
Abstract
Introduction:
Institutional studies suggested that tumor size (TS) might be an independent predictor of recurrence after local tumor ablation (LTA). However, limited data exist to ascertain whether a larger TS may also predispose to a worse cancer-specific mortality (CSM) rate.
Materials and Methods:
Patients treated with LTA for T1a nonmetastatic renal-cell carcinoma were identified within the Surveillance, Epidemiology, and End Results (SEER) database (2004–2015). Estimated annual percentage change (EAPC) methodology, cumulative incidence plots, and multivariable competing risk regression (CRR) models before and after the 1:1 ratio propensity score (PS) adjustment were used to compare LTA for TS ≤30 mm vs TS >30 mm. A comparison of cryosurgery vs thermal ablation according to TS was also performed.
Results:
Of 3946 LTA patients, 2974 (75.3%) patients harbored TS ≤30 mm vs 972 (24.7%) harbored TS >30 mm. The latter was significantly older (median age 67 years vs 71 years, p < 0.001), compared with TS ≤30 mm. No differences were recorded in annual rates over time. In unmatched CRR models, after adjustment for other-cause mortality (OCM) rate, LTA for TS >30 mm showed a worse 5-year CSM rate (hazard ratio [HR] 2.3, p < 0.001), relative to TS ≤30 mm. In PS- and OCM rate-adjusted CRR models, LTA for TS >30 mm still showed a worse 5-year CSM rate (HR 2.86, p < 0.001), relative to TS ≤30 mm. Thermal ablation was associated with a higher 5-year CSM rate, compared with cryosurgery (7.6% vs 3.9%, p = 0.02), but only when TS was >30 mm.
Conclusions:
TS >30 mm is an independent predictor of higher 5-year CSM rates in patients treated with LTA, even after adjustment for OCM rate. In consequence, when LTA is considered, it ideally should be performed for TS ≤30 mm.
Introduction
In the last two decades, ablative techniques (local tumor ablation [LTA]) emerged as a treatment option for management of renal masses, especially in the elderly and/or patients with comorbidities. 1,2 Existing reports do suggest that tumor size (TS) is a significant predictor of oncologic outcomes after LTA, with good results for masses up to 30 mm. 1,3
However, these data originate from institutional retrospective series 4 –9 with small sample sizes (range from 627 to 168 patients 8 ), where oncologic outcomes were mostly evaluated as recurrence-free survival (RFS). Moreover, some of these studies 5,6 also included T1b renal-cell carcinoma (RCC). Only one population-based study 10 relying on the Surveillance, Epidemiology, and End Results (SEER) database (2004–2013) assessed 5-year cancer-specific survival (CSS) rates according to TS in a cohort of 3052 LTA patients. However, the prognostic role of TS on survival outcomes was not assessed.
Based on this evidence, European guidelines 11 suggest that definitive conclusions regarding oncologic outcomes of LTA according to TS cannot be drawn. Conversely, the 2019th North American guidelines 12 recommend LTA for lesions less than 3 cm, based on the potential for higher recurrence above this threshold.
Despite this recommendation, existing data regarding LTA are of limited robustness, especially for renal masses in excess of 3 cm. In consequence, we tested for differences in cancer-specific mortality (CSM) rates after LTA according to TS ≤30 mm vs >30 mm. We hypothesize that LTA for TS >30 mm may result in higher CSM rates in T1a RCC, even when the other-cause mortality (OCM) rate is accounted for. To test this hypothesis, we relied on propensity score (PS) matching and competing risk regression (CRR) models within the SEER database (2004–2015).
Materials and Methods
Data source and patient selection
Within the SEER database (2004–2015), we focused on patients aged 18 years or older treated with LTA, as primary treatment, with histologically confirmed T1a RCC (International Classification of Disease for Oncology [ICD-O] site codes C64.9). LTA was coded according to the SEER coding manual 13 and only cryosurgery (surgery code 13 and 23) and thermal ablation (surgery code 15) were included. Death was defined according to the SEER mortality rate code, as either CSM rate (CSM rate, death from RCC) or OCM rate (death from any other causes). All autopsies and death certificates, as well as missing follow-up data, were excluded.
