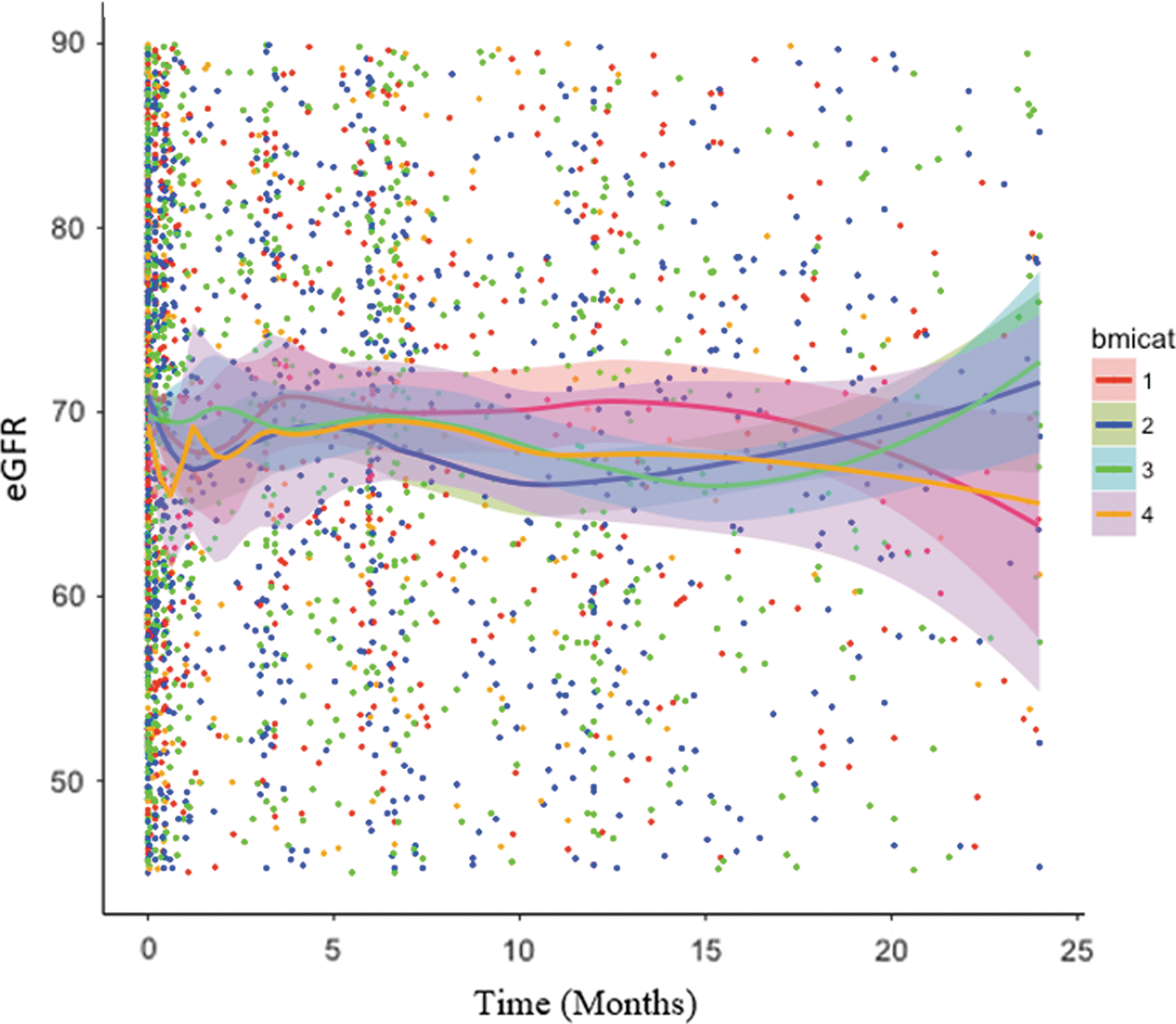
Estimated glomerular filtration rate after robotic partial nephrectomy stratified by BMI class.
Body Mass Index and the Change in Estimated Glomerular Filtration Rate Between 3 and 24 Months Post-Robotic Partial Nephrectomy
Variables were included in the model if they were both (a) associated with eGFR or the change in eGFR over time at the p < 0.20 level and (b) associated with BMI categorically at the p < 0.20 level for the first model or BMI continuous at the p < 0.20 level for the second model.
eGFR over time: the square root of eGFR was used because of violations of assumptions of the linear mixed effects model when using a nontransformed version of eGFR. Fitted values and residuals from the model were plotted against each other, the distribution of residuals was evaluated using histograms and standardized as well as Pearson residual plots were evaluated to test assumptions of the linear mixed effects model.
The linear mixed effects model, including random effects for the surgeon, and patient were tested for the best fit according to whether a random intercept, random intercept + random slope model, and whether a quadratic term for time should be included in the model. The model with the lowest Akaike information criterion was selected as the final model.
Bold values indicate significance at p < .05; 2quadratic term for time.
