
Abstract
Introduction:
Although general guidelines exist directing the management of new/novel oral anticoagulants (NOACs) in the perioperative period for open/endoscopic procedures, no consensus exists for those patients being considered for shockwave lithotripsy (SWL). To gauge current practice, we administered a survey to the international endourologic community.
Methods:
A web-based survey was sent to current Endourological Society members. Respondents were asked whether they would consider SWL in patients receiving NOACs, and if they used SWL how these agents were managed perioperatively. Respondents were also asked which physicians in the patients' circle of care managed the discontinuation and reinstitution of the drugs.
Results:
There were 165 respondents from 27 countries. Approximately 92.7% of urologists had access to SWL but only 53.4% indicated they would offer SWL to patients receiving NOACs. Among these urologists, 63.3% relied on internal medicine/hematology/cardiology colleagues to counsel patients on the discontinuation of NOACs pretreatment, whereas the majority (64%) handled the resumption guidance themselves. There was wide variability in the management of NOACs before lithotripsy, with discontinuation varying from 2 to 7 days. Resumption was more consistent, ranging from 1 to 2 days or when hematuria resolved. None of the respondents reported knowledge of adverse effects such as perinephric hematomas or cardiovascular morbidity.
Conclusions:
A large percentage of globally surveyed endourologists do not offer SWL to patients who are taking NOACs. Among those that do offer SWL, there seems to be a absence of consensus on optimal duration of discontinuation, suggesting a need to establish evidence-based guidance to optimize patient outcomes.
Introduction
Since their introduction into clinical practice in 2011, the new/novel oral anticoagulants (NOACs) apixaban, rivaroxaban, dabigatran, and most recently edoxaban, have resulted in significant changes in the management of stroke risk in patients with nonvalvular atrial fibrillation. These agents have shown comparable stroke risk reduction to warfarin in large international multicenter trials and are being increasingly prescribed because of their ease of use compared with warfarin, which necessitates ongoing monitoring because of its narrow therapeutic range and has potentially hazardous drug and food interactions. 1 –3
Although widely prescribed, many urologists may not be familiar with the pharmacokinetic and pharmacodynamic properties of these new agents. Understanding their effects on the coagulation cascade and the management of their discontinuation and resumption in the perioperative period is important for all physicians.
Apixaban, rivaroxaban, and edoxaban function as factor Xa inhibitors, whereas dabigatran's effect is through thrombin inhibition. Apixaban typically is dosed twice daily, has a half-life of 8 to 15 hours and is eliminated primarily through hepatobiliary excretion. 4 Rivaroxaban and edoxaban are prescribed as a single daily dose with half-lives of 8 to 13 hours, and have greater renal elimination than apixaban. 5 Dabigatran is primarily renally excreted and has a half-life of 12 to 14 hours. 4 For the three agents eliminated by renal excretion, if patients have normal renal function, the anticoagulant effect is gone by four to five half-lives, meaning the drugs should be stopped for at least 48 hours before an operation with a high bleeding risk. 6 For patients with renal impairment, creatinine clearance should be determined to properly gauge treatment cessation that may be 72 hours or longer depending on the degree of renal dysfunction. 6 No blood monitoring exists for these agents and the drugs' anticoagulant effects are not easily reversible. Since their initial clinical release however, reversal agents are now available. Idarucizumab as an antidote to dabigatran, received U.S. Food and Drug Administration (FDA) approval in 2015, and has been shown to be effective when urgent anticoagulation reversal is required. 7 In the Spring of 2018, the FDA approved andexanet alfa, which has demonstrated effective reversal in the setting of acute major bleeding associated with Factor Xa inhibitors. 8
In 2014, the International Consultation on Urological Disease/American Urological Association commissioned and published consensus-based recommendations on the periprocedural management of anticoagulants and antiplatelet agents relevant to urologic procedures. 9 Recommendations for NOAC periprocedural management in patients with nonvalvular atrial fibrillation included stratifying patients according to the procedural bleeding risk and whether the procedure was emergent or elective. It was recommended that for elective procedures, the NOACs should be discontinued 2 to 5 days preoperatively. 9 If the risk of surgical bleeding is considered low, discontinuation 2 days preoperatively was suggested, and if the bleeding risk is high, 3 days of cessation before operation was recommended. 9 These guidelines were drafted based on available evidence and were intended to provide direction to clinicians regarding open and endoscopic procedures. The document did not specifically provide direction on NOACs and shockwave lithotripsy (SWL) but did provide a general recommendation that “anticoagulants/antiplatelet agents should be discontinued and/or reversed prior to shock wave lithotripsy,” and that “the timing of cessation and reinstitution of oral anticoagulants/antiplatelets should include an assessment of the risks of thrombotic complications versus bleeding using a coordinated multidisciplinary plan with stratification according to risks.” 9
