
Abstract
Introduction and Objectives:
Ureteral injuries can occur during ureteral access sheath (UAS) deployment. The force exerted during deployment and the amount of force that results in ureteral injury is yet to be accurately quantitated. In this feasibility study, we developed and then tested a novel force-sensing device in our animal laboratory to identify the threshold force that results in a porcine ureteral injury.
Methods:
With Institutional Animal Care and Use Committee approval, we measured ureteral dilator and UAS deployment force using our proprietary University of California, Irvine Ureteral Access Sheath Force Sensor (UAS-FS). The exerted force was measured during deployment from the moment that the tip of the UAS was passed into the urethral meatus until it reached the renal pelvis; progression of the UAS along the ureter was monitored with fluoroscopy. Ureteroscopic evaluation was performed after deployment of each catheter/sheath ≥8F to assess for ureteral injury using the Postureteroscopic Lesion Scale (PULS).
Results:
Six juvenile Yorkshire female pigs (12 ureters) were studied. No injuries were detected when the deployment force was <4 Newtons (N), which was the case when the catheter/access sheath was ≤13F. Increasing UAS size >13F resulted in greater peak forces. In five of the pigs, ureters selected for 14F UAS deployment without previous sequential dilation were injured (PULS ≥3) at a mean threshold force of 4.84 N. Serial dilation had a higher threshold for PULS ≥3 at 5.56 N. Overall, injury of PULS ≥3 was routinely noted when the force applied exceeded 8.1 N.
Conclusions:
The UAS-FS reliably measured forces while deploying a UAS. Significant ureteral injury can routinely be avoided if the applied force is <4.84 N; PULS ≥3 routinely occurred when forces exceeded 8.1 N. Serial dilation may allow safe passage at higher deployment forces, as much as 5.56 N.
Introduction
Flexible ureteroscopy (URS) has become the gold standard for definitive management of small ureteral and renal calculi. 1,2 The ureteral access sheath (UAS) was developed to safely facilitate the repeated passage of the flexible ureteroscope into the proximal ureter and kidney. 3,4 In addition, use of the UAS is associated with decreased intrarenal pressure, 5 –7 improved stone-free rates, 8,9 reduced operative time, 8,10 and less ureteroscopic repair costs. 11,12
Although the UAS has undergone design modifications to improve its deployment 13 –15 (e.g., size variation, change in sheath construction to reduce buckling and kinking, and a hydrophilic coating), ureteral injury secondary to its deployment continues to be of concern. 16 A study by Traxer and Thomas estimated the incidence of UAS-induced ureteral injury to be as high as 48%, with serious injuries (i.e., ureteral perforation/splitting) noted in 13%. 17 An established threshold of application force and a method of real-time force measurement during UAS deployment could markedly improve the safety of UAS deployment during routine URS.
In an effort to characterize the forces exerted upon the ureteral wall during UAS deployment, we created a novel load-sensing device, the Ureteral Access Sheath Force Sensor (UAS-FS) at the University of California, Irvine (UCI). We hypothesized that the UAS-FS would allow us to measure the forces applied to the sheath and ureter and define a safe range of forces and a threshold force beyond which UAS-induced ureteral injury would likely occur.
Methods
UAS-FS development
Development of the UAS-FS (Fig. 1) was a collaborative effort between the UCI Department of Urology and faculty at the UCI California Institute of Telecommunications and Information Technology. The device is designed for sterile use in the operating room during endoscopic procedures in which a UAS is used. An internal load cell is used as a strain gauge to measure input force during UAS deployment; it is calibrated using a 200 g weight. A guidewire is passed through the dock connected to the device that allows for the coupling between the distal end of the UAS and UAS-FS. The surgeon holds the device and propels the UAS toward the kidney over the guidewire while the sensor simultaneously indicates the applied force by color (from green to yellow to red) and by an audible signal (increasing sound intensity and frequency). The device also transmits force data, in Newtons (N), to a tablet Android device loaded with proprietary software developed by the UCI Department of Engineering. The transmission occurs through Bluetooth technology, thereby providing for continuous wireless data collection throughout deployment of the UAS.
