
Abstract
Introduction and Objective:
Quality-based reimbursement continues to gain popularity as value-based care becomes more prominent. Our goal is to describe the impact of preoperative characteristics, intraoperative variables, and postoperative complications on the cost of robot-assisted laparoscopic radical prostatectomy (RALP).
Materials and Methods:
Using our institution's National Surgical Quality Improvement Program (NSQIP) data, we identified minimally invasive prostatectomies performed from January 2012 to March 2017. A retrospective chart review was done to collect perioperative data; financial data were collected from the business office.
Results:
Two hundred seventy-five patients were identified during this time period. Median total cost was $16,600 (interquartile range $15,100–$18,300), and median direct cost (DC) was $11,200 ($10,100–$12,400). Among preoperative characteristics, body mass index (BMI) ≥30 kg/m2, diabetes, hypertension, and blood urea nitrogen >21 were associated with increased DCs of $500, $500, $200, and $600, respectively (p < 0.05). American Society of Anesthesiologists (ASA) class III was associated with increased DC of $200 compared with ASA classes I–II (p < 0.05). Considering intraoperative characteristics, increasing operative times and estimated blood loss (EBL) were associated with increased DC (p < 0.001, p < 0.05, respectively). Occurrence of any postoperative complication was associated with increased DC of $1400 (p < 0.05). On multivariable analysis, a 1-U increase in BMI was associated with a $129 increase in DC (p < 0.001), a length of stay (LOS) greater than 3 days was associated with a $4099 increase in DC (p < 0.001), a 30-minute increase in operating room duration was associated with a $410 increase in DC (p < 0.05), any postoperative complication was associated with a $5397 increase in DC (p < 0.01), and treatment for diabetes was associated with a $1860 increase in DC (p < 0.05).
Conclusion:
BMI, diabetes, operative duration, EBL, LOS, and postoperative complications were associated with significantly increased DC of RALP. Understanding perioperative factors affecting cost contributes to understanding value in prostatectomy and improving quality in urologic care.
Introduction
As the climate of health care changes, the importance of improving value has become increasingly emphasized. Value in health care can be defined as the patient health outcomes per dollar spent. 1 With recent scrutiny on the increasing costs of health care, we have seen a shift from a fee-for-service-based system, which tends to promote an emphasis on quantity of care, to value-based payment systems, which emphasize quality of care. 2 For example, the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) promotes quality of care through the Merit-Based Incentive Payment System (MIPS) and Alternative Payment Models (APMs). 3
Within a value-based payment system, however, aggregating the total cost (TC) of care for a given medical condition or procedure may not always acknowledge cost variations across individual patients and medical conditions. 1 It is the clinician's responsibility to continue to deliver quality high-value care. To do so, we must continue to work on defining how these variations impact cost and how we can predict cost differences. Recent efforts by national organizations, including the American Urological Association (AUA), call for physicians to be leaders in initiating quality improvement. 4,5 The AUA Quality Improvement and Safety Committee summons urologists to develop quality improvement initiatives, including development and testing of physician performance measures. 5 We are now seeing an increase in data that help us better characterize quality and value across the field of urology. 6
Prostate cancer remains the most common nonskin cancer diagnosed in men in developed countries and is second only to lung cancer worldwide with over one million cases diagnosed yearly. 7 Radical prostatectomy continues to be the most common treatment for patients with clinically localized disease. 8 Minimally invasive techniques, including robot-assisted laparoscopic radical prostatectomy (RALP), offer similar cancer control, continence recovery, and sexual recovery outcomes along with the advantages of decreased blood loss, complication rate, length of stay (LOS), and length of sick leave compared with open approaches. 9 –11 Consequently, the use of RALP has risen from 13.6% of prostatectomies in 2003–2004 to 72.6% in 2011–2012. 12
Although cost–utility analysis has shown minimally invasive prostatectomy to be more expensive compared with the open technique in general, RALP continues to be the most widely used surgical technique. 12 More recent analyses have noted similar costs among high-volume surgeons and hospitals. 13 –15 At this point, while the cost differences between minimally invasive and open radical prostatectomy have been well described, there is a dearth of information on what perioperative factors influence cost. 16 Our study aims to define how preoperative, intraoperative, and postoperative variables impact the cost of RALP, with a goal to identify significant perioperative factors that can either be controlled to minimize cost or acknowledged as known factors influencing cost variation.