Managing patients who are at risk for a thromboembolic event in the periprocedural time period who are on anticoagulation therapy is challenging. The ischemic stroke risk for patients with atrial fibrillation is calculated by the cumulative score for congestive heart failure (CHADS2) score, which is a cumulative score for congestive heart failure (assigned 1 point), hypertension (treated or >140/90) (1 point), age >75 years old (1 point), diabetes mellitus (1 point), and previous stroke or transient ischemic event (2 points). 10 For patients with a high CHADS2 score or other significant risk factors such as mechanical heart valves, thromboembolism after previous cessation of anticoagulation, recurrent venous thromboembolism, thrombophilia, or active malignancy, continuing their anticoagulation or periprocedural bridging anticoagulation with heparin has been recommended. 9,11,12
Unfortunately, the literature related to SWL and the risks of bleeding associated with antiplatelet/anticoagulants in general has been considered low quality because of retrospective and nonstandardized study designs. 13 Moreover, no publications specifically address SWL and the periprocedural management of NOACs. In fact, despite the absence of specific data, SWL has been classified as a high-risk bleeding procedure. 14,15 Baron and colleagues included SWL, transurethral prostatectomy, bladder tumor resection, renal tumor ablation, and kidney biopsy as high-risk bleeding procedures for the purposes of determining the safety of bridging anticoagulation. 15 All these procedures present an inability to apply direct pressure to the area of bleeding should hemorrhage occur. In fact, SWL relies solely on the body's coagulative system for hemostasis.
Given the lack of specific guidance on the appropriate management of NOACs in patients being considered for SWL, we wished to canvass an international group of endourologists for their opinions on handling this clinical scenario. By gathering this information we hoped to identify practice patterns that might be a focus for education initiatives, and future evidence-based guidelines.
Materials and Methods
A 10-question survey was constructed containing multiple choice responses. Five of the questions allowed for free text entry if the potential responses provided were not suitable to an individual respondent.
The questionnaire was hosted on the web-based survey host (Survey Monkey™;
The first four questions were posed to collect demographic data including country of practice, years in practice, academic vs community practice setting, and previous fellowship training.
In the fifth question, participants were asked in general terms, if they provided SWL as a treatment option to patients in their practice regardless of whether or not they were taking NOACs. Respondents who did not provide SWL as an option to any of their patients were thanked and informed that their participation in the survey was completed.
The remaining five questions were constructed to capture responses related to whether SWL is offered to patients on NOACs and if so, for how long these agents are stopped preoperatively, when they are restarted postoperatively, and which physician(s) is/are responsible for their perioperative management.
For each question harboring a free text option, all answers were reviewed, and percentages were calculated. Descriptive statistics were used to compare demographic data and survey responses were reported by frequency.
Results
Of the 2000 e-mails sent to members of the Endourological Society, 165 respondents from 27 countries representing 8.3% of the membership completed the survey. The majority of the respondents were from North America (43.0%), with a third of all participants from the United States. Seventeen countries from Europe contributed to 24.6% of the total responses, with the majority of respondents from the United Kingdom and Italy (4.8% each). Twelve countries from Asia contributed to 22.2% of the responses, with India and Turkey having the largest contributions (4.2% and 3.6%, respectively). The majority of completed surveys from South America (7.8%) came from Brazil (4.8%). One respondent from both Egypt and Nigeria comprised Africa's contribution. A single respondent completed the survey but failed to mention his/her country of practice.