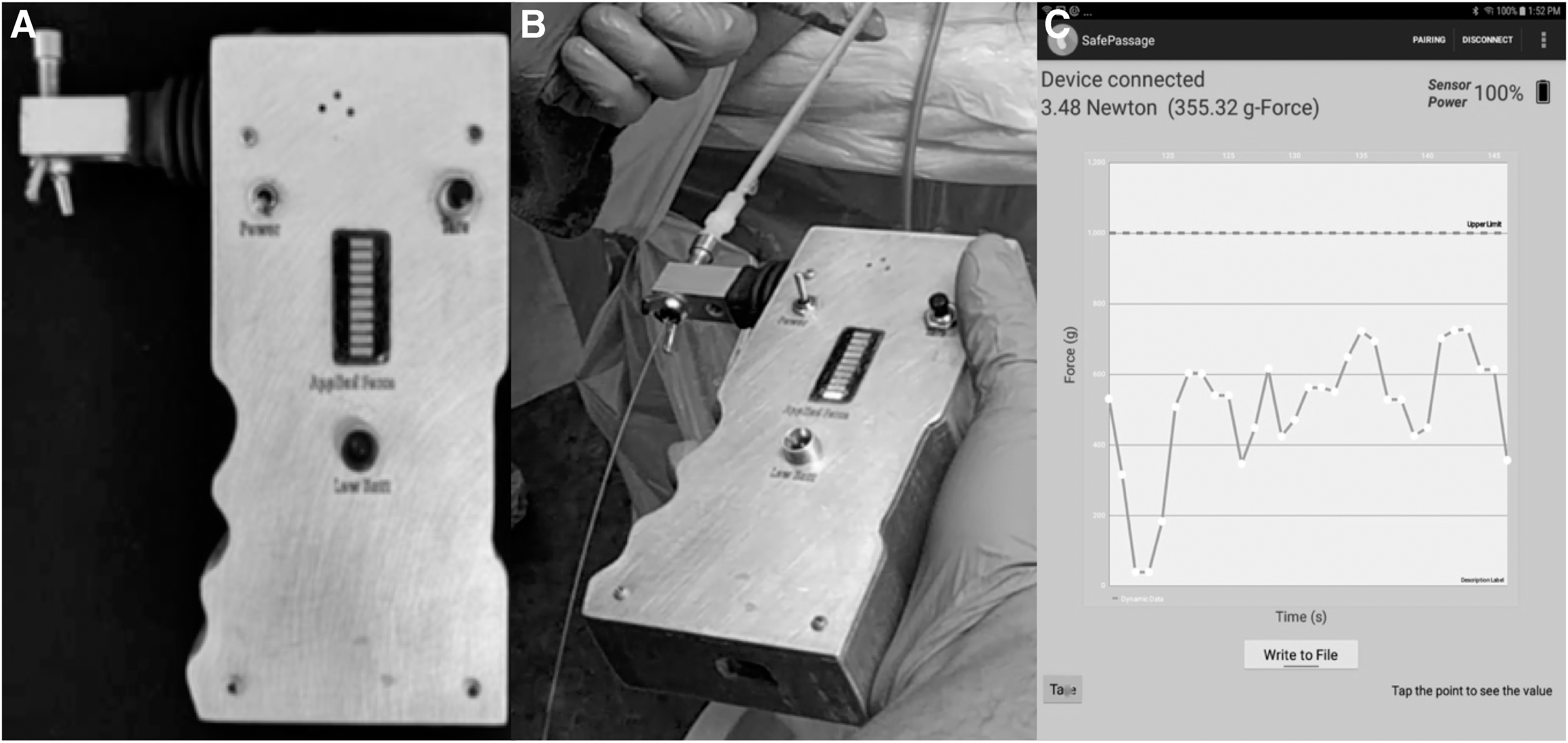
Ureteral access sheath force sensing device and screenshot of software printout.
