
Abstract
Background:
Although robotic surgery can improve ergonomics, strain in the hand and wrist is commonly reported. We evaluated gripping force differences between novice and expert surgeons while performing a da Vinci surgical simulator task.
Methods:
By attaching two force sensors to both master controllers, the average gripping force (AF) and maximum gripping force (MF) were evaluated. Participants (11 experts and 10 novices) performed the Suture sponge 1 task.
Results:
Almost all AF and MF in the dominant hand of experts were significantly smaller than those of novices. Mean gripping force with the dominant hand was correlated with the number of missed targets (r = 0.63, p = 0.002).
Conclusions:
Experts applied softer gripping force with the dominant hand than novices. Increased AF in the dominant hand was associated with more missed targets. These results may support learners to relax while performing robotic surgical procedures.
Introduction
There has been substantial recent interest in improving ergonomics during endoscopic surgery to prevent musculoskeletal injuries to surgeons. 1,2 Robotic surgery techniques generally appear to have physical advantages that improve a surgeon's ergonomics while decreasing the muscle workload by allowing the surgeon to remain in a seated position, providing brow and arm rests during surgical operations. 3 –5 In contrast, some researchers reported that, according to questionnaire and online survey results, physical symptoms or discomfort in the neck, shoulders, wrists, and hands were caused by robotic maneuvers. 5,6
Regarding neck stiffness, upper/lower back pain, and shoulder pain, surface electromyography is used to evaluate the difference of muscle activities (biceps, triceps, deltoid, and trapezius) between robotic and laparoscopic surgeries or between novice surgeons and expert surgeons. 3 –5 However, no previous studies have evaluated the intrinsic hand muscle activation involved, because it is difficult to evaluate the activation of small dense or overlapping muscles due to the lack of sufficient space to precisely attach an electrode to each interdigital muscle, and crosstalk among neighboring forearm muscles. 7
Several previous studies have assessed participants' dynamic finger force while playing a musical instrument (piano, violin, and clarinet). 8 –10 Practicing a musical instrument over a long time can cause overuse syndromes. Previous studies reported that experienced players apply less and shorter finger force with soft and efficient finger movements. 10 This information could support teachers and learners to recognize small differences among players at different levels of experience, and to give advice during teaching situations. In the field of robotic surgery, although differences in the dynamics of master manipulator velocity and movement have been reported, 11 there have been no reports of differences in the force applied to the master controller during robotic surgical maneuvers. The aim of this pilot study was to measure gripping force differences while participants performed a surgical simulation task (Suture sponge 1) with the da Vinci Skills Simulator (DVSS), and to analyze differences in task performance between novice and well-trained surgeons, including the time to deliver a virtual needle and the correlation between the number of missed targets and gripping force.
Methods
Force measurement system
Two force measurement sensors (USL06-H5-50N; Tec Gihan Co., Ltd., Kyoto, Japan) were attached to the left and right master controllers of a da Vinci surgical system (Intuitive Surgical, Sunnyvale, CA) device, by removing the straps and attaching aluminum plates (Fig. 1). The 2-cm square sensor can record normal forces as much as 50 N at the center screw hole on the sensor plane. The mechanism and accuracy of the forces measured by this sensor have been previously described. 12 A sampling frequency of 100 Hz was used to detect the gripping force. To quantify the applied force on the master controller, we used the larger of two values measured by two sensors on the master controller. Before the force measurement, we performed calibration of all force sensors.