The majority (55.5%) of respondents had been in practice for <15 years; 43.3% had been in practice between 5 and 10 years, and 12.2% for <5 years (Fig. 1). The majority of responses (70.1%) were received from urologists in academic practices, with 69.5% having completed endourology fellowship training.
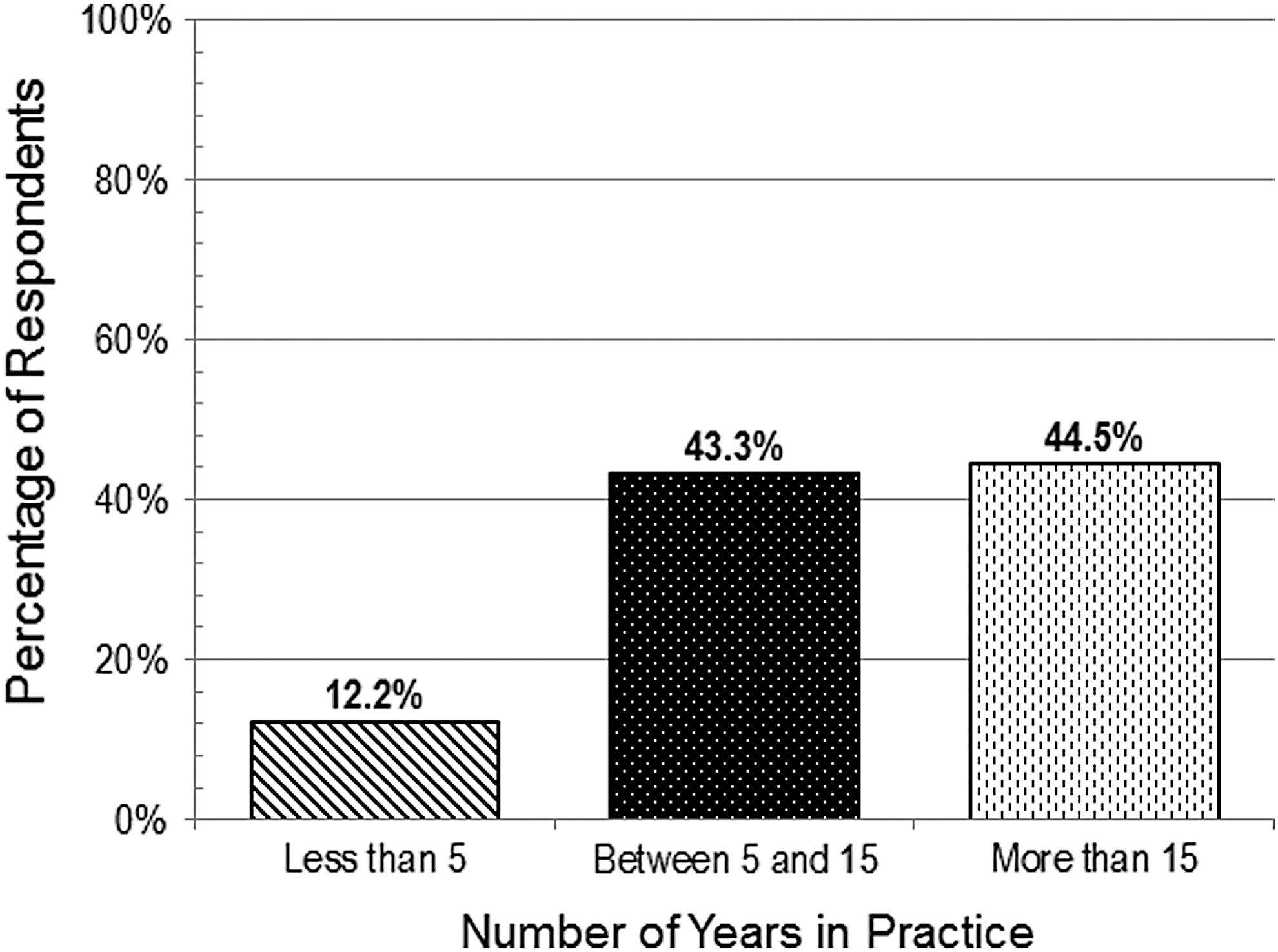
Survey responders classified by duration of clinical practice.