Animal preparation
After approval by the Institutional Animal Care and Use Committee, six juvenile Yorkshire female pigs were entered into the study. The animals were initially administered xylazine (2 mg/kg) intravenously. Then, the pigs were oriented in the supine position and isoflurane (1.5%) was administered by inhalation throughout the procedure. Vital signs, temperature, and muscle tone were continuously monitored throughout the procedure as per the Guide for the Care and Use of Laboratory Animals.
Preliminary ureteral access
The perineum was prepared with povidone–iodine solution and standard drapes were applied. A 15F flexible cystoscope (Karl Storz, Germany) was introduced into the urethra and a 0.035″ guidewire (Amplatz Super Stiff™ Guidewire; Boston Scientific, Marlborough, MA) was placed into the ureteral orifice and fluoroscopically guided to the kidney (vide infra).
Ureteral dilator, access sheath deployment force measurement, and assessment of ureteral damage
A single surgeon (K.S.K.) performed all ureteral dilator and UAS deployments over the guidewire using the UAS-FS. Force measurement was initiated with the UAS tip at the urethral meatus and stopped when the UAS had reached the renal pelvis; each deployment was carried out under pulsed fluoroscopic guidance (4 pulses/s). The initial ureter was randomized to either serial or nonserial dilation; the contralateral ureter then received the approach that was not used for the initial ureter. For serial dilation, measurements were recorded using serially passed ureteral dilators (6F, 7.5F, 8F, and 9F) followed by passage of ureteral access dilators with their respective outer sheaths (9.5/11F, 35 cm; 10/12F, 35 cm; 11/13F, 36 cm; 12/14F, 35 cm; 13/15F, 36 cm; 14/16F, 35 cm) (all 35 cm sheaths were from Cook Medical, Bloomington, IN, whereas all 36 cm sheaths were from Boston Scientific). For each insertion, deployment forces were measured. For nonserial dilation, dilation began with passage of the 8/10F dilator followed by deployment of the 12/14F UAS. It is our standard practice to use the 8/10F dilator during all ureteroscopic cases to perform the retrograde ureteropyelogram before deployment of a UAS, and at the end of our cases to facilitate ureteral stent placement. Thus, we used 8/10F dilator to mimic our clinical conditions in the porcine ureter.
The porcine bladder was emptied between deployments using a 10F Foley catheter. Flexible URS was performed after each deployment, starting with the 8F dilator, to assess and grade any ureteral injury using the Postureteroscopic Lesion Scale (PULS 0–5) 18 (Appendix Table A1). Significant ureteral injury was defined as PULS ≥3 scores. The appearance of a ureteral injury was endoscopically recorded, and the injury location was confirmed with fluoroscopy.
Results
Six juvenile female pigs completed the study protocol. In the serial dilation group, the maximal force recorded for the UAS for each ureter during serial dilation (12 dilations/deployments per ureter) jumped considerably after deployment of a UAS ≥11F but, in general, did not peak until passage of the 13F UAS (Fig. 2). Endoscopic images and the corresponding fluoroscopic location of two ureteral injuries are given in Figure 3. There were 16 instances of PULS 1 scores with an average force value of 2.54N in the serially dilated group. Only one PULS 2 score was experienced in the serially dilated group after a deployment force of 5.59 N. Serial dilation had a threshold for PULS ≥3 at 5.63 N (Fig. 2). In the serially dilated group, locations of the initial injury (PULS ≥3) were experienced in the mid-ureter in four instances and the distal ureter in three instances (one ureter had two injury locations). There were no PULS 4 initial injuries; however, we observed these injuries only after an initial injury to the ureter had occurred and with larger access sheath deployment (14–16F); this occurred in 5/6 ureters at 16 separate locations. There were no PULS 5 injuries.