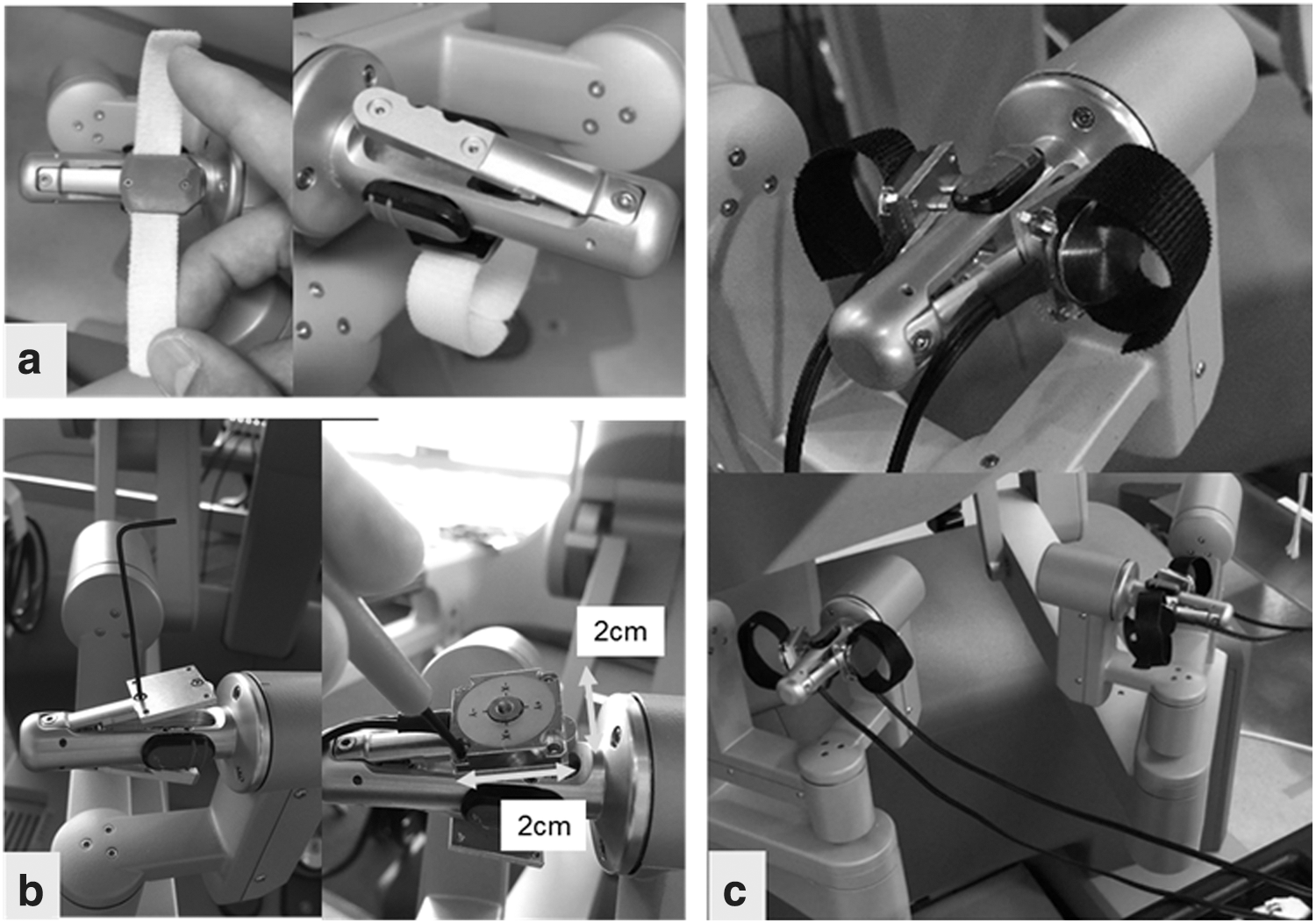
Force measurement system.
Simulator task procedure
We selected the Suture sponge 1 needle driving task in the DVSS. In this task, the needle must be passed from one predetermined point with a marker to another point with a marker on the suture sponge. This module was divided into four parts, as follows: Insert and rotate the needle from the top point to the bottom point with the right hand, then extract the needle with the left hand three times. Perform the same procedure as 1 with the left hand and extract the needle with the right hand three times. Insert and rotate the needle from the bottom point to the top point with the right hand, then extract it with the left hand three times. Perform the same procedure as in step 3 with the left hand and extract the needle with the right hand three times.
Participants
Twenty-one subjects were recruited for this study, and were divided into two groups: 10 novices who were residents with no robotic surgery experience and 11 well-trained urologists (experts) who had performed ∼100 robotic prostatectomies (Table 1). All participants were right handed. The study protocol was approved by the Ethics Committee of the Graduate School of Medicine, Kansai Medical University, Osaka, Japan (protocol number 1654).
Characteristics of the Participants and da Vinci Skills Simulator Score
Values are presented as the mean (standard deviation).
DVSS = da Vinci Skills Simulator.