Patients were stratified according to TS ≤30 mm and TS >30 mm. These selection criteria yielded 3946 assessable patients.
Statistical analyses
Statistical analyses consisted of six analytical steps. First, we evaluated overall rates of LTA for TS ≤30 mm and TS >30 mm and we tested for statistically significance differences in means and proportions. Second, we examined the estimated annual percentage changes (EAPCs) 14 for TS ≤30 mm and TS >30 mm, as well as according to LTA type in each TS group. Third, cumulative incidence plots depicted CSM and OCM rates according to both TS and LTA type; the statistical significance of differences was tested with the Gray test. 15 Fourth, multivariable CRR models 16 predicted CSM and OCM rates according to TS (≤30 mm vs >30 mm). Adjustment variables consisted of age at diagnosis, histology, Fuhrman grade, gender, marital status, and ethnicity. Fifth, survival analyses were repeated after 1:1 PS matching according to the nearest neighbor. 17 The PS-matched cohorts (LTA for TS ≤30 mm vs TS >30 mm) were balanced according to age at diagnosis, gender, ethnicity, socioeconomic status, population density, period of treatment, histology, and Fuhrman grade. Finally, we generated a graphical depiction of HRs reported within previous institutional retrospective studies, 4 –6,8,9 focused on RFS in LTA-treated patients for TS ≤30 mm vs TS >30 mm 4,5,8 and TS <30 mm vs TS ≥30 mm. 6,9
All statistical tests were two sided with a level of significance set at p < 0.05. Analyses were performed using the R software environment for statistical computing and graphics (version 3.4.1;
Results
Sociodemographic and tumor characteristics of the overall population
Of 52,001 patients with T1a nonmetastatic RCC, 4578 patients (8.8%) were treated with LTA. Of these, 3946 patients treated with either cryosurgery (3028, 76.7%) or thermal ablation (918, 23.3%) were included in this study.
Table 1 summarizes baseline characteristics of the study population. Overall, 972 (24.7%) patients were treated with LTA for TS >30 mm. Compared with those with TS ≤30 mm, patients treated with LTA for TS >30 mm were significantly older (median age at diagnosis 67 years vs 71 years, p < 0.001), more frequently male (62.0% vs 68.8%, p < 0.001), and more frequently in the highest socioeconomic quartiles (71.6% vs 75.2%, p = 0.03). No other sociodemographic characteristic differences were recorded. LTA type (cryosurgery vs thermal ablation) was evenly distributed in patients with TS ≤30 mm (76.4% vs 23.3%, respectively) and TS >30 mm (77.7% vs 22.3%, respectively). Patients treated for TS >30 mm more frequently harbored clear cell histology (53.7% vs 57.9%, p < 0.001), compared with those treated for TS ≤30 mm. No significant differences were recorded in Fuhrman-grade distribution.
Baseline Characteristics of 3946 Patients with T1a Renal-Cell Carcinoma Treated with Local Tumor Ablation for Tumor Size ≤30 mm (2974) or Tumor Size >30 mm (972), Identified Within the Surveillance, Epidemiology, and End Results Database from 2004 to 2015
Temporal trend analyses
In the overall population, no statistically significant differences over time were recorded for both LTA for TS ≤30 mm (from 71.7% to 74.9%; EAPC +0.6%, p = 0.08) vs LTA for TS >30 mm (from 28.3% to 25.1%; EAPC −1.9%, p = 0.06) (Fig. 1A).

