
Abstract
Introduction:
Calcium oxalate (CaOx) is the predominate component within renal calculi and can be divided into two subtypes: CaOx-monohydrate (COM) and CaOx-dihydrate (COD). COM and COD form in differing urinary environments, which suggest differential underlying metabolic abnormalities associated with each subtype. We compared clinical and metabolic findings in CaOx stone formers to delineate factors differentiating COD and COM stone formers and the implication this holds in terms of etiology and treatment.
Patients and Methods:
We identified CaOx stone formers that had passed their stones or had undergone endoscopic extraction between October 2014 and December 2018. Only patients who had a predominant subtype (≥80% COM or COD) and who had a 24-hour urine evaluation before medical management were included. Clinical and metabolic factors were compared in the two subgroups.
Results:
Out of 157 stone formers, 121 were COM and 36 were COD. COD formers were younger than COM formers with a mean age of 53 ± 16 vs 59 ± 15, respectively (p = 0.038). There were no observable differences in gender, body mass index, hypertension, diabetes mellitus, or hyperlipidemia. COM formers exhibited higher rates of hypocitraturia and hyperoxaluria, p = 0.022 and p = 0.018, respectively. Conversely, COD formers had significantly higher rates of hypercalciuria (47% vs 28%, p = 0.012). Multivariate analysis found hypercalciuria to independently predict COD (p = 0.043) and hyperoxaluria to predict COM stones (p = 0.016).
Conclusion:
COM formers are more likely to have hyperoxaluria, hypocitraturia, and elevated urinary oxalate levels compared to COD formers. COD formers exhibited higher incidence of hypercalciuria. These data suggest that all CaOx stones are not alike and that distinct metabolic and clinical etiological differences exist that may guide future management and prevention.
Introduction
The nationwide prevalence of kidney stones in the United States is proximately 8.8%, a 70% increase from 1994, and 5-year recurrence rates are as high as 30% to 50%. 1 These data suggest that further emphasis must be placed on stone prevention. During medical management of kidney stones, the specific course of dietary changes and medical therapy is determined by a patient's metabolic abnormalities and stone composition. 2
Calcium oxalate (CaOx) is the predominate component within renal calculi and can be divided into two subtypes as follows: CaOx-monohydrate (COM) and CaOx-dihydrate (COD). 1 COD and COM stones differ with respect to stone forming environments 3 ; therefore, delineating metabolic abnormalities associated with each subtype would assist in further advancing our knowledge of how these stones form and how these calculi can be treated. In laboratory evaluation of the urine from CaOx stone formers, urinary crystals of COM and COD have elevated urinary oxalate and calcium levels, respectively. 3 In this study we compare clinical and metabolic findings between COD and COM stone formers to elucidate factors that might be responsible for etiology and could be exploited in terms of treatment and prevention.
Patients and Methods
After institutional review board, we queried our prospectively-maintained endourology database of 2228 patients and identified CaOx stone formers that had passed their stones or had undergone endoscopic extraction between October 2014 and December 2018. Only patients who had pure CaOx stones as determined by Infrared Spectrum Analysis (Quest Diagnostics, Inc., Secaucus, NJ) and who completed a 24-Hour Urine Evaluation (Litholink Corp., Chicago, IL) before medical management were included. To compare COD and COM stone formers independently patients were separated into two groups: those with stones composed of ≥80% COM and those with stones composed of ≥80% COD.
To analyze how any significant metabolic results may present themselves on a grade, mixed CaOx stone formers—dihydrate/monohydrate composition <80%—were included in a separate analysis. In this additional analysis patients were separated into three groups based on the percent of dihydrate in their stone: CaOx stones with 0% to 33% dihydrate were included in Group 1, CaOx stones with 34% to 66% dihydrate were included in Groups 2, and 3 consisted of any CaOx stones with >66% dihydrate.
Baseline characteristics, including demographic information, history of hypertension (HTN), diabetes mellitus (DM), hyperlipidemia (HLD), coronary artery disease (CAD), gastrointestinal (GI) disease, glycated hemoglobin levels, as well as serum calcium, uric acid, and creatinine, were analyzed. Statistical analysis was performed with the SPSS software version 25 (IBM Analytics, Armonk, NY) using Chi-squared test, analysis of variance, and Student's t-tests, where appropriate. Variables from univariate analyses with p < 0.05 were included in a multivariable binary logistic regression analysis to identify independent predictors of stone type.