Evaluating force parameters
Gripping force parameters
In this study, we measured the force applied to the master controller, and evaluated the average gripping force (AF) and maximum gripping force (MF). Based on a previous study, 8 we evaluated gripping force by deconstructing the task into three phases (Fig. 2): needle grasping (phase 1), needle insertion into the target marker (phase 2), and needle extraction (phase 3). Consecutive images of the virtual simulator were recorded, and the start and end frames of each phase were reviewed by Ta.Mi. and K.Y. The phases were defined as follows:
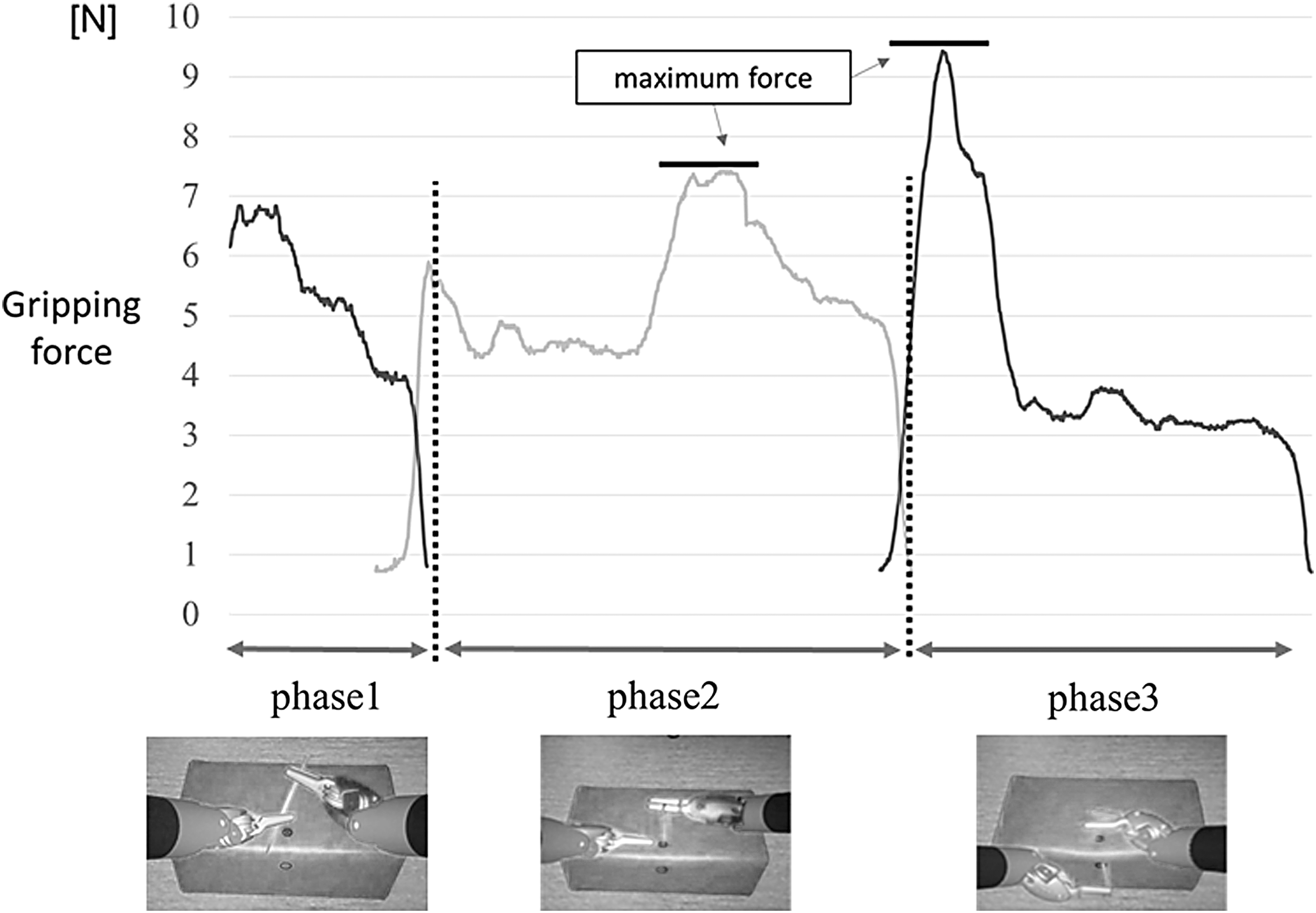
The black curve shows the left instrument force, and the gray curve shows the right-hand force. Segmentation of the simulation task. Phase 1, moving the needle from the delivering hand to the receiving hand; Phase 2, inserting and rotating the needle; and Phase 3, extracting the needle.
Phase 1
In phase 1, the needle was shifted from the delivering hand to the receiving hand. The beginning of phase 1 was defined when the receiving needle driver grasped the needle. The end of phase 1 was defined as the moment when the delivering needle driver moved away from the needle.
Phase 2
The beginning of phase 2 was defined as the moment when the delivering needle driver moved away from the needle. In this task, there were two markers on the sponge. If the participant hit the first marker, it turned from yellow to green and the second marker turned yellow (if the fist marker was not hit, the marker turned red). The participant then advanced the needle to the second marker. The end of phase 2 was defined as the moment when the first marker turned red, or the second marker turned green or red.