Materials and Methods
The Institutional Review Board at our institution approved this retrospective study. The local American College of Surgeons National Surgery Quality Improvement Program (ACS NSQIP) data were used to identify cases of RALP from January 1, 2012, to March 31, 2017, by the primary CPT code 55866. Over 30 preoperative patient variables were included, such as age, body mass index (BMI), laboratory values, and various comorbidities, including diabetes mellitus, tobacco use, dyspnea, chronic obstructive pulmonary disease, hypertension, steroid use, and bleeding disorders. The medical records were then reviewed to obtain biopsy results, surgical pathology (Gleason grading), gland size, pathologic staging (pT), estimated blood loss (EBL), use of lymph node dissection, and preoperative staging imaging. We categorized EBL into <200, 200–299, 300–399, and >400 mL groups. Information, including operative duration and American Society of Anesthesiologists (ASA) class, was ascertained from our institutional operating room (OR) database. Operative duration was defined as time from incision to completion of closure. Operative time was divided into the following categories: <210 minutes, 210–269 minutes, 270–329 minutes, and over 330 minutes. The ACS NSQIP database was used to obtain 30-day postoperative data, including hospital LOS and postoperative complications. A postoperative complication was defined as any of the following 30-day complications: superficial surgical site infection (SSI), organ/space SSI, sepsis/septic shock, transfusion, pneumonia, urinary tract infection (UTI), unplanned reintubation, mechanical ventilation >48 hours, cardiac arrest, myocardial infarction, cerebral vascular accident, pulmonary embolism, or deep venous thrombosis.
The institutional accounting system was used to obtain cost data for the hospital encounter during which the RALP took place (Allscripts EPSi, Chicago, IL). TCs were considered the sum of all costs for the encounter, and direct costs (DCs) were considered as any cost directly related to the patient, such as OR time, anesthesia time, bed occupancy, supplies, and nursing time.
Cost variables were compared by pre-, intra-, and postoperative variables using Mann–Whitney U tests for binary variables and Kruskal–Wallis tests for all other categorical variables. Linear regression models were used to compute unadjusted and adjusted effect estimates. Adjustment variables included BMI, diabetes, dyspnea, hypertension, blood urea nitrogen (BUN) >21, ASA class, and operative duration. All analyses were done using R programming language, version 3.5.0 (R Core Team, Vienna, Austria). Statistical significance was set at p < 0.05.
Results
Two hundred seventy-five patients were identified during the study period. Median TC across all prostatectomies was $16,600 ($15,100–$18,300) and median DC was $11,200 ($10,100–$12,400). Only DC will be discussed for the remainder of the results as DC and TC change in a linear manner. Variables significantly influencing cost are depicted in Figure 1.
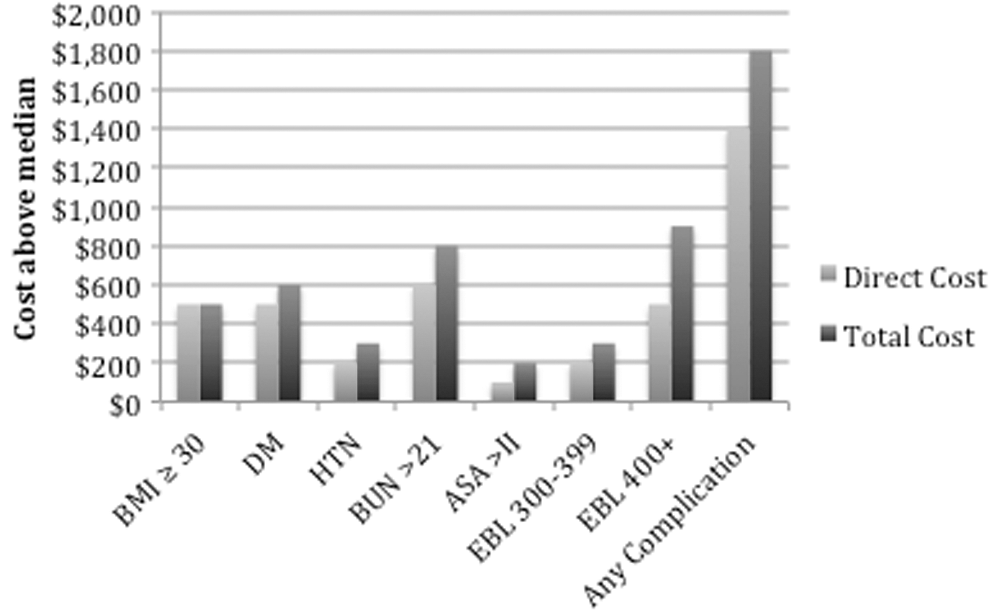
Variables significantly affecting cost in RALP, N = 275. RALP = robot-assisted laparoscopic radical prostatectomy.