Annual rates over time of patients with T1a nonmetastatic RCC treated with LTA for either tumor size ≤30 mm and tumor size >30 mm
In LTA for TS ≤30 mm cohort, both cryosurgery (EAPC +0.4%, p = 0.47) and thermal ablation (EAPC +1.3%, p = 0.26) remained stable over time (Fig. 1B). In LTA, for the TS >30 mm cohort, cryosurgery remained stable over time (EAPC −0.6%, p = 0.46). Conversely, thermal ablation rates decreased over time (from 9.1% to 6.2%, EAPC −6.9%, p = 0.02) (Fig. 1C).
Survival analyses of unmatched cohort
In the overall unmatched cohort, cumulative incidence plots showed 5-year CSM rates of 2.0% vs 4.7% (p < 0.001) and 5-year OCM rates of 7.0% vs 13.7% (p < 0.001), respectively, for LTA for TS ≤30 mm and TS >30 mm (Fig. 2A). In unadjusted multivariable CRR models (“a” in Table 2), TS >30 mm independently predicted higher CSM (HR 2.3, p < 0.001) and higher OCM (HR 1.81, p < 0.001) rates, relative to TS ≤30 mm. In addition, older age (HR 1.07, p < 0.001), never married status (HR 1.98, p = 0.04), and Fuhrman grade G3/G4 (HR 2.21, p = 0.04) independently predicted higher 5-year CSM rates.
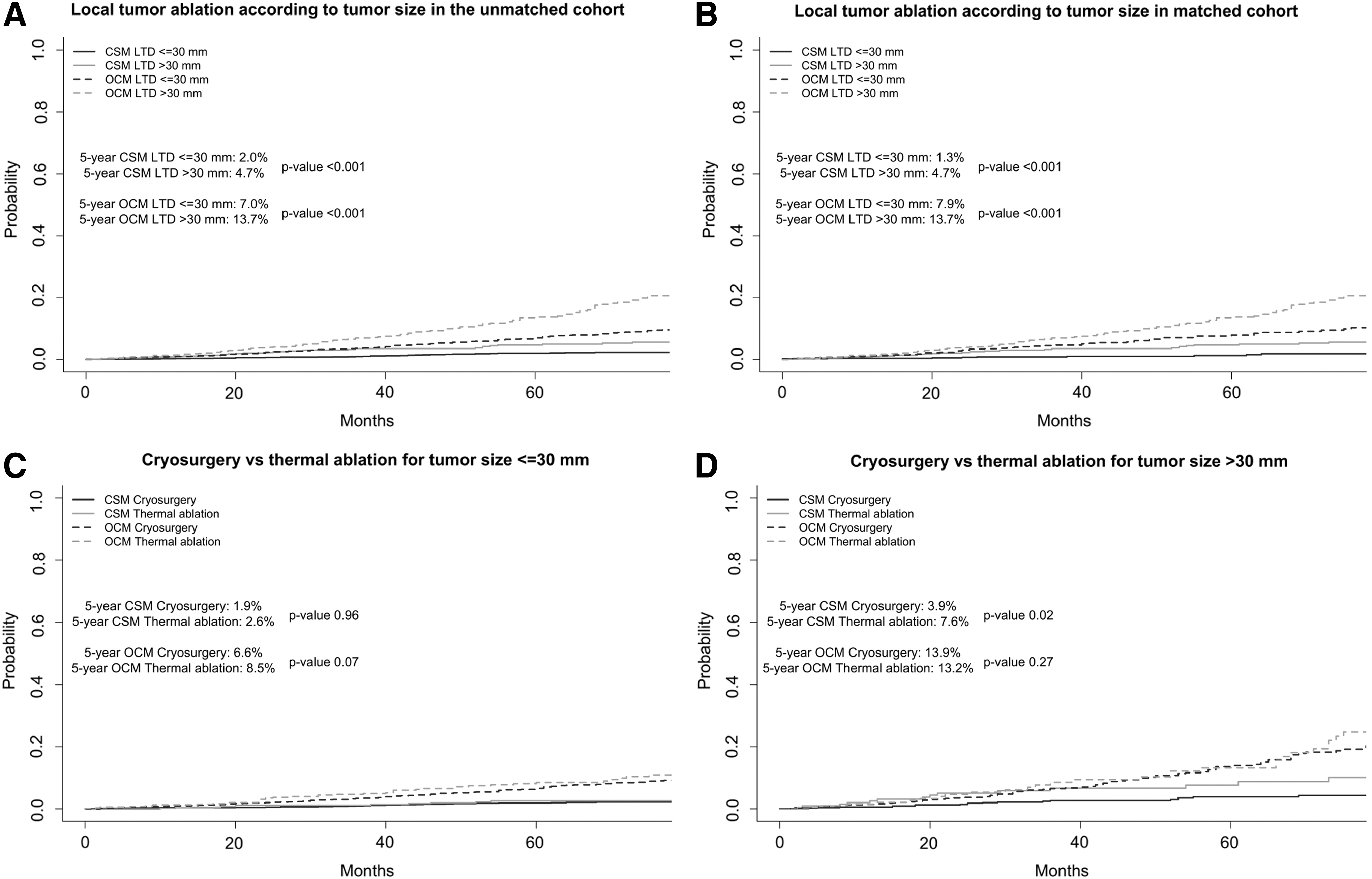
Cumulative incidence plots depicting CSM and OCM rates in T1a nonmetastatic RCC patients treated with LTA for either tumor size ≤30 mm and tumor size >30 mm, in the unmatched
Multivariable Competing Risk Regression Models Before (a) and After (b) 1:1 Propensity Score Match Predicting Cancer-Specific Mortality Rate and Other-Cause Mortality Rate in T1a Renal-Cell Carcinoma Treated with Local Tumor Ablation for Either Tumor Size ≤30 mm or Tumor Size >30 mm
Bold type indicates significant p values.
HR = hazard ratio; LTA = local tumor ablation.