The majority (92.7%) of survey participants indicated they would consider SWL for patients with a symptomatic stone. When asked specifically if they would offer SWL to patients taking NOACs, interestingly only 53.4% of survey participants responded they would consider SWL for these high-risk patients.
When participants were asked which physician in the patient's circle of care makes the decision on the length of time the NOACs be stopped before SWL, more than half of urologists (63.3%) enlisted the help of other physicians, whereas 36.7% of urologists surveyed managed the NOACs preoperatively themselves (Table 1).
Frequency of Survey Responses Classified According to Physician Specialty that Manages Preoperative Discontinuation of New/Novel Oral Anticoagulant Medications Before Shockwave Lithotripsy Treatment
Hematology, anesthesiology, combined with other specialties.
When survey participants were asked how many days before SWL NOACs were stopped at their institution, responses were quite varied with 20.4% stopping 2 days before, 29.6% preferred 3 days, whereas 14.8% discontinued them 4 days pre-SWL. The remaining 35.2% chose the option “other duration” and entered a free text response. The free text answers provided included 5, 6, 7, and 10 days pre-SWL. The most common free text answer was a cessation time of 7 days (13.6%), followed by 5 days (10.5%), whereas 6.2% reported that the duration depended on the specific NOAC medication being used (Fig. 2).
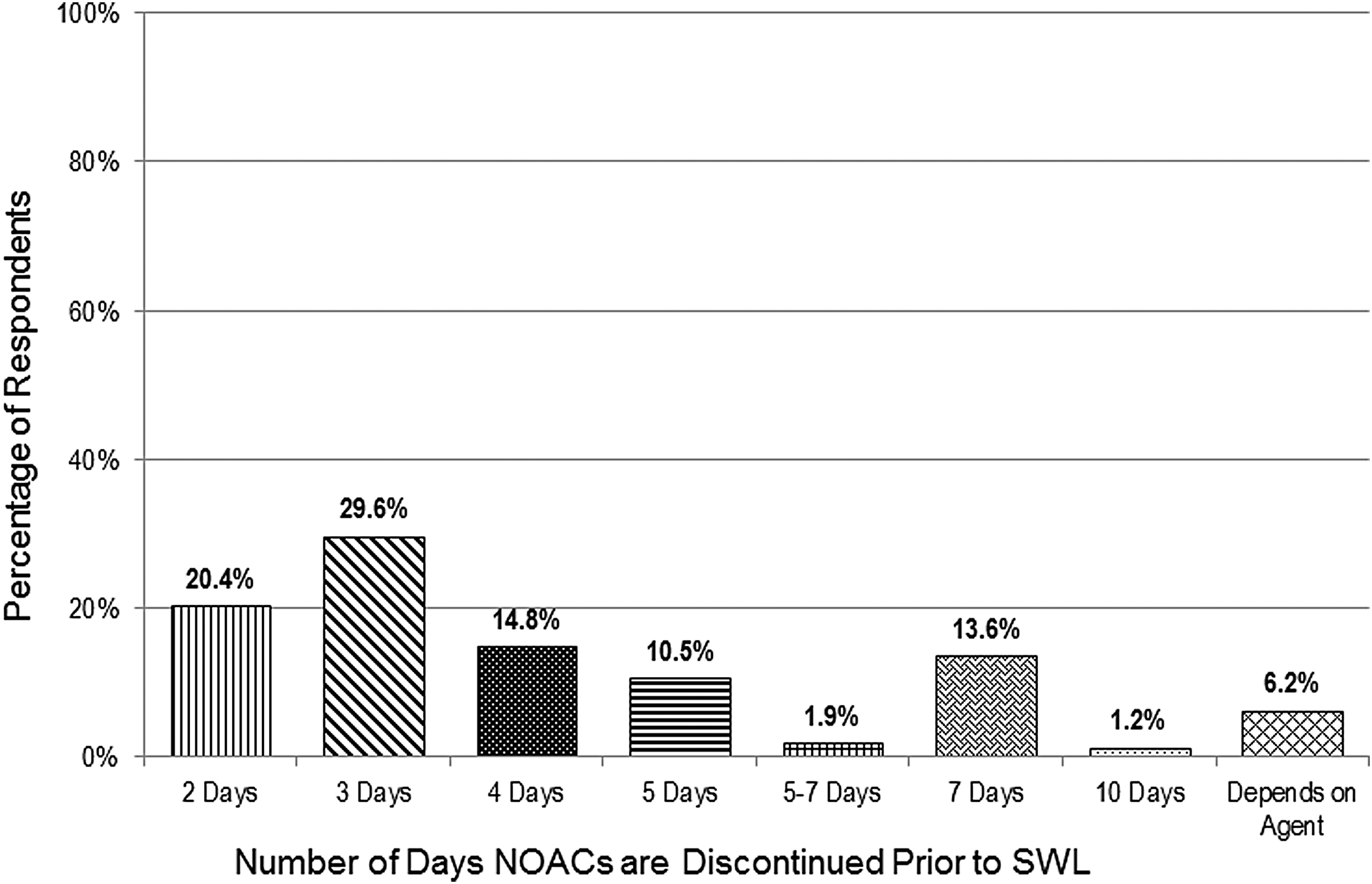