Results
Of the 1523 CaOx stone patients with both completed pretreatment 24-hour urine tests and stone analysis, 157 had a predominant (≥80%) COM or COD subtype and were included in the study. Of these, 121 were COM stone formers, and 36 were COD stone formers. The cohort included 106 men and 52 women. Mean body mass index (BMI) was 27.5 kg/m2 (±5.8) and mean age 58 years (±14.2). Univariate analysis revealed significant difference in mean age between the two groups, with COD formers being significantly younger than COM formers (mean age of 53 ± 16 vs 59 ± 13, p = 0.038).
No differences in rates of DM, HTN, HLD, CAD, or GI disease were observed between the two stone forming groups (Table 1). The mean rate of recurrence was 33% and 35% for COM and COD stone formers, respectively; this difference was not found to be significant (p = 0.584). In addition, no significant difference was reported in mean 24-hour urine volume (2.02 L vs 2.00 L, p = 0.914), mean BMI (27.8 kg/m2 vs 28.4 kg/m2, p = 0.640), percent male (66.7% male vs. 66.9% male, p = 0.563), mean HbA1c (5.7 vs 6.0, p = 0.353), and mean serum calcium (9.5 mg/dL vs. 9.5 mg/dL, p = 0.172).
Clinical Characteristics of Study Patients
Denotes significance.
t-Test.
Chi-square test.
Fisher's exact test.
BMI = body mass index; CAD = coronary artery disease; CaOx = calcium oxalate; CO2 = carbon dioxide; COD = CaOx-dihydrate; COM = CaOx-monohydrate; DM = diabetes mellitus; GI = gastrointestinal; HbA1c = glycated hemoglobin; HLD = hyperlipidemia; HTN = hypertension.
Comparison of metabolic abnormalities between the two groups revealed significantly higher rates of hypercalciuria (defined as male >250 mg/day, female >200 mg/day) in COD formers compared to COM formers (47% vs 28%, p = 0.027). Conversely, COM formers had higher incidence of both hypocitraturia (defined as male <450 mg/day, female <550 mg/day), 42% vs 22%, and hyperoxaluria (>40 mg/day), 43% vs 22%, than COD formers with p-values of 0.022 and 0.018, respectively (Table 2). From the 24-hour urine samples collected, COD formers had higher mean urinary calcium ion concentrations compared to COM formers (247.0 mg/day vs 193.5 mg/day, p = 0.012).
Metabolic Findings of Study Patients
Denotes significance.
A total of 183 patients were included in our secondary analysis of which 121 had a dihydrate composition between 0% and 33% (Group 1), 24 patients had dihydrate composition between 34% and 66% (Group 2), and 38 patients had stone dihydrate composition greater than 66% (Group 3). Rates of hypercalciuria in Groups 1, 2, and 3 were 27.3%, 29.1%, and 47.4%. Group 3 demonstrated a significantly higher rate of hypercalciuria compared to the overall prevalence within our sample (47.4% vs 31.7%, p = 0.019) (Fig. 1).
