
Abstract
Introduction:
Operative duration (OD) is associated with complications but has been poorly studied in minimally invasive partial nephrectomy (MIPN). We seek to examine the relationship between OD and complications in MIPN.
Methods:
The American College of Surgeons National Surgical Quality Improvement Program database was queried from 2011 to 2016 by CPT code. Risk factors for complications were determined using univariable and multivariable analysis.
Results:
In all, 12,018 patients were examined. OD was broken into deciles, ∼1200 patients in each, by minutes, <111, 111 to 131, 132 to 149, 159 to 164, 165 to 180, 181 to 196, 197 to 215, 216 to 238, 239 to 276, >276. Variables significantly associated with OD (values stated are shortest and longest deciles, respectively) include: male 47.8% and 68.2% of patients; body mass index 28.5 and 31.3 kg/m2; diabetes 13.4% and 23.7%; smoking 20.4% and 22.0%; taking medication for hypertension 53.1% and 64.2%. Morbidities significantly associated with OD (shortest and longest deciles reported, respectively) include: complications 4.2% of patients and 14.2%; postoperative transfusion 1.3% and 7.8%; pulmonary embolism (PE)/deep vein thrombosis 0.5% and 1.2%; renal insufficiency 0.3% and 1.7%; cardiac arrest or stroke 0.3% and 1.4%. On multivariable analysis, patients with OD >180 minutes were significantly more likely to have complications odds ratio of 2.0, 2.3, 2.3, 3.2, and 3.7 for deciles 181 to 196, 197 to 215, 216 to 238, 239 to 276, >276, respectively, p < 0.001.
Conclusions:
Even when adjusting for patient-specific preoperative factors, OD is an independent predictor of significant morbidity. Patients in the longest decile were nearly four times as likely to have complications. Further study is needed to determine reasons for prolonged OD.
Introduction
Approximately 64,000
Longer operative duration (OD) could be one potential factor, as it has been associated with poor outcomes in other fields and procedures. 8 –11 A complex interplay of factors contributes to OD, including surgeon's skill, surgeon's decision-making, surgeon's experience, patient factors, disease factors, and operating room workflow. 12 While there are described preoperative risk factors for complication in PN, little is known about the relationship between OD and postoperative complications. We hypothesize that longer OD is associated with an increased risk of complications in minimally invasive PN (MIPN).
Methods
The American College of Surgeons National Surgical Quality Improvement Program's (ACS-NSQIP) Participant Use Files (PUFs) between 2011 and 2016 was queried for cases with MIPN as the primary CPT code (50543). Cases were excluded if the total OD was >8 hours or <30 minutes. Additionally, cases were excluded if they were missing data on sex, height, weight, American Society of Anesthesiologists (ASA) class, or elective surgery status. Since patient ages ≥90 are identified as “90+” in the NSQIP PUFs, an age of 90 was imputed for these cases. Morbidity was defined as any of the following 30-day complications included in the database: mortality, superficial incisional surgical site infection (SSI), deep incisional SSI, organ/space SSI, wound dehiscence, pneumonia, bleeding transfusion, urinary tract infection, unplanned intubation, on ventilator for >48 hours, sepsis, septic shock, acute renal failure, progressive renal insufficiency, pulmonary embolism (PE), deep vein thrombosis (DVT) or thrombophlebitis, cardiac arrest requiring cardiopulmonary resuscitation (CPR), myocardial infarction (MI), and stroke with neurological deficit or cerebrovascular accident (CVA).
OD, defined as time from incision to dressing, was divided into deciles. Frequencies and column percentages were reported and p-values were calculated using Fisher's exact tests and chi-square, as appropriate, for categorical variables. Shapiro–Wilk normality test and histograms were used to examine continuous variables. Means and standard deviations were reported and p-values were calculated using one-way ANOVA for normally distributed continuous variables; otherwise, medians and first and third quartiles [Q1, Q3] were reported and p-values were calculated using Kruskal–Wallis tests.
Multiple variables included in the database were analyzed to determine their relationship with OD. Predictors of total OD were found using a stepwise procedure that identifies the most predictive multivariable linear regression model by minimizing Akaike's information criterion (AIC). Variables were included in the initial model if they were found to have a p-value <0.2. Since a large number of cases were missing at least one lab value, missing lab values were imputed with their respective medians before running the stepwise procedure.