Frequency of survey responses classified by duration of NOAC discontinuation before SWL treatment. NOAC = new/novel oral anticoagulants; SWL = shockwave lithotripsy.
When responses were calculated based on the physician managing the preoperative discontinuation of the NOAC, 28.8% of urologists preferred 3 days, with 23.7%, 11.9%, and 13.6% preferring to hold it for 2, 4 and 7 days, respectively. When internal medicine, hematology, or cardiology handled the preoperative management, the majority (30.0%) also stopped them 3 days before SWL.
Surprisingly, different regimens were followed when responses were tabulated based on the urologists' continent of practice. In North America 35.2% of physicians surveyed preferred to hold the NOACs for 3 days. The preferred duration for European participants (36.6%) was to hold them for 2 days. Asian participants and those in South America preferred to hold the NOACs for 7 days pre-SWL 21.6% and 33.3%, respectively.
When the participants were asked who makes the decision on when the NOACs may be resumed after SWL, 64.2% of urologists preferred to manage this themselves. The remainder (35.8%) relied on other physicians (internal medicine, hematology, cardiology, or primary care physicians).
When urologists were queried on how many days after SWL NOACs were restarted, the majority (35.8%) preferred to do so when hematuria resolved. The remainder waited anywhere from 1 to 10 days (Fig. 3). When responses were reviewed based on who resumed the NOACs and when they were resumed post-SWL, similar responses were noted for urologists and nonurologists (Fig. 4).
