
Abstract
Objectives:
To evaluate the long-term tumor recurrence, progression, and cancer-specific mortality (CSM) of patients after holmium laser ablation of non-muscle invasive bladder cancer (NMIBC) under topical anesthesia. To identify variables that help to predict risk of tumor recurrence, progression, and CSM.
Materials and Methods:
A prospective study of 251 consecutive patients with 399 recurrent NMIBC who underwent outpatient Holmium yttrium aluminium garnet laser ablation under topical anesthesia was carried out between September 2006 and September 2018. All patients underwent primary transurethral resection of bladder tumor to obtain histology. All patients completed a patient satisfaction questionnaire and visual analogue scale (VAS) for procedure-related pain.
Results:
All 251 patients were analyzed with an average age of 75.2 years and follow-up of 69.8 months. The majority of patients had multiple comorbidities with an American Society of Anesthesiologists of 3 or 4. The proportion of tumor grade 1, 2, and 3 disease and tumor stage Ta and T1 was 43.4%, 41.5%, 15.1%, 78.5%, and 21.5%, respectively. Overall, 57.8% of patients had at least one tumor recurrence with an average time of 16.3 months. Risk factors were tumor grade, number of tumors at time of first laser ablation, and tumor stage. Overall, 19.1% of patients demonstrated tumor progression with an average time of 51 months. Only 5.6% of patients had progression to muscle invasive bladder cancer, and the CSM rate was 5.2% with an average time to death of 71.2 months. Risk factors for CSM were tumor grade, stage, and the patient's age. The average VAS for pain was 0.6 out of 10, with all patients willing to have the procedure repeated if required.
Conclusion:
Laser ablation of NMIBC is a safe, effective, and well-tolerated long-term option for patients, particular in those who have moderate-to-severe co-morbidities. The long-term cancer outcomes are best for younger patients with primary low-grade and low-stage disease.
Introduction
Bladder cancer was the ninth most common cancer globally, with 430,000 new cases diagnosed in 2012. 1 In the United Kingdom, there were 10,171 new cases in 2015, making it the second most common genito-urinary malignancy, with 5383 cancer-specific deaths in 2016. 2 Approximately 75%–80% are non-muscle invasive bladder cancer (NMIBC) at diagnosis, with even higher proportions in younger patients. 3 There is a higher prevalence of stage Ta and T1 disease, due to good long-term survival rates and low cancer-specific mortality (CSM), compared with T2–4 disease. 4 Due to a combination of high prevalence rates and the vulnerability to multiple episodes of tumor recurrence and progression with bladder preservation treatment modalities, this disease process causes a substantial financial burden to the health service and has the highest lifetime treatment cost per patient of any cancer, followed by colorectal, breast, prostate, and lung cancer. 5,6
The conventional management of patients with bladder cancer is with white-light transurethral resection of bladder tumor (TURBT) under general anesthesia. Using this method, the overall recurrence, progression, and CSM of NMBIC is 47%, 10.7%, and 10.1%, respectively. 7 Repeated TURBT in an elderly population with recurrent disease is challenging due to high incidence of cardiovascular morbidity in this patient subgroup. There is, therefore, a need for alternate treatment modalities with the potential to avoid general anesthetic (GA) altogether. 8,9
Laser technology has been used for the management of NMIBC for approximately four decades. Staehler and colleagues 10 were the first to publish their initial experience of endoscopic laser ablation of NMIBC in 15 patients from the University of Munich in 1978. They used neodymium:yttrium aluminium garnet (Nd:YAG) laser for destruction of recurrent bladder tumors ranging from 5 to 10 mm and noted no short-term recurrence or complications. 10 The use of Nd:YAG was subsequently abandoned, due to the long extinction length of up to 18 mm increasing the risk of bowel injury, and the first use of holmium:yttrium aluminium garnet (Ho:YAG) laser for bladder tumor ablation was reported by Johnson in 1994 on 15 patients with a 3-month infield recurrence rate of 20%. 11 Subsequently, the use of Ho:YAG laser, in an outpatient setting under local anesthesia, has been shown to be safe and effective in the management of recurrent NMIBC. 12 Over the past few decades, several small studies have reported on the successful use of Ho:YAG laser for the ablation of recurrent NMIBC as an alternative to conventional TURBT or cystodiathermy under GA. The short-term recurrence rate has been well described, and it ranged significantly between 0% and 73%. 13 However, there is no evidence on the long-term outcomes of patients undergoing laser ablation of recurrent NMIBC in terms of disease progression to muscle invasive bladder cancer (MIBC) and CSM.
Our primary objective was to evaluate the long-term tumor recurrence, progression, and CSM of patients after holmium laser ablation of NMIBC under topical anesthesia. The secondary objective was to identify variables that help to predict risk of tumor recurrence, progression, and CSM.