Phase 3
The beginning of phase 3 was defined as the moment when the needle was held by the receiving needle driver, and the end of phase 3 was defined as the moment when the needle moved away from the sponge.
Task performance
Needle grasping time with both hands
In phase 1, we evaluated needle grasping time (NGT) with both hands using the recorded virtual simulator image. Novice surgeons occasionally accidentally bend or deform the needle during surgery by grasping the needle in both hands for longer than experienced surgeons. We compared the difference in the time taken from the start to the end of phase 1 between novices and experts.
Correlation between number of missed targets and gripping force
In phase 2, we evaluated the correlation between AF and the number of missed targets to determine whether there was a relationship between excessive gripping force and the accuracy of the maneuvers.
Statistical analysis
All data are expressed as mean ± standard deviation. The statistical analysis was performed using SPSS 20.0.0.1 (SPSS, Chicago, IL). All parameters were compared between the two groups using the Mann–Whitney U test. Spearman's rank correlation was used to compare the number of missed targets and the gripping force in the simulated task. A p-value <0.05 was considered statistically significant.
Results
DVSS score
The DVSS scores are shown in Table 1. There were significant differences between groups for all parameters.
Gripping force parameters
In phase 1, there was no significant difference in MF of both hands between experts and novices (right-hand expert group: 6.95 ± 2.20 N, novice group: 8.47 ± 2.13 N, p = 0.18; left-hand expert group: 9.52 ± 4.82 N, novice group: 9.31 ± 3.12 N, p = 0.72) (Fig. 3). There was a significant difference in AF of the right hand between experts and novices (right-hand expert group: 4.26 ± 1.26 N, novice group: 5.71 ± 1.68 N, p = 0.024; left-hand expert group: 5.15 ± 2.76 N, novice group: 5.45 ± 2.04 N, p = 0.48).
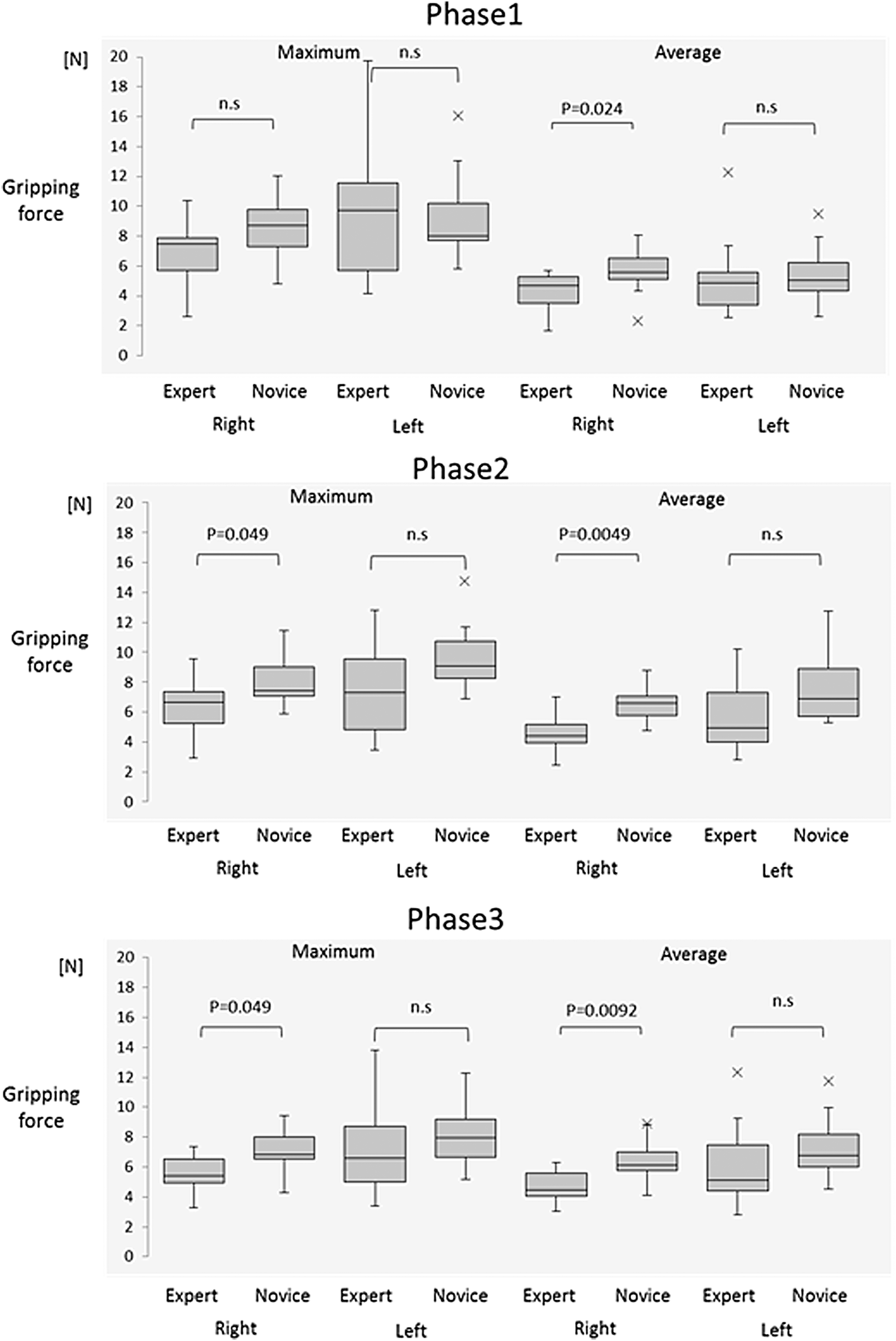
Results of MF and AF in each of the three phases. AF = average gripping force; MF = maximum gripping force.