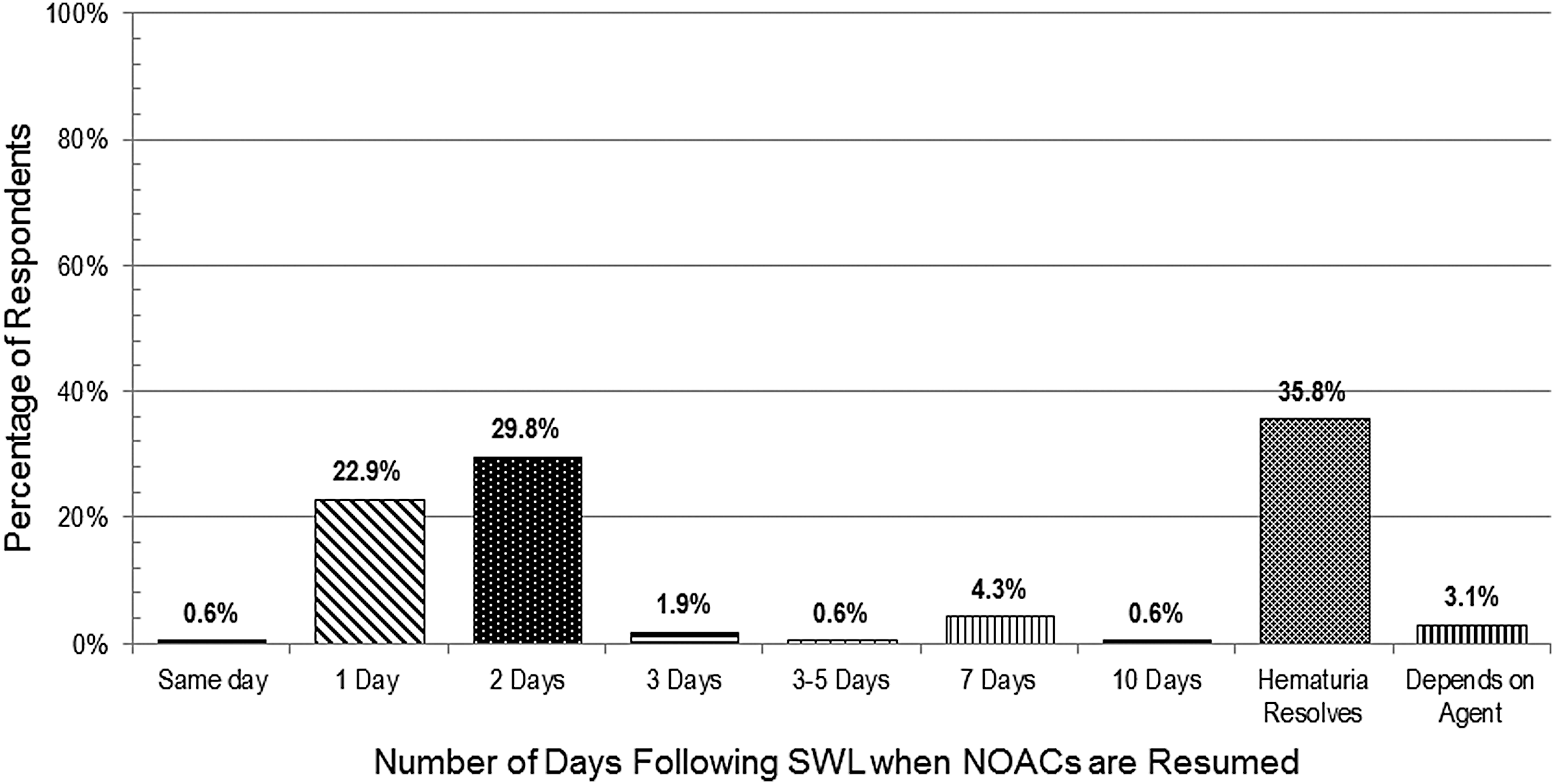
Frequency of survey responses classified by when NOAC medications are resumed after SWL treatment.