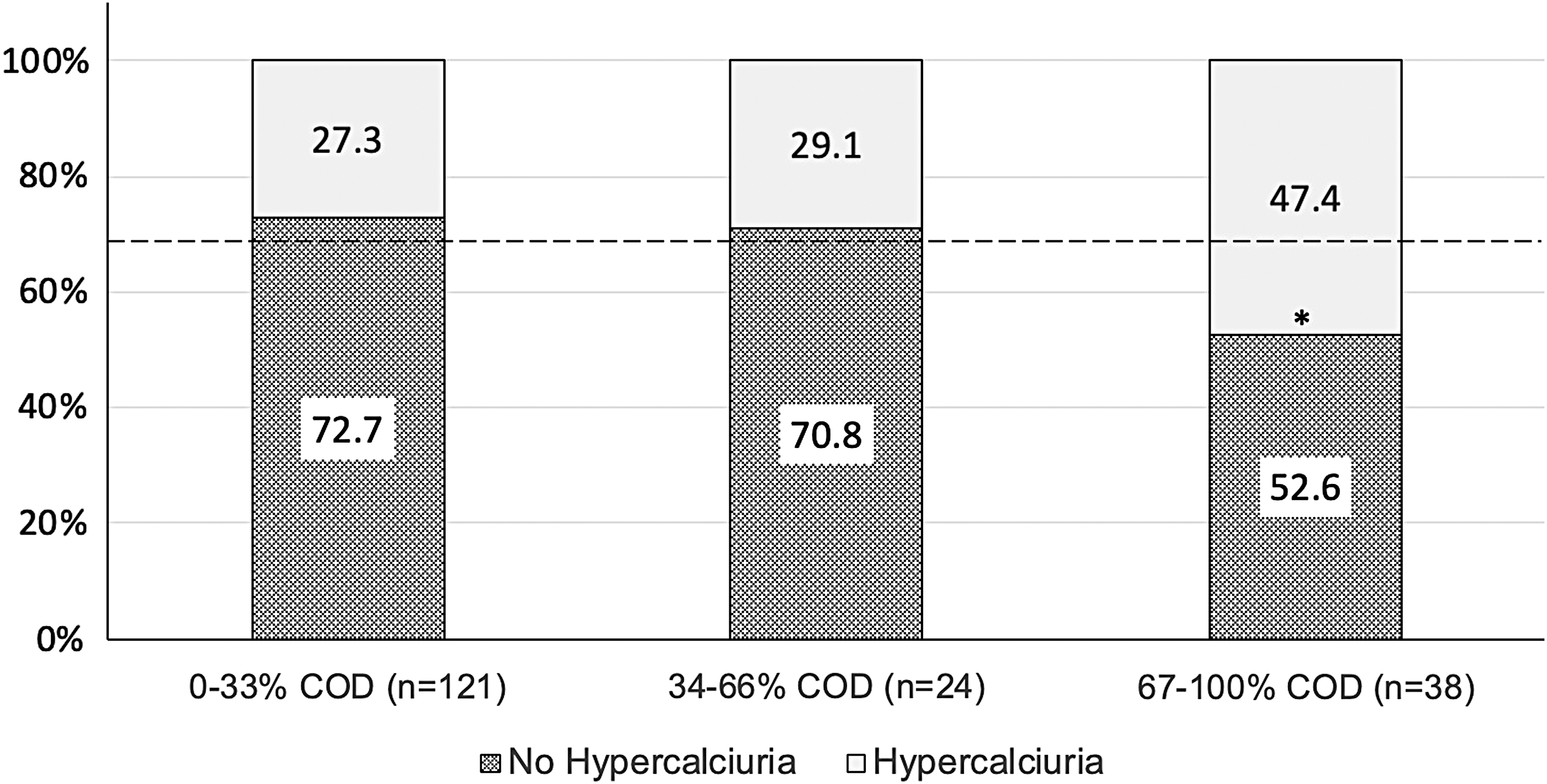
Rates of hypercalciuria based on percent dihydrate composition within CaOx stone formers. Dashed line indicates total sample rate of hypercalciuria, 31.7%. *p < 0.05. CaOx = calcium oxalate; COD = CaOx-dihydrate.
Rates of hyperoxaluria are as follows, 46% in Group 1, 37.5% in Group 2, and 44.7% in Group 3; however, no significant difference compared to the mean sample prevalence for hyperoxaluria, 44.8%, was noted (p = 0.743, p = 0.472, and p = 0.994, respectively). Finally, a comparison of hypocitraturia rates within the three groups reported prevalence in Group 1 to be 41.3%, Group 2 prevalence was 50%, and the prevalence in Group 3 was 23.6%, yet no significant difference from the mean total sample rate of hypocitraturia, 38.8%, was noted (p = 0.569, p = 0.260, and p = 0.056, respectively).
On multivariate analysis, hypercalciuria was independently associated with COD stones (odds ratio [OR] = 2.312, 95% confidence interval [CI] 1.03–5.20; p = 0.043), while hyperoxaluria was independently associated with COM stone formation (OR = 0.329, 95% CI 0.133–0.812; p = 0.016) (Table 3).
Multivariate Analysis of Metabolic Abnormalities in Predicting Stone Type
Denotes significance.
Discussion
In developed countries the 24-hour urine test has proven invaluable when analyzing a patient's metabolic profile and facilitates the development of patient-specific treatment regimens. However, such tests are not readily accessible in all areas of the world. Without this pertinent information, physicians are forced to treat stones as they present—significantly contributing to the high recurrence rates observed. 1 In this study, we sought to compare clinical and metabolic profiles of COM and COD stone formers to delineate any differences that would provide information on etiology and perhaps even suggest differential management for these supposedly similar CaOx stone formers.