In phase 2, there was a significant difference in MF of the right hand between experts and novices (right-hand expert group: 6.33 ± 1.84 N, novice group: 8.06 ± 1.78 N, p = 0.049; left-hand expert group: 7.52 ± 3.33 N, novice group: 9.58 ± 2.40 N, p = 0.11). There was also a significant difference in AF of the right hand between experts and novices (right-hand expert group: 4.58 ± 1.25 N, novice group: 6.42 ± 1.21 N, p = 0.0049; left-hand expert group: 5.57 ± 2.40 N, novice group: 7.54 ± 2.40 N, p = 0.057).
In phase 3, there was a significant difference in MF of the right hand between experts and novices (right-side expert group: 5.62 ± 1.19 N, novice group: 7.09 ± 1.64 N, p = 0.049; left-side expert group: 7.18 ± 3.05 N, novice group: 8.21 ± 2.16 N, p = 0.26). There was also a significant difference in AF of the right hand between experts and novices (right-hand expert group: 4.72 ± 1.09 N, novice group: 6.39 ± 1.60 N, p = 0.0092; left-hand expert group: 6.15 ± 2.79 N, novice group: 7.34 ± 2.18 N, p = 0.21).
NGT with both hands
There was a significant difference in NGT with both hands during phase 1 between experts and novices (expert group: 0.26 ± 0.077 seconds, novice group: 0.44 ± 0.12 seconds, p = 0.0015) (Fig. 4).
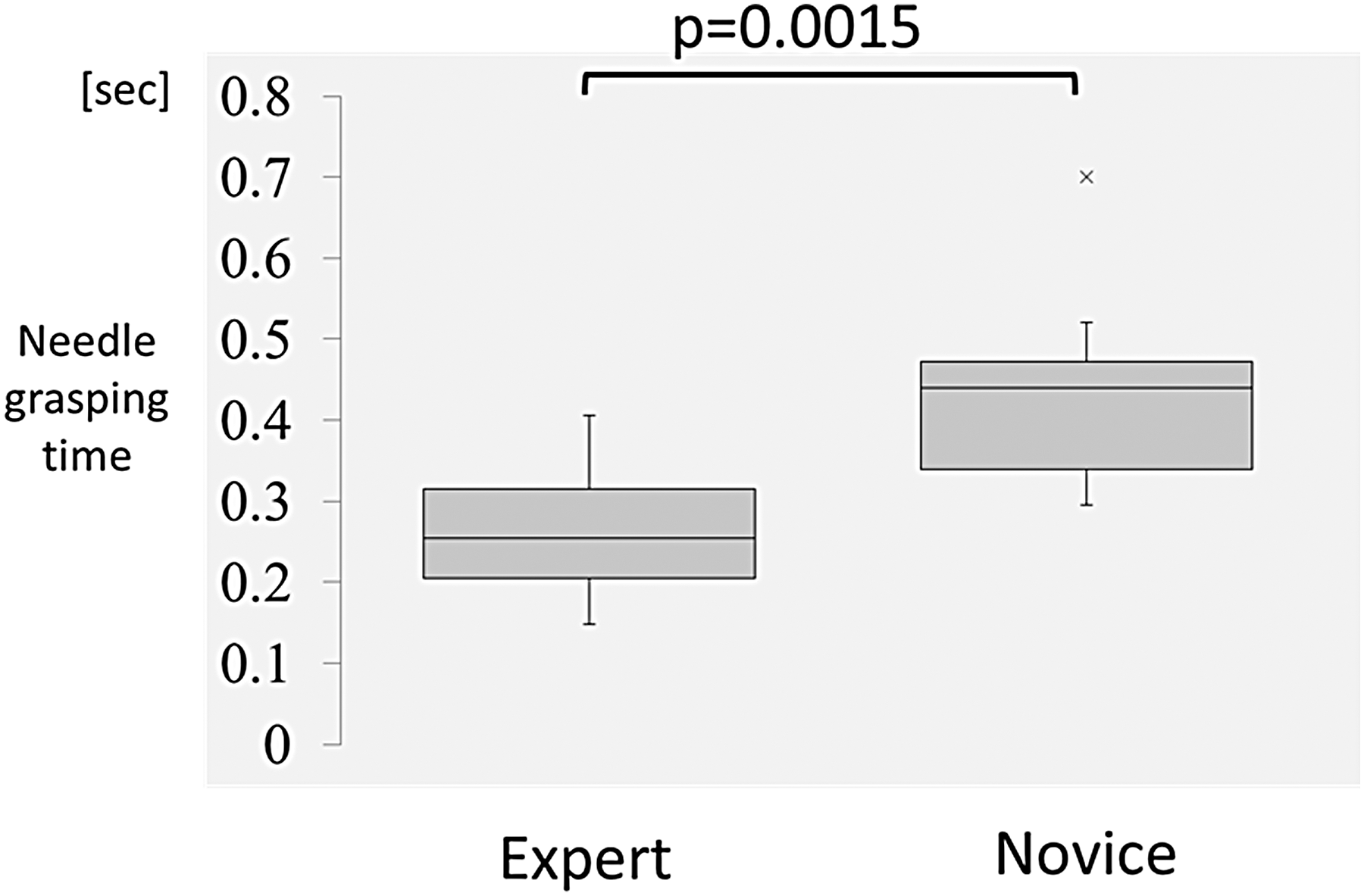
Needle grasping time with both hands.
Correlation between the number of missed targets and gripping force
AF of the dominant (right) hand was significantly correlated with the number of missed targets in phase 2 (r = 0.63, p = 0.002) (Fig. 5). There was no significant correlation with MF of both hands or AF of the nondominant (left) hand.
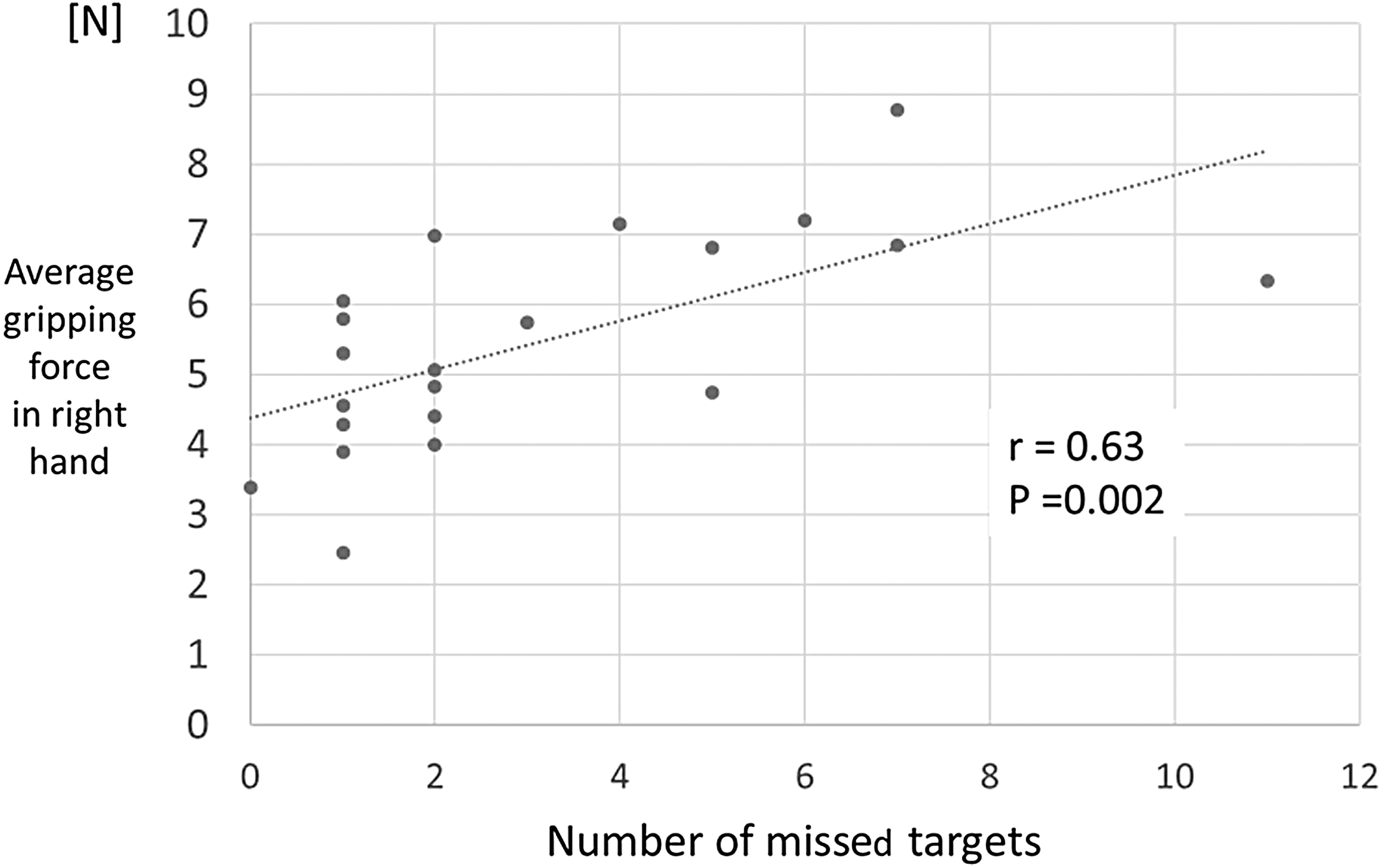
Relationship between number of missed targets and AF in phase 1.