Preoperative characteristics
The majority of patients were >55 years of age (84.4%). Over 40% (41.8%) of patients had BMI over 30 kg/m2 and those patients had significantly higher DCs by $500, p < 0.001. Fourteen percent of patients had a diagnosis of diabetes mellitus (DM) and 18.5% were smokers. Patients with DM had increased median DC by $500, p < 0.01. Over half (59.6%) had a diagnosis of hypertension and those patients had increased median DC of $200, p < 0.05. BUN >21 was also associated with a significantly higher DC by $600, p < 0.05. Forty-eight percent had ASA class of III, which was associated with $200 higher DC compared with ASA classes I–II, p < 0.05. Those preoperative patient characteristics in ACS NSQIP not significantly affecting cost parameters can be found in Table 1.
Preoperative Characteristics
All costs are in $1000s. N = 275.
p < 0.05; ** p < 0.01; *** p < 0.001.
ASA = American Society of Anesthesiologists; BMI = body mass index; BUN = blood urea nitrogen; COPD = chronic obstructive pulmonary disease; DC = direct cost; SGOT = serum glutamic-oxaloacetic transaminase; TC = total cost.
Intraoperative variables
Operative times of <210 minutes, 210–269 minutes, 270–329 minutes, and over 330 minutes had median DCs of $9700, $10,900, $11,900, and $13,200 in each group, respectively (p < 0.001). EBL of <200, 200–299, 300–399, and >400 mL had median DCs of $11,100, $11,000, $11,400, and $11,700 in each group, respectively (p < 0.05). Further prostate and cancer specifics, including gland size, Gleason grading, biopsy and surgical pathology, and tumor state, are listed in Table 2. Neither gland size nor differences in grade or stage had a significant impact on cost (Table 2).
Perioperative Characteristics
All costs are in $1000s. N = 275.
p < 0.05; ** p < 0.01; *** p < 0.001.
EBL = estimated blood loss; pT = pathologic staging.
Postoperative outcomes
Hospital LOS greater than 3 days was associated with a significantly increased DC by $1600. Twelve of the 275 patients (4.4%) experienced at least one postoperative complication, and those patients had increased DCs by $1400. Four patients experienced a deep SSI, and median DC for those patients was $12,300. Median DC for the four patients who received a blood transfusion was $13,000. Three patients developed a UTI; median DC was $12,600. Most other complications occurred only in one patient (Table 3).
Postoperative Outcomes
All costs are in $1000s. N = 275.
p < 0.05; ** p < 0.01; *** p < 0.001.
CVA = cerebral vascular accident; DVT = deep venous thrombosis; LOS = length of stay; MI = myocardial infarction; SSI = superficial surgical site infection; UTI = urinary tract infection.
Multivariable analysis
Change in DC for each 1-U change in BMI was $129 (p < 0.001). Adjusted increase in DC for LOS longer than 3 days was $4099 (p < 0.001). For each 30-minute increase in OR duration, DC increased by $410 (p < 0.05). Any postoperative complication increased DC by $5397 (p < 0.01). Patients with diabetes had increased DC by $1860 (p < 0.05). There was no significant change in DC per 100-U increase in EBL, for ASA class >III, or for patients with hypertension (Table 4).
Regression Results
Adjusted and unadjusted results along with 95% CIs are reported. N = 275.
p < 0.05; ** p < 0.01; *** p < 0.001.
CI = confidence interval; OR = operating room.
Discussion
The goal of this study was to identify patient-specific variables influencing cost of RALP. Our results highlight increased costs in patients with multiple comorbidities, including DM and obesity. Intraoperative factors, including operative duration, also significantly increased costs. Postoperatively, our results highlight increased costs secondary to a prolonged LOS or any surgical complication.
Given the dearth of studies on RALP, addressing cost of preoperative factors at a granular lever, we looked to other procedures for comparison. Cost analyses in other specialties have demonstrated increased cost associated with preoperative factors such as medical comorbidities. For example, preoperative diagnoses of DM, hypertension, and increased ASA class were found to significantly increase cost in ventral hernia repairs. 17 Obesity also increased TC of total hip arthroplasty by $500 per each 5-U increase in BMI. 18 Interestingly, BMI has not previously been found to incur an additional financial burden for RALP in other studies. 19,20 However, our data show a $129 increase in cost for each 1-U increase in BMI on multivariable analysis. Additionally, carrying a diagnosis of DM increased adjusted DC by $1860. A multispecialty study of greater than 5000 patients concluded that preoperative risk factors, including medical comorbidities, were more predictive of cost than postoperative complications. 21 Our data suggest that DM and obesity substantially increase cost of RALP on multivariable analysis, further supporting the hypothesis that complex patients incur more expensive surgical care.