In LTA, for the TS ≤30 mm cohort, cumulative incidence plots showed 5-year CSM rates of 1.9% vs 2.6% (p = 0.96) and 5-year OCM rates of 6.6% vs 8.5% (p = 0.07), respectively, for cryosurgery and thermal ablation (Fig. 2B). Conversely, in LTA for the TS >30 mm cohort, cumulative incidence plots showed 5-year CSM rates of 3.9% vs 7.6% (p = 0.02) and 5-year OCM rates of 13.9% vs 13.2% (p = 0.27), respectively, for cryosurgery and thermal ablation (Fig. 2C).
Survival analyses of PS-matched cohort
After 1:1 ratio PS matching, 972 LTA for TS ≤30 mm and 972 LTA for TS >30 mm remained for the purpose of subsequent analyses. No baseline differences were recorded between both cohorts after PS matching.
Cumulative incidence plots showed 1.3% vs 4.7% 5-year CSM rates (p < 0.001) and 7.9% vs 13.7% OCM rates (p < 0.001), respectively, for LTA for TS ≤30 mm and TS >30 mm (Fig. 2D).
In PS-adjusted multivariable CRR models (“b” in Table 2), TS >30 mm independently predicted higher CSM (HR 2.86, p < 0.001) and higher OCM (HR 1.86, p < 0.001) rates, relative to TS ≤30 mm. Moreover, older age (HR 1.05, p < 0.001) and Fuhrman grade G3/G4 (HR 3.8, p = 0.02) were independent predictors of higher 5-year CSM rates.
Graphical depiction of hazard ratios of previous studies
Graphical depiction of hazard ratios for cancer recurrence after LTA in previous institutional studies (Fig. 3) showed an almost fivefold increase in recurrence rates after LTA for either TS >30 4,5,8 or TS ≥30 mm. 6,9

Graphical depiction of the current HRs relative to those reported within the previous institutional retrospective studies, focused on RFS in patients treated with LTA for tumor size ≤30 mm vs >30 mm and tumor size <30 mm vs ≥30 mm. HRs = hazard ratio; RFS = recurrence-free survival.