Discussion
Robotic surgery has been found to improve surgeons' physical stress compared with conventional laparoscopic surgery, and several studies have reported a significant decrease in the muscle workload of the biceps and the flexor carpi ulnaris. 3 –5 However, high levels of strain are associated with robotic surgery. Bagrodia and Raman reported that 23% of urologists experienced neck and back pain while performing robot-assisted laparoscopic prostatectomy. 13 Tjiam and colleagues reported that 86% of urologists who responded to an online questionnaire experienced work-related complaints in the past 12 months. 14 Franasiak and colleagues reported that surgeons using robotic surgery systems experienced ergonomic strain in the neck (73.7%), shoulders (52.6%), lower back (42.1%), and wrist/hands (36.8%). 6
Some researchers have proposed that physical complaints in the wrist and hand can be caused by unnecessary tension on the intrinsic hand muscle due to the absence of tactile feedback of master controller. 5,6 Although large muscles, such as the trapezius, deltoid, and forearm muscles, were evaluated in terms of muscle workload using surface electromyography, 3 –5 small muscles, such as the intrinsic hand muscles, were not able to be evaluated because of difficulties in measurement. 7 Thus, measuring the gripping force on the master controller using a force sensor provides an alternative method for evaluating unnecessary tension in the hand during robotic surgery. Quantifying the gripping force at the master controller may extend understanding of how expert surgeons produce finger movements to control the manipulator.