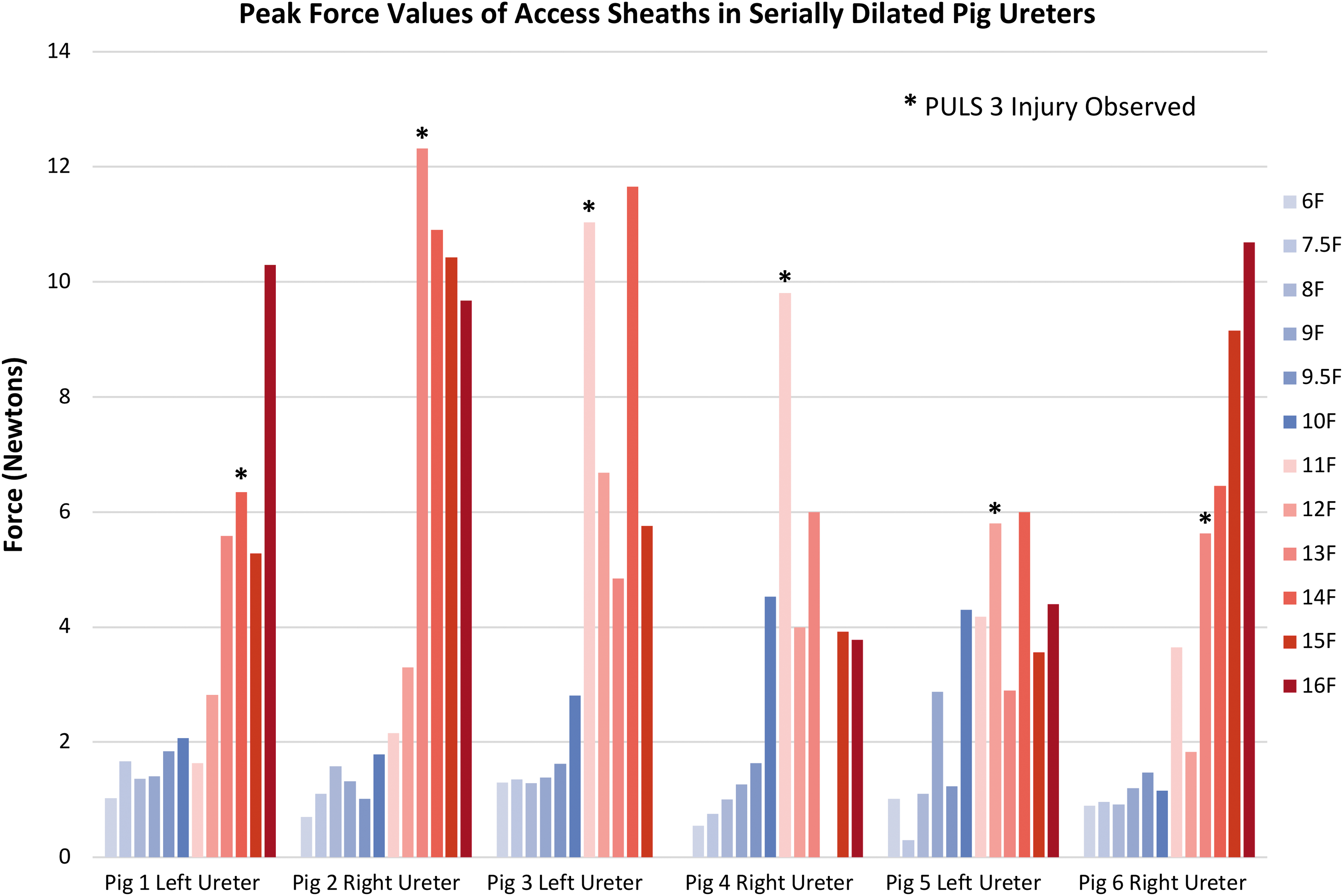
Peak force measured during serial UAS deployment in the porcine ureter. PULS = Postureteroscopic Lesion Scale; UAS = ureteral access sheath.