Discussion
We relied on the SEER database (2004–2015) to test the hypothesis that LTA for TS >30 mm may result in higher CSM rates in T1a RCC, even when the OCM rate is accounted for. Our analyses represent the first population-based study that investigated this topic. As opposed to previous institutional series, our study relied on a substantially larger sample size and more contemporary patients. Moreover, it relied on PS matching and CRR models and resulted in several noteworthy findings.
First, less that 10% (4578 out of 52,001) patients with nonmetastatic T1a RCC were treated with LTA within the SEER database. In our cohort of 3946 LTA patients, the majority of these individuals (75.3%) harbored TS ≤30 mm, while one-quarter (24.7%) harbored tumors >30 mm. The latter was significantly older (median age at diagnosis 67 years vs 71 years, p < 0.001). These findings are in agreement with guidelines that recommend LTA as a treatment option for small renal masses and/or in elderly patients. 11,12
Second, survival analyses showed a significantly higher CSM rate in patients with TS >30 mm (4.7% vs 2.0% and 4.7% vs 1.3%, in an unmatched and matched population, respectively), which was validated in CRR models (2.86-fold increase). In addition, patients with TS >30 mm also experienced significantly higher OCM rates compared with those with TS ≤30 mm (13.7% vs 7.0% and 13.7% vs 7.9%, in an unmatched and matched population, respectively), validated in CRR models (1.86-fold increase). Higher OCM rates, as well as older age of LTA patients with TS >30 mm, indicate that clinicians give higher priority, for LTA with TS >30 mm, to patients at higher risk of OCM rate. To the best of our knowledge, no other studies examined the concept of OCM rate after LTA. Moreover, all other institutional studies 4 –8 relied on RFS and/or disease-free survival (DFS) as endpoints also without adjustment for OCM rate. In all five institutional studies, 4 –8 RFS and DFS are higher for TS greater than or equal to 30 mm. Our graphical depiction of HR of these studies showed an almost fivefold increase of recurrence, while our analyses showed a 2.86-fold increase in CSM rate for TS >30 mm. Even though different endpoints were used, our findings are highly consistent with the analyses on earlier endpoint (recurrence).
Third, CSM rates after thermal ablation were higher for TS >30 mm, compared with cryosurgery (7.6% vs 3.9%, p = 0.02). Conversely, no CSM rate difference was identified according to LTA type for TS ≤30 mm. In consequence, cryosurgery should represent the preferred option for LTA in patients with TS >30 mm. Our findings are in agreement with a historical meta-analysis, 18 where higher local progression rates were reported for thermal ablation compared with cryosurgery. Conversely, a more recent pooled analysis 19 reported similar proportions of clinical efficacy (described as no evidence of recurrence on imaging) for thermal ablation vs cryosurgery. However, the heterogeneity of the studies imposes interpretation of these results with caution.
Taken together, our findings validate the NCCN recommendation regarding use of LTA in patients with TS <30 mm. Second, a minority of patients are treated with LTA for TS >30 mm. In general, these individuals are older and at substantially higher risk of OCM rate. These characteristics may justify LTA use above the recommended TS threshold. Nonetheless, the CSM rate in LTA-treated patients for TS >30 mm was 2.8-fold higher than in their counterparts treated for TS ≤30 mm. This observation should be considered in clinical decision-making and at informed consent before LTA for TS >30 mm.
Despite its strengths, the limitations of this study include its retrospective nature, absence of comorbidity information, lack of standardized specimen handling as well as of central review regarding histologic subtype, and lack of data regarding earlier cancer control endpoints, such as local recurrence and disease-free survival. Nonetheless, our analyses relied on PS matching to maximally reduce biases and on CRR models adjusted for OCM rate.
Conclusions
TS >30 mm is an independent predictor of higher 5-years CSM rates in patients treated with LTA, even after adjustment for the OCM rate. In consequence, when LTA is considered, it ideally should be performed for TS ≤30 mm.
Footnotes
Author Disclosure Statement
No competing financial interests exist.