Our data support the finding that not all CaOx stone formers are created equal. It is known that CaOx stone formers may possess a wide array of clinical factors that predispose their disease processes, including obesity and diabetes, along with genetic predisposition. 4 Metabolic factors such as high urinary oxalate, high urinary calcium, low urinary citrate, and low urinary pH also predispose patients to form CaOx stones. 1,3,5 –7 Some patients, however, present without any of these findings, and many present with multiple findings.
Finding accurate methods to substratify CaOx stone formers would provide insight into CaOx etiology and help guide further stone management. A singular 24-hour urine sample serves as a “metabolic photograph,” yet considering the dynamic nature of stone formation 24-hour urine testing is an imperfect tool. In addition, Tasian and colleagues 8 reported that diurnal variation of calcium excretion between the two kidneys may cause unilateral hypercalciuria to go undetected when analyzing bladder urine. They postulated that it is plausible diurnal variation that may apply to other urinary parameters, such as oxalate as well. 8 If in fact true, this may partially explain the variability in metabolic findings among CaOx stone formers.
There is strong evidence that COM and COD stones are quite different, even though they commonly occur together, with COD crystals on the surface and COM toward the center or core. 9 COM and COD crystals differ in structure and morphology resulting in dissimilar physical stone appearance. 10 COD stones are yellowish in color and tend to have a rough and irregular exterior and may have spikes emanating from the surface resulting in a jackstone. COM stones, in contrast, are brown to black in color and tend to have a smoother external surface (Fig. 2). 10

In addition, when viewed on CT scan imaging these two differ in appearance and density. On single energy multidetector CT scans, COM stones visually appear homogenous and smooth, whereas COD stones are more heterogeneous and irregular. Indeed, these findings are consistent within the internal architecture of the stones as well. 11 The range of density based on mean attenuation value has significant overlap, making distinctions between these stones on the sole basis of HU difficult. 12 On dual energy CT, however, the density of these stone types differ, with COD stones having a statistically lower density (323 ± 5 vs 510 ± 17 HU). 13
Moreover, the shape and morphology of these two stone types are also quite different as detected on microCT. 13,14 These differences manifest into the varied degree of how COD and COM stones respond to fragmentation. Stone composition can impact ease of fragmentation during shock wave lithotripsy (SWL). 15 However, stone heterogeneity and internal architecture are reported to strongly influence ease of fragmentation, where stones with varied architecture and higher degrees of heterogeneity are associated with increased response to SWL. 16 The observed difference in fragmentation carries forward with ureteroscopic laser lithotripsy, yet the difference is less detectable given the powerful nature of the Holmium laser that can fragment any human urinary stone regardless of density or composition. 17
Our study fortifies the evidence that COM and COD stones form and behave differently. More specifically, we illustrate the strong influence of hypercalciuria and hyperoxaluria in COD and COM stone formation, respectively. Using a binary logistic regression model, we found that patients presenting with hypercalciuria were over twice as likely to form COD stones. Conversely, hyperoxaluric subjects had approximately thrice the likelihood to form COM calculi.
The association between hyperoxaluria and COM stones has been previously reported and believed to influence monohydrate crystallization. 3 Elevated oxalate levels within urine are found to cause oxidative stress on renal tubular cells resulting in cell damage. 18 This disruption of epithelial cells in renal papillae leads to the formation of Randall's plaques, the nidus of COM calcification. 19 Although hyperoxaluria and COM formation have been reported in many studies, these results are not ubiquitous throughout the literature.
Galan and colleagues found that elevated oxalate was only found to influence COM formation in patients with low urinary pH, 20 whereas other groups of researchers comparing metabolic profiles in CaOx stone formers did not report an association between hyperoxaluria and COM at all. 21 However, many of these studies did not utilize standardized 24-hour urine testing and perhaps included patients with “mixed” CaOx stones given that their sample reports higher numbers of “pure” monohydrate or dihydrate stone formers than is generally seen. 20,22 In fact, of the 1523 CaOx stone formers with metabolic work-ups included in our sample, only 157 (10.3%) satisfy our inclusion criteria for being a COM or COD former.