Materials and Methods
Patient selection
In this prospective study, all consenting patients who presented with recurrent NMIBC to a single referral center between September 2006 and September 2018 were included. The inclusion criteria for the study were: patients consenting to regular endoscopic surveillance and Ho:YAG laser tumor ablation under topical anesthesia, primary histology confirmed NMIBC (Ta–T1, G1–3) after a primary TURBT or re-resection if high-risk primary histology (G3 or T1 disease), and willingness to complete the patient satisfaction questionnaire with a visual analogue scale (VAS) for procedure-related pain at the time of the first treatment. Exclusion criteria were: abnormal lower urinary tract anatomy, presence of MIBC, or carcinoma in situ (CIS) on original histology. Anticoagulation was not an exclusion criterion, and medical therapies were not stopped before the procedure. After a multidisciplinary confirmation of NMIBC histology and risk stratification, patients were offered intravesical therapies, as required, and underwent regular endoscopic surveillance according to published international protocols, with all having their first surveillance cystoscopy at 3 months. 14 Risk stratification of patients was undertaken according to bladder tumor characteristics into Low, Intermediate, and High risk groups. All patients received immediate post-operative intravesical mitomycin C. Patients with intermediate risk were offered × 6 additional (Mitomycin), and patients with high risk were offered intravesical (Bacille Calmette-Guerin) (induction and maintenance) as per international guidelines. 14
Patients with low-risk original disease or co-morbid patients with intermediate- or high-risk disease who had tumor recurrence were counseled and offered endoscopic laser ablation of tumor as an alternative to conventional TURBT. During endoscopic surveillance of patients who had undergone laser ablation, tumor recurrences that were >3 cm on endoscopic view, multifocal, non-papillary or mixed appearance, suspicious of CIS, or with positive urine cytology were offered biopsy for histology under either general or regional anesthesia to ensure early diagnosis of upgrading or staging of the disease. Intermittent cross-sectional imaging (computed tomography or magnetic resonance imaging) was offered to patients to evaluate for extra-vesical disease or muscle invasion in patients unwilling to proceed to biopsy. Relevant cross-sectional imaging performed for unrelated issues was also evaluated. A prospective database was maintained detailing patient demographics and original tumor histology, size and location of tumor recurrence and/or progression, subsequent tumor histology and all cross-sectional imaging, laser settings and operative time, procedure-related complications, patient satisfaction questionnaire and VAS, and time and cause of death. Records were also kept to determine whether recurrences were localized (on-site) to original laser ablation, or distant (off-site) and whether progression was to MIBC. The start point of the study was recorded as the date of first tumor ablation using Ho:YAG laser. The primary endpoint was either patient death or continual surveillance at the end of the study period.
Procedural technique
All patients were treated in a laser compliant endoscopy room as an outpatient procedure. All clinical staff were trained in laser safety, and universal precautions were taken. The flexible cystoscope (Olympus CYF-V/VA) and laser machine (ACMI-GYRUS DUR-HL30) used were regularly serviced. The procedure was carried out by using a 17F video flexible cystoscope with 210°/120° deflection, using topical gel per urethra (Instillagel®). Ciprofloxacin 500 mg was given 30 minutes before the procedure. No additional analgesics were required. Urine culture was performed pre-procedure to exclude infection, and if indicated urine for cytology was collected before the procedure. Using normal saline irrigation, diagnostic cystoscopy was carried out and a 200 or 365 μN laser fiber was passed through the working channel of the flexible cystoscope if tumor ablation was required. The exophytic papillary component of the tumor was ablated by brushstroke movements with the laser fiber on top of the tumor. The base of the tumor was subsequently vaporized. Biopsies were not routinely taken, but if there was any suspicion of disease progression, as explained earlier, patients were offered a formal GA cystoscopy and biopsy. For longer procedures, a small catheter was inserted alongside the flexible cystoscope to aid bladder drainage. Post-operative catheterization was not routinely performed. Standard laser frequency was 6 Hz, with 0.9 kJ energy; however, around more sensitive areas, such as the trigone, bladder neck, and ureteric orifice area, the laser frequency was 6 Hz, with 0.6 kJ energy. All patients completed a satisfaction questionnaire and VAS for pain after their first treatment and had a follow-up flexible cystoscopy at 3 months post-procedure to monitor the treatment response. All patients in the study had undergone previous diagnostic flexible cystoscopies; therefore, the questionnaire evaluated patients' satisfaction and VAS for pain of flexible cystoscopy with tumor laser ablation as compared with their previous flexible cystoscopy alone.
Statistical analysis
Kolmogorov-Smirnov and Sharipo-Wilk tests were used to check whether the data fell within a normal distribution with boot-strapping methods utilized for data that did not. Simple-Cox and Logistic-Regression models were used for the multivariate analysis of tumor recurrence. Chi-squared test was used for the multivariate analysis of tumor progression due to the smaller size of this sub-population. Mann-Whitney U test was used for the analysis of the patient satisfaction questionnaire, and VAS was utilized for procedure-related pain. A Kaplen-Meier survival curve was created by using