In five of the six juvenile female pigs, ureters selected for 12/14F UAS deployment after 8/10F dilation without serial dilation were injured (PULS ≥3) at a mean threshold force of 4.84 N (Fig. 4). There were no PULS 1 injuries, and a single PULS 2 injury at 8.11 N. Of these injured ureters (PULS ≥3) within this nonserially dilated group, locations of the initial injury were in the mid-ureter in three instances, the distal ureter in three instances, and the proximal ureter in one instance (three ureters had multiple injury locations). One ureter had a PULS 4 injury at 14.9 N. There were no PULS 5 injuries. Table 1 provides the maximum and minimum forces attained, collectively, by all six pigs and the associated injuries.

Peak force values measured during nonserial deployment of the 12/14F sheath following 8/10F dilator in alternating ureters.
Minimum and Maximum Forces Measured in the Ureters That Underwent Serial Dilation and Corresponding Injury
PULS 3 and 4 scores were selected because these values denote significant ureteral injury. There were no PULS 5 scores.
N = Newtons; PULS = Postureteroscopic Lesion Scale.
Discussion
UAS deployment has faced challenges since its introduction largely because of concerns over acute ureteral urothelial injury and the potential for subsequent ureteral stricture formation. 16,17,19 Newman and colleagues first reported concerns with the original UAS upon discovering a ureteral perforation in 8 of 43 (19%) cases in their prospective study. 20 Numerous design changes followed 13 including, tapered proximal tip of the inner dilator, metal coiling of the outer sheath to preclude kinking, and a liquid-activated hydrophilic coating. 4,8 Nevertheless, in a prospective investigation of 359 patients undergoing UAS-facilitated URS, Traxer and Thomas reported low-grade ureteral injury in 47% of patients and high-grade injury in 13% of patients. 17 The force required to induce such injuries has not been defined and thus surgeons are left to rely on their own individual unmeasured haptic feedback to determine what force to apply to the UAS during its deployment.
Accordingly, we sought to define how much force could be applied to the porcine ureteral wall before it would split (PULS ≥3). To this end, our team partnered with engineers and computer scientists at UCI to develop a novel load-sensing device and software package that could potentially be used in the operating room to measure the applied force throughout the deployment of a UAS over a guidewire.
In this initial work with the force sensor in the juvenile female porcine ureter, forces >8.1 N routinely resulted in a PULS ≥3 injury. When forces remained ≤4 N, no ureteral injury was observed. As the diameter of the UAS increased, so did the force required to deploy it; however, it was not until an 11F sheath was passed that 8 N was reached and a PULS 3 ureteral injury was noted in two of the six pigs. Not surprisingly, once the ureter was split, subsequent passage of the same size or a larger sheath necessitated less force and resulted in injury at multiple locations (Fig. 4; Table 1). In addition, it appeared that serial dilation increased the force threshold for injury by 0.8 N to 5.63 N (Figs. 2 and 4).
We hypothesize that during serial dilation of the porcine ureter, the ureter is expanded in a safer/slower manner, whereas in the nonserial dilation arm, we hypothesize the surgeon transmits more force acutely to the lower ureter resulting in more injury. Of note, most of the porcine ureteral injuries occurred in the mid-ureter which is not surprising given the anatomy of the porcine ureter with a commonly capacious ureteral tunnel. In contrast, our recent clinical data using the UAS-FS at our center has shown that the most common location of maximum force in the human ureter occurs at the distal ureter along the area of the ureterovesical junction (31%). 21
The concept of evaluating the force placed on the ureter during URS was first introduced by Ulvik and Wentzel-Larsen 22 who created a novel coupling device to attach a standard force meter to an 8.5F semirigid ureteroscope to measure forces exerted in the ureter during rigid URS. Mean retrograde insertion force ranged from 9.7 ± 7.3 N at the distal ureter to 4.4 ± 3.6 N at the proximal ureter. Although no complications were reported, the study did not grade ureteral injury nor provide long-term patient follow-up.