In addition to oxalate, urinary citrate excretion has been implicated in COM stones. 23 Citrate is considered an ionic inhibitor of COM stone formation by disrupting the structural stability of CaOx crystals and, thereby, preventing nucleation. 23,24 In corroboration with previous studies, we found COM stone formers to have significantly lower urinary citrate compared to COD stone formers. 3 These findings highlight the clinical relevance of differentiating CaOx formers.
Currently potassium citrate is a common medical treatment for CaOx stones 25 ; however, the disparity in citrate levels between COM and COD formers may indicate that potassium citrate is more likely to be effective in treating patients with COM stones. Further research into the efficacy of potassium citrate in treating CaOx subtypes is needed. While there is some discrepancy in the literature regarding oxalate's role in COM stone formation, the association between hypercalciuria and COD appears consistent. Our results indicating that COD crystallization is favored by high urinary calcium is consistent with previous reports. 3,5,14,20,22,26
In addition, we found COD patients to be significantly younger than COM patients, a finding with implications given the increasing amount of evidence suggesting an association between calcium nephrolithiasis and a higher risk for bone fracture in the literature. 25,27,28 Notably, in patients with history of nephrourolithiasis hypercalciuria was found to be a risk factor for decreased bone density. Furthermore, a recent study by Denburg and colleagues indicated that risk of bone fracture was particularly high in adolescent boys with kidney stones. 29 In conjunction with our findings, these data reinforce the possible role elevated calcium excretion has in COD stone formation in addition to an increased risk of fracture in younger patients with renal stone disease.
In our secondary analysis we aimed to understand how differences in metabolic abnormalities might present themselves on a grade based on the degree to which dihydrate or monohydrate predominates the stone composition. Our data indicate an increase in proportion of patients with hypercalciuria as COD becomes increasingly predominate within CaOx stones. However, a significant deviation from the total sample rate of hypercalciuria was only found for Group 3, 67% to 100% COD (Fig. 1). We believe that further investigation into this trend with larger samples is warranted as an increase in sample size will facilitate analyses that can be conducted using more narrow percent dihydrate intervals.
Notable comorbidities such as DM, HTN, CAD, HLD, and elevated BMI (determinants of metabolic syndrome) have all been implicated as risk factors for nephrourolithiasis. 4,30 Although linked to kidney stone disease, no significant difference in these comorbidities was found between COD and COM stone formers.
The limitations of this study included a retrospective study design and limited sample size. Much of this has to do with our strict criteria as to what defines a predominate COD or COM stone. A notable strength of this study was that our participants were recruited from a large metropolitan area with a high level of diversity providing an ideal sociocultural cross-section to suggest generalizability to our results. Our findings are significant not only in that they imply differential etiologies but also because of their impact on management and prevention.
In terms of etiology, the close association of COD with hypercalciuria indicates that patients with recurrent mixed CaOx stones, despite medical therapy with a low oxalate diet and chelators, may have intermittent hypercalciuria or diurnal variation in calcium levels or differential excretion of calcium by their two kidneys partially accounting for the recurrences. In these patients, use of a thiazide diuretic in select situations may be warranted, especially if a substantial component of COD is found in their stones. In addition, knowing that a patient has substantial COD component within their stones may warrant consideration for SWL for a subsequent stone event, given that these stones tend to have more heterogeneous architecture, which has been associated with better shock wave outcomes.
Indeed, many clinical and metabolic factors must be noted when considering the use of thiazide and/or SWL for stone treatment. However, we suggest that stone composition may be included as an additional factor when choosing the optimal treatment course for a specific patient. Moreover, these data may serve particularly useful when other relevant information is not readily available. For example, in third world countries or areas in which 24-hour urine testing is either not available or prohibitively expensive, knowing the stone type could provide a clue about etiology and, thus, guide preventative methods, even in the absence of a detailed metabolic evaluation. Further work is warranted in distinguishing these stone types and measuring their impact on treatment and prevention.
Conclusion
We found COM stone formers to have higher incidence of hyperoxaluria and hypocitraturia, while COD stone formers were more likely to present with hypercalciuria and be younger in age. These data suggest that all CaOx stones are not alike and that distinct metabolic and clinical etiological differences exist that may guide future management and prevention.
Footnotes
Author Disclosure Statement
M.G. participates in education programs and lectures sponsored by Cook Urological, Inc., Olympus Medical, and Boston Scientific Corp. There are no other commercial associations related to this study to disclose.