The current results revealed that, in all three phases, most MF and AF of the right hand were smaller among experts than novices, although MF and AF of the left hand were not significantly different between groups in all phases. These results indicate that experts gripped the master controller more gently in their dominant hand. If experts had more experience performing surgery with their nondominant hand (e.g., >500 cases), the left-hand force might be expected to be smaller than that measured in this study.
Several previous studies examined gripping force during microsurgery and laparoscopic surgery. Harada and colleagues 15 reported a quantitative assessment of microsurgical anastomosis (phantom vascular model) using motion measurements and force sensing systems. The researchers evaluated a stitching task divided into needle placement (insertion, pushing, and extraction), suture handling, and knot tying phases. The results revealed a difference in maximum needle gripping force only in the needle extraction phase, although task completion time and the total path were shorter for skilled surgeons. Araki and colleagues 16 developed forceps that measure the gripping and reaction forces applied to laparoscopic instruments for clinical use. They quantified the force differences between novice and experienced surgeons in a kidney elevation maneuver during laparoscopic nephrectomy on a pig. The researchers suggested that experienced surgeons apply gripping force more slowly, softly, and stably than novices, enabling them to safely perform the maneuvers. 16 Similar gripping force trends may also occur in robotic surgery. Our current measurements of the gripping force on the master controller support these previous findings.