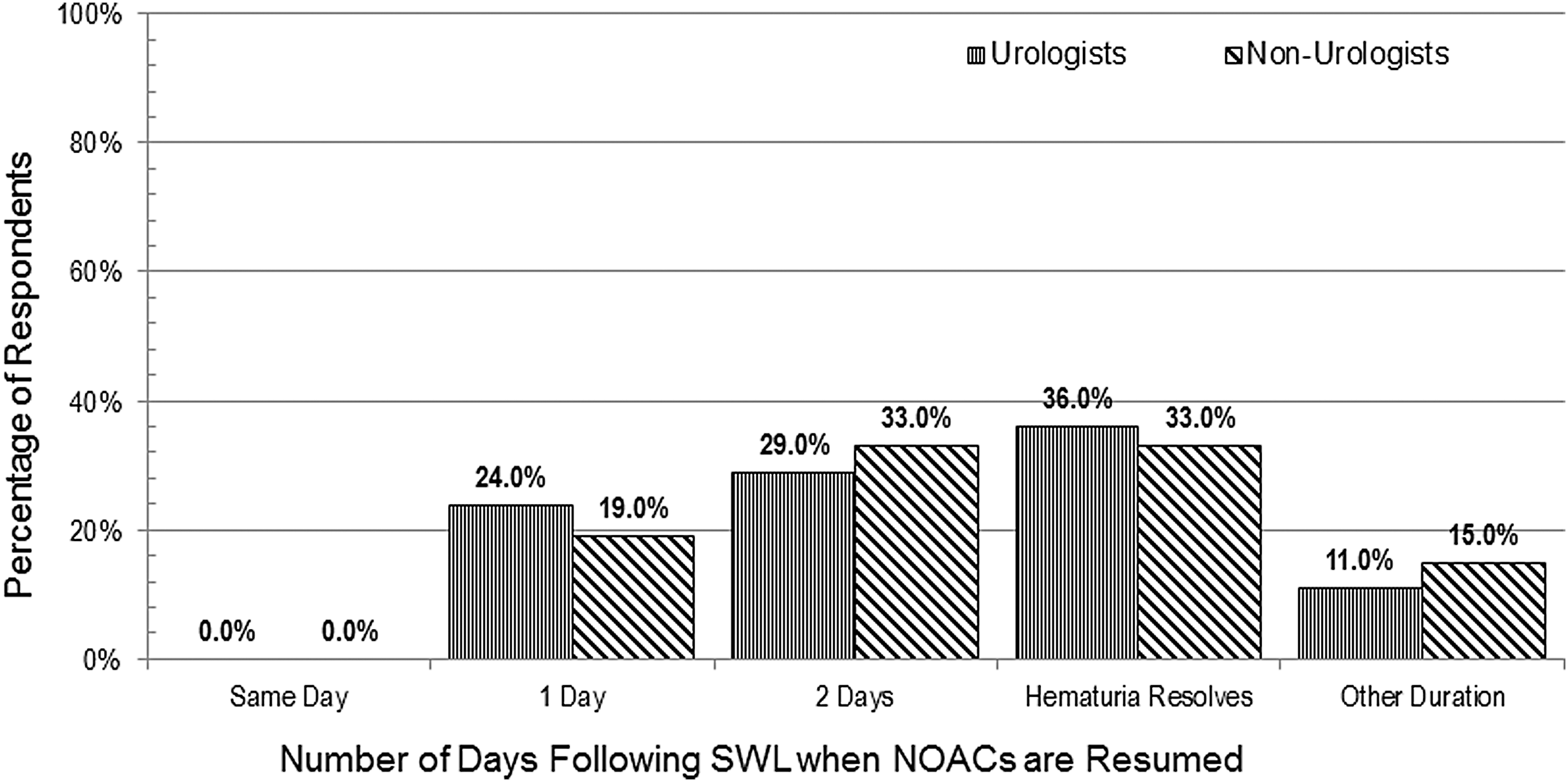
Frequency of survey responses classified by when NOAC medications are resumed after SWL treatment stratified by physician specialty.
When including data on the preferred pre- and post-SWL discontinuation of NOACs, the most common approach in 11.2% was to hold the NOACs 3 days before SWL and resume them 1 day after treatment.
Respondents were asked if they were aware of any adverse events such as perinephric hematomas or cardiovascular morbidity potentially related to the use or discontinuation of NOACs in patients undergoing SWL, but none were reported by any participant.
Discussion
The management of urologic patients on NOACs has become an everyday occurrence. Unfortunately, evidence-based guidelines are lacking on the optimal timing of discontinuation of these agents before and after SWL. The purpose of our survey was to determine whether there is consensus on how members of the Endourology Society manage this increasingly common clinical scenario.