In a similar fashion, the effect of total OD on morbidity was estimated while controlling for potential confounders using a multivariable logistic regression model. All variables that were found to have a p-value <0.2 in Tables 1 to 3 were included in the initial model, and an AIC-based stepwise procedure was used to find the group of variables that are most predictive of morbidity. Finally, total OD was added to the model.
Patient Characteristics Stratified by Total Operative Duration Decile
BMI = body mass index; Hx = history; SD = standard deviation.
Statistical significance was set at p ≤ 0.05. Missing observations were reported and excluded on an analysis-by-analysis basis. All analyses were done in R programming language, version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria). All graphics were produced using the R package ggplot2, version 3.0.0 (Hadley Wickham).
ACS-NSQIP and the hospitals participating in the ACS-NSQIP are the source of data used herein; they have not verified the data analysis and are not responsible for the statistical validity of it or the conclusions derived by the authors.
Results
Patient characteristics
Over 12,000 patients were identified, with ∼1200 patients in each decile. The mean age of the cohort was 59 years. Approximately 41% of the patients were female, and female gender was significantly associated with shorter OD. Median body mass index (BMI) was 29.8 kg/m2. Both BMI and BMI classification were significantly associated with longer OD. BMI in the shortest three deciles was 28.5, 29.2, and 29.3 kg/m2 and 30.0, 31.0, and 32.3 kg/m2 in the longest three deciles. Longer OD was associated with a higher ASA class. The percentage of ASA class III patients increased from 43.6% to 45.9% in the shortest deciles to 54.9% in the longest deciles, and the percentage of ASA II patients decreased from 54.6% to 42%. Other patient characteristics significantly associated with OD include diabetes, smoking history, male gender, and taking medication for hypertension (Table 1). For preoperative laboratory values by decile, see Table 2.
Patient Preoperative Laboratory Values Stratified by Total Operative Duration Decile
ASA = American Society of Anesthesiologists.
Patient outcomes
Given the large size of the data set, we used deciles to allow narrower ranges to more accurately identify potential inflection points in the data. Complication rate for the entire cohort was 8%. The rate of any of the examined postoperative complications was significantly higher in the longest three deciles—9.2%, 12.3%, and 14.2%—compared with the shortest three deciles—4.2%, 4.9%, and 5.6%. Postoperative