The current results also revealed that, in phase 1, novice surgeons grasped the needle with both needle drivers for a longer duration than expert surgeons, indicating that novice surgeons are less able to achieve sufficient cooperative movements with both hands. Although the value of NGT was small, this difference between two groups may lead to deformation or bending of the needle while passing the needle from one side to the other.
One previous study examined the correlation between gripping force and maneuver accuracy. Safwat and colleagues 17 reported that the gripping force on a stylus did not affect the endpoint accuracy. However, the task used in Safwat and colleagues' study was simple, requiring participants to maintain the location of a disk-shaped cursor at the target location on a two-dimensional monitor while they controlled the stylus with different gripping forces. 17 Therefore, the correlation between accurate surgical performance and excessive gripping force could not be examined. Actual surgical maneuvers are typically complex. Surgeons are often required to hold, dissect, suture, and cut tissue carefully by grasping, rotating, and pushing an instrument. The current results revealed correlations between AF on the dominant side and the number of missed targets. Excessive gripping force from the dominant hand can cause unstable and inaccurate maneuvers.
In contrast to the nondominant side, there were no significant correlations between AF and the number of missed targets. The number of missed targets with the nondominant hand was also smaller than that with the dominant hand. There are several possible explanations for these results. First, the Suture sponge 1 task proceeds from the right to the left hand, and we assumed that there was a learning curve. Second, the nondominant hand is typically clumsier, and surgeons may have moved their instruments more carefully along the shape of the needle when using their nondominant hand, compared with their dominant hand. Third, the height of the surgeon's elbow from the armrest might be correlated with the accuracy of the maneuver. The relationship between placing the elbow on the armrest and the performance of surgical maneuvers was examined by Yang and colleagues, revealing that proper armrest use improved the performance of operative maneuvers in the DVSS. 18,19 In addition, Takayasu and colleagues reported differences in posture patterns in the elbow position using an optical motion tracking system. 20 According to their results, the height of the elbow on the nondominant side was not significantly greater than the height of the dominant hand in both expert and novice groups. 20 In this study, although the position of the elbow was not evaluated, the elbow height of the nondominant hand might have affected the small number of missed targets.
Several limitations involved in this study should be noted. First, we did not evaluate the learning curve in terms of gripping force. As surgical skills are acquired, surgeons might gradually relax and decrease their gripping force. Second, when working in challenging environments, even expert surgeons may apply excessive gripping force. Therefore, further research is necessary to evaluate the correlation between grip force and missed targets during challenging situations involving anastomosis or bleeding. Third, many parameters may be related to missed targets, such as the junctional position of the wrist, elbow, and shoulder, and the speed of movement. Future studies should evaluate the correlations between muscle fatigue, junctional position, and gripping force. However, we assume that excessive gripping force may be a factor contributing to the likelihood of missing targets. Fourth, we only evaluated gripping force in this study, and did not propose a method for improving the skills of novice surgeons. We have been developing a force feedback system to alert surgeons using sound or a colored indicator on the screen when strong grip force is applied. In future, we plan to test this system in more stressful surgical maneuvers in which excessive force might be accidentally applied, and to evaluate the usefulness of a gripping force feedback system.
Conclusions
In conclusion, we measured gripping force on the master controller during simulations using DVSS and examined whether surgeons of different skill levels applied different gripping force. We found that experts gripped the master controller more gently with their dominant (right) hand compared with novices, whereas novices exhibited longer NGT than experts. Moreover, we assume that excessive gripping force may be a parameter that contributes to the likelihood of missing targets. These results can help novices understand how to decrease unnecessary stress while performing robotic surgical maneuvers.
Footnotes
Acknowledgments
This work was supported by JSPS KAKENHI, Grant Numbers 16K11074 and 17K11211, and Intuitive Surgical Clinical Research Grant, Grant Number ISI Grant-110216. The authors have no conflicts of interest or financial ties to disclose. We thank Melissa Gibbons, PhD, and Benjamin Knight, MSc, from Edanz Group for editing a draft of this article.
Authors' Contributions
K.Y. and T.M. provided conception and design of the study; K.Y., T.M., K.T., and M.W. performed acquisition of data; K.Y., T.M., and K.T. performed analysis and/or interpretation of data; K.Y. and T.M. drafted the article; T.M. and H.K. revised the article critically for important intellectual content; T.M., K.Y., K.T., M.W., H.K., and T.M. worked on the approval of the version of the article to be published.
Author Disclosure Statement
Drs. T.M., K.Y., K.T., M.W., H.K., and T.M. have no conflicts of interest or financial ties to disclose.
Funding Information
No funding was received for this article.