The results of the survey are based on a small sample of Endourology Society members, but do include an international representation of stone experts. Although an 8% response rate raises questions about the possibilities of exclusion bias, we believe the rate of participation is in line with what is expected of e-mail-solicited, on-line surveys, where a 10% response rate is currently considered reasonable. 16
The majority of participants had been in practice for <10 years (55.5%) and therefore presumably had received some formal education in the pharmacology and clinical use of the NOACs. Seventy percent of respondents worked in academic clinical settings and had received formal Endourology fellowship training, suggesting some level of exposure to the clinical impact of NOACs on surgical stone management including SWL.
Of interest, almost one-half of those surveyed would not consider SWL if a patient was taking one of the NOACs. For patients on chronic anticoagulants, considering other treatment options instead of SWL has been suggested as a reasonable management strategy. 17 A number of case series have suggested anticoagulants do not need to be discontinued before ureteroscopy as bleeding risks are minimal. 9,18 –21 A more recent review of patients on anticoagulants including NOACs undergoing ureteroscopy however, did reveal a significant bleeding-related event rate of 15.4%. 22 Lower stone-free rates and higher hospital readmissions because of gross hematuria have also been reported after ureteroscopy when anticoagulants were not discontinued. 23
Our survey results suggest that the majority of urologists rely on their medical colleagues to manage the NOACs prelithotripsy. Remarkably, the duration of discontinuation was quite varied ranging from 2 to 10 days. Based on the specialist making the decision on when to stop the NOAC prelithotripsy, there seemed to be more variation among urologists. When reviewing the survey findings to this question based on continent, the North American and European practice was to discontinue the NOACs for a shorter length of time pretreatment compared with other regions of the world.
In contrast to the pretreatment management, the decision on postlithotripsy resumption of NOACs was more likely to be handled by urologists. The most common practice among respondents as to when the anticoagulants are restarted seems to be when hematuria resolves.
There are a number of limitations to this study that must be acknowledged. The small sample size does raise questions about the interpretation of our findings and whether they are generalizable to the broader urologic community. Approximately 70% of respondents had completed fellowship training in stones/endourology making them a select group with perhaps a greater interest and knowledge, or inherent bias. The responses therefore, might be different from those obtained had a more generalist urology physician population been surveyed. Despite these limitations, given the disparity in responses especially to the optimal time to hold NOACs preoperatively, the message seems to be that there is conflicting opinion and a lack of high-level evidence to assist urologists in their decision-making.
In addition, our survey did not specify stone location when asking respondents about their perioperative management of NOAC agents for SWL. This maybe an important factor to consider and could impact the chosen duration of NOAC discontinuation, depending on whether the stone was renal or ureteral in location.
Although our survey did query respondents regarding the occurrence of bleeding and thromboembolic complications related to the management of NOACs in patients undergoing SWL, our study was not designed to determine the incidence of these adverse events. However, it is interesting that no adverse events were reported by any of the survey respondents. Unfortunately, it is unlikely there will be randomized clinical trials assessing the various days of perioperative NOAC discontinuation in the SWL patient population because of the large sample sizes that would be required to demonstrate differences in important clinical outcomes. To date no studies have been performed assessing the safety of SWL in patients who are actively anticoagulated.
SWL is an effective and noninvasive treatment option for the management of urinary stone disease. However, the utilization of SWL in patients anticoagulated with NOAC medications, and the perioperative management of their anticoagulants, is highly variable among endourologists as demonstrated by our survey. To further increase the safety of SWL in this patient population, focused education regarding the pharmacology of the NOACs directed to urology trainees and those currently in practice is necessary. In addition, education of our nonurologist colleagues involved in the perioperative care of patients undergoing SWL is also required, specifically regarding the higher bleeding risk associated with SWL given the inability to obtain hemostasis during the procedure. Future efforts should focus on establishing specific guidelines regarding the perioperative management of NOAC medications for patients undergoing SWL using the highest level of evidence available.
Footnotes
Acknowledgements
We wish to acknowledge the Endourological Society for their assistance in the distribution of the survey, and Linda Nott for helping to prepare the manuscript.
Author Disclosure Statement
No competing financial interests exist.