transfusions were significantly more common in the longest deciles, with rates of 4.7%, 5.9%, and 7.8%, compared with the shortest deciles (1.3%, 1.8%, and 2.5%). Postoperative renal failure or renal insufficiency, venous thromboembolic events, and cardiovascular events such as MI and CVA were also more common in the longest deciles (Table 3 and Fig. 1A, B). The unadjusted effect of OD on any morbidity shows statistical significance for all deciles above the median (∼3 hours), with odds ratios (OR) of 2.0, 2.3, 2.3, 3.2, and 3.8, respectively, compared with the shortest operations (Fig. 2).

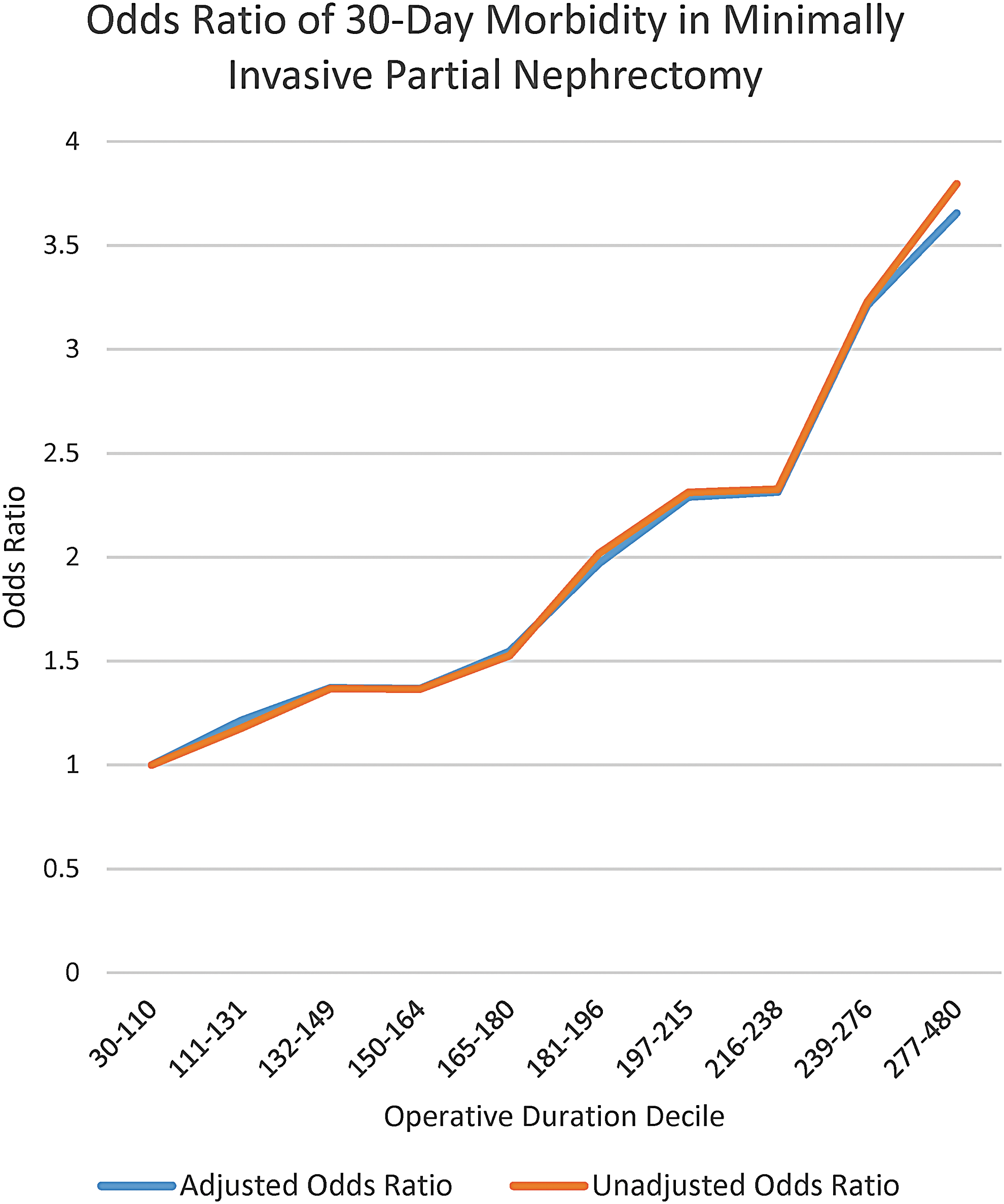
Odds ratio of 30-day morbidity in minimally invasive partial nephrectomy.
Patient Outcomes Stratified by Total Operative Duration Decile
DVT = deep vein thrombosis; LOS = length of stay; MI = myocardial infarction; SSI = surgical site infection; UTI = urinary tract infection.
Multivariable analysis
The following variables were then included in the multivariable analysis: gender, BMI group, diabetes, medication for hypertension, preoperative transfusion requirement, sodium, creatinine, albumin, alkaline phosphatase, INR, need for emergency surgery, outpatient status, ASA class, wound class, and OD. Preoperative transfusions, ASA class, and OD were all associated with increased morbidity. Statistical significance of the relationship between OD and risk of any morbidity was maintained for all deciles above the median, with adjusted OR of 2.0, 2.3, 2.3, 3.2, and 3.7 (Fig. 2).
Discussion
This study aimed to examine the relationship between any 30-day morbidity and OD in MIPN. Morbidity was significantly associated with both OD and ASA class. Adjusted analysis showed an increased risk of complications beginning at about 3 hours of case duration. Interestingly, little data exists regarding the potential association of OD with outcomes in MIPN. Routh et al. examined the association of OD with the incidence of non-urological complications in 2200 patients undergoing open nephrectomy and open PN. In their study, OD from 4 to 6 hours and >6 hours had an OR of morbidity of 1.91 and 4.84, respectively, which persisted on multivariable analysis. Examined morbidities were similar to this study, including DVT/PE, MI, and postoperative transfusion. 13 Another study of 1867 patients undergoing laparoscopic urologic surgery found that surgery lasting over 4 hours was an independent predictor of complications in patients undergoing surgery for urologic malignancy (OR 2.5). 8 Our results showed similar association of increased OD with increased risk of postoperative complications, limited to a cohort undergoing MIPN.