Intraoperative variables impacting cost have been examined before the widespread adoption of RALP. One study from 2001 showed that factors significantly influencing cost in retropubic radical prostatectomy included increasing operative times, EBL, and units of blood transfused. 22 Bolenz et al. examining costs associated with RALP also noted increased cost with longer operative time, placement of drains, and requirement of blood transfusions. 20 Similarly, our data reveal significant cost increase with increasing operative duration and EBL in the univariable analysis and OR duration in the multivariable analysis. Although prostate gland size has previously been associated with increased operative times, 23,24 our data do not show any impact of prostate gland size or tumor pathologic grade and stage on cost. This is consistent with data from other studies and may indicate only a minor impact of gland size on operative time and therefore cost. 20
Postoperative complications are well known to increase costs across specialties. 17,20,21 The costs of complications at academic institutions have been estimated to approximate $6,000,000 on an annual basis. 21 Postoperative complications following minimally invasive partial nephrectomy have been shown to incur a significant increase in cost by almost $5000. 25 Our complication rate was ∼4.4%, and the presence of any complication increased DCs by $5397 on multivariable analysis. Hospital LOS is another well-known driver of cost increase. 11,20 Our data reveal an adjusted $4099 increase in DCs for patients with LOS greater than 3 days. However, LOS may be influenced by patient complexity and complication rate. Focusing instead on variables that impact LOS may offer more significant avenues for cost reduction, and quality improvement projects aiming to reduce LOS and complications have the potential to significantly affect cost.
Much of the available literature analyzing the cost of prostatectomy focuses on the increased cost burden of use of robotics when compared with open techniques. 13,16,26 A 2018 analysis using data from the Laparoscopic Prostatectomy Robot Open clinical trial determined that RALP was associated with a cost increase of $3837 compared with radical retropubic prostatectomy. 11 The study also noted that much of the cost variation was dependent on other factors, including operative times, robot maintenance, and sick leave. Regardless, the clinical benefits of RALP as well as market pressures have led to its rapid adoption as the most common treatment option for clinically localized disease. 12 However, there are little data defining specific preoperative factors influencing cost of RALP as aforementioned factors that have been associated with increased cost were largely intraoperative and postoperative. Interestingly, no preoperative variables such as medical comorbidities have been previously shown to have a significant influence on cost, which is contrary to our findings. 20
As payment strategies evolve toward value-based care, we need to continue to gather data to help us understand outcomes in relation to cost. Improved outcomes, decreased cost, or both will improve value. In oncologic surgery, it is difficult to modify preoperative risk factors contributing to medical complexity due to the necessity of timeliness in treatment. However, we can use this information in predicting the cost for prostatectomy. These data provide insight into how variations between patients result in significant cost differences. We propose that information provided in this study and data from similar studies can be used as we develop a bundled payment model for RALP, which accounts for variations in patient complexity and takes into account the cost burden of postoperative complications. Failure to provide a method for risk stratification may incentivize providers to selectively choose lower risk patients, leaving a negative impact on providers willing to care for high-risk patients.
There are multiple limitations to this study. This analysis included patients from a single institution, and thus the cost metrics may be specific to this institution. In addition, complications and intraoperative characteristics were not adjusted by surgeon. Our data are also limited to the single hospital encounter at the time of surgery and 30-day complication data. This does not include delayed factors such as frequency of outpatient visits, length of sick leave, cost of travel, and cost of adjuvant treatment for complications or further cancer treatment. Without these data, we are limited in estimating true costs to society.
Our study has several strengths as well. Cost was used rather than charge data to more accurately represent resources. Indirect costs, DCs, and profit margins all contribute to charge data and are subject to institution-specific variables. Therefore, they may be artificially elevated and introduce bias to the data. This study reflects a large group of patients, examined in a granular manner by using ACS NSQIP data, thus allowing for comparison across multiple cost variables from the finance office.
Conclusions
BMI, diabetes, operative duration, and postoperative complications significantly affect cost in RALP. Improved understanding of cost-influencing variables will allow for better quantification of the value we deliver in prostatectomy. With the data presented here, we can increase value through modification of perioperative variables that we know influence cost. Defining cost variables can also aid in development of appropriate bundled payment models.
Footnotes
Author Disclosure Statement
No competing financial interests exist.