Discussion
This large retrospective study lends several key insights into nonmetastatic kidney cancer patients and the effects that BMI may have on their care and prognosis. As rates of obesity rise, 1 these data suggest that a robotic approach is a viable surgical option across BMI status. Furthermore, the higher propensity for malignancy among obese patients suggests a possible mechanistic component of the metabolic syndrome.
The breakdown of baseline characteristics of this cohort suggests several insights into the complex interplay of BMI and malignancy. Patients with higher BMIs trended toward having larger tumors (p = 0.06) and were more likely to have a malignant tumor (p < 0.001), which is consistent with renal cancer kinetics and the majority of published data. 16 –21 Notably, this trend does not appear across all ethnicities nor is it always found to be linear. Examining a Korean population, Choi and colleagues found that obese patients had smaller tumors and lower likelihood of metastases, 22 whereas Park and colleagues found that visceral obesity had an increased risk of disease recurrence at both extremes, rather than a linear relationship. 23 The distinction between BMI and visceral obesity was further drawn out by Zhu and colleagues, who found that visceral obesity was associated with worse Fuhrman grade, whereas BMI was not. 24 Our data support the theory that increasing BMI is associated with increased tumor size and chance of malignancy, but because of the absence of long-term follow-up survival data in this localized cohort, we cannot comment on prognostic significance.
Our data support much of the prior literature on obesity and perioperative outcomes. Several analyses have demonstrated that although obesity may pose unique intraoperative challenges, it does not necessarily lead to an increased complication rate in RPNs. In particular, Kiziloz and associates, 25 Komninos and colleagues, 26 and Abdullah and colleagues, 21 each of which encompassed several prior single institution studies, did not demonstrate an increased complication rate. These data suggest equivalent outcomes in terms of length of stay, complication rate, and positive margin rates.
There exists conflicting data on the role of different types of obesity and partial nephrectomy perioperative outcomes. Macleod et al. suggested that the key characteristic that defined case complexity was perinephric fat thickness and showed that increasing perinephric fat was associated with increased estimated blood loss (EBL) and operative time. 27 Yet, Ioffe and coworkers examined several patterns of obesity, including visceral, subcutaneous, and perinephric, and did not see any difference in outcomes. 28 Our baseline cohort exhibited expected differences in terms of hypertension, diabetes, and associated longer operative times; yet, we did not ultimately see any change in complication rate and the increase in AKI was not reflected in long-term renal function outcomes. This may suggest that although increasing BMI does portend toward a more complicated positioning, setup, or dissection, as evidenced by extended operative times, this elevated risk is not prohibitive. Fundamentally, these data demonstrate RPN to be a safe and effective modality for patients regardless of BMI status.
Long-term renal function outcomes appear to be similar across BMI statuses, whereas rates of AKI are increased in obese patients. This relationship may stem from the small trend toward larger tumors in obese patients and a requisite larger portion of surrounding tissue removed, trends that are obviated at long-term follow-up. These results are consistent with our groups' prior findings on extended warm ischemia time (WIT) in which patients are able to recover from the surgical insult adequately. 29 Although this cohort did see a significant increase in EBL and operative time, it saw no change in WIT, suggesting that the complexity of the case is found in accessing and exposing the renal tumor rather than the excision and renorrhaphy. Conversely, in a minimally invasive cohort, Richards and colleagues found obesity to be linked with new onset chronic kidney disease stage 3 and a greater decline in eGFR—findings not supported by our data. 30
Our findings must be understood in the context of the limitations of this retrospective cohort. Although selection for robotic surgery would naturally be a source of bias, it is worth noting that this cohort reflects a wide range of BMIs that closely resembles the American population. 15 Although larger tumor size and prior abdominal surgeries were previously strong indicators for an open approach, the improvement in technology and familiarity with robotic techniques has allowed most patients to be able to be offered a robotic approach. In addition, this cohort reflects patients who ultimately underwent robotic surgery and, therefore, excludes not only patients who underwent an open or laparoscopic approach, but patients treated nonoperatively as well. Specifics of the surgical technique were not standardized across sites and the generally safe outcomes reflect the experience of high-volume surgeons in tertiary care facilities. Preoperative imaging from each site was not available for reevaluation to differentiate between the types of obesity each patient had. In addition, some patients were missing data on renal function, potentially introducing a source of bias into that portion of the results. In particular, the fewer number of morbidly obese patients may have limited the statistical differences in that subcohort. As obesity rates continue to rise worldwide, these data are supportive of the clinical utility of the robotic platform in mitigating the surgical risk of obesity.
Conclusions
Patients with greater BMI had higher rates of malignancy, suggesting that obesity may play a causative role in fostering more aggressive renal cancer. Despite underlying differences in comorbidities, RPN was found to be an equivalent surgical option for patients regardless of BMI, with minimal or no clinical differences in perioperative outcomes or long-term renal function.
Footnotes
Author Disclosure Statement
Authors D.C.R., M.K., Y.K., A.T.B., D.J.P., A.B., A.K.H., J.R.P., and K.K.B. have no disclosures to report. Dr. D.D.E. receives personal fees from Intuitive Surgical, Medtronic, Conmed, outside submitted study. Dr. R.A. receives grants from Intuitive Surgical and Conmed, outside submitted study.