Similar studies utilizing porcine models have been performed to assess the force of UAS deployment. A feasibility study by Harper and colleagues, 23 compared the insertion force after placement of a novel radially dilating 9.5F UAS and a conventional 12/14F UAS in a porcine model to the interface of the ureteropelvic junction. The researchers reported mean forces of 0.48 and 2.2 N, respectively, and maximum forces of 1.6 and 6.5 N, respectively. These results are similar to our findings using the UAS-FS during 9.5F and 12/14F UAS deployment (mean application force of 0.67 and 3.63 N, respectively); however, peak application force showed greater variation (1.4–2.9 N and 7.6–11.4 N, respectively). Furthermore, although the Harper study used a novel, although not PULS, trauma score to assess ureteral damage after UAS placement, the amount of force at the moment of injury was not provided. Of note, similar to Ulvik and Wentzel-Larsen, 22 Harper and coworkers 23 used a standard force sensor that was not designed specifically for force measurement during deployment of a catheter or sheath over a guidewire.
Lildal and colleagues 24 evaluated the effect of isoproterenol on the insertion force of placing a 13/15F UAS in the porcine ureter, again using a standard force sensor with a coupling mechanism. During UAS placement, input force was measured, and deployment was stopped once subjective resistance was met by the operator. Subsequently, pharmacological intervention (i.e., intraureteral instillation of isoproterenol vs. saline) through a 10F ureteral catheter was delivered. Input force for ureters treated with isoproterenol was significantly less than those irrigated with saline. Of importance, mean endpoint values of 5.34 N (preirrigation) and 4.6 N (in 6 ureters with no subjective resistance) found by Lildal and colleagues 24 are similar to the limits of mean (1.7–4.0 N) and peak (4.2–10.0 N) 15F UAS forces measured in our study with the UAS-FS. Their study corroborated that the force applied, and resulting ureteral injury, varied with the operator thus highlighting the importance of being able to make the surgeon aware of the precise application force being applied during UAS deployment in real time. Of note, their study did not measure forces for different-sized UAS or define a threshold for injury.
There are several limitations to our study. First, this study is only meant as a pilot study in which the primary objective was to assess the operable reliability of the force sensor that we had developed. Although we have been assured of the accuracy of the UCI force sensor using our calibration weight, we have not compared its readings head-to-head with off-the-shelf force transducers as used in other studies. However, it is of note that the readings with the UCI force sensor were in the range of what other investigators have reported during instrumentation of the ureter. Second, translating our laboratory findings to the clinical scenario is a significant leap of faith; however, within the nonprimate animal kingdom, the pig ureter is most similar to the adult human ureter. 25,26 Based on the current findings, a clinical protocol was developed and is now in progress specifically examining force thresholds in the human ureter using 8 N as an upper limit of acceptable force. Finally, the PULS injury was determined by a solitary, nonblinded user at the time of the procedure. It would have been far better to have videotaped the exit URS after each manipulation and then have the videotapes reviewed by several fellowship trained endourologists to achieve a consensus PULS score for each catheter or UAS device that was passed.
Conclusions
The novel, UCI-developed, UAS-FS accurately and continuously measures forces during UAS or ureteral dilator deployment in a reproducible manner. Significant ureteral injury in the juvenile female porcine ureter can routinely be avoided if the applied force is <4.84 N; serial dilation may extend the “safe” range of deployment force to 5.5 N. In contrast, PULS ≥3 ureteral injuries routinely occur when forces exceed 8.1 N.
Footnotes
Acknowledgment
The authors thank Boston Scientific (Marlborough, MA) for sponsoring this laboratory study with a research grant.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
The Postureteroscopic Lesion Scale
| Grade | Ureteral injury description | Overall classification of operation |
|---|---|---|
| 0 | No lesion | Uncomplicated URS (no grading according to the Dindo-modified Clavien classification of surgical complications) |
| 1 | Superficial mucosal lesion and/or significant mucosal edema/hematoma | |
| 2 | Submucosal lesion | |
| 3 | Perforation with <50% partial transaction | Complicated URS (Grade 3a or b according to the Dindo-modified Clavien classification of surgical complications) |
| 4 | More than 50% partial transaction | |
| 5 | Complete transection |
Pietrow and colleagues. 11
URS = ureteroscopy.