However, it is not clear what factors are most important in determining OD in an individual patient, or how those factors might contribute directly to increased risk of complications. Patient-specific factors, surgical technique, trainee involvement, intraoperative communication, intraoperative complications, surgical decision-making, surgeon's experience, surgeon's training, and surgeon's learning curve all are believed to influence OD. 6,9,10,14 Recently, Dagenais et al. examined 1461 cases of PN with respect to surgeons' variability in PN outcomes. Interestingly, but not surprisingly, the variability between surgeons' operative times and complications was not explained by patient-specific factors alone. 15 Furthermore, even after controlling for known surgeon-specific factors such as volume and fellowship training, 81% of OD variability was unexplained by known factors. 15 It seems likely that other, as-yet-undefined factors at the system, patient, and/or surgeon level exist and may have profound impact on OD. Such factors may or may not have a direct impact on the risk of complications independent of their effect on OD.
For many cases, it seems intuitive that disease complexity would have an important effect on OD, with more complex pathology requiring longer surgeries. However, the role of renal mass complexity in OD and its association with non-urologic complications is unclear. Simhan et al. examined 390 patients undergoing PN, and a multivariable analysis revealed that longer OD and a higher nephrometry score were each associated with major complications, such as urine leak. 7 Highly complex lesions were more likely to have more blood loss (130 vs 300 mL), higher ischemia time, and longer length of stay (LOS), along with higher rates of urine leak and transfusions. The high-complexity group also had ischemia time of 10 minutes longer than the low-complexity group. 7 However, OD in the low-complexity group was 198 minutes compared with 201 minutes in the high-complexity group, a negligible difference in OD despite the complexity difference. 7 Similarly, Waldert et al. examined 240 PN and found higher-complexity renal masses to be associated with greater ischemia time and more Clavien >0 complications, but not severity and type of complications. 16 Further studies have been unable to validate the correlation of tumor complexity with severity of complications. 17 While higher-complexity lesions may increase ischemia time, blood loss, and LOS, it is not clear that such lesions lead to longer OD. Furthermore, as current studies have not been able to predict an association of complication severity with tumor complexity, the association of these variables with major complications presented here is unclear.
Prolonged OD, it seems, decreases value from both outcomes and cost perspectives. Specific studies on MIPN have found OD to increase cost by $680 per 30-minute period on multivariable analysis. 6 Furthermore, complications at academic institutions have been estimated to cost $6,000,000 per year. 18 A study examining cost in MIPN has found the occurrence of one major complication in MIPN to increase cost by nearly $5,000 on multivariable analysis. 6 This same study has found transfusions to cost nearly $4,000, which in our cohort included 6% to 8% of patients in the longest two deciles. 6 As we move toward quality-based reimbursement, further study into longer OD will likely be necessary.
Despite the large number of patients and rigorous collection of data associated with this database, our study has several limitations. It is unclear if longer OD caused the complications, or if some other factor or a combination of factors contribute to longer OD. We attempted to minimize this by using multivariable analysis, but given this study design, we cannot prove longer OD as a causative. This data set does not have surgeon-level or renal mass-specific data, such as surgeon's experience or nephrometry scores. Also, the CPT code is the same for robotic and laparoscopic PN, and therefore, we could not examine this relationship. Our data only include major morbidities mentioned in the Methods section and do not consider other complications such as urine leak and pseudoaneurysm. Finally, cancer-specific outcomes and patient-reported outcomes were not examined, nor available in our data. However, the objective of this study was to generate a thought-provoking discussion and a more rigorous study in this area, not to provide definitive conclusions.
Conclusions
OD longer than 3 hours is associated with significantly increased risk of 30-day morbidity, compared with shorter OD. The reasons for longer OD are unclear as patient factors, mass factors, and known surgeon factors likely do not explain the complete difference. The goal of this work was to generate a thought-provoking discussion and study in this area. As we move toward value-based reimbursement, further study is needed concerning OD to elucidate if OD is causative of specific complications and the specific reasons for OD variability.
Footnotes
Author Disclosure Statement
No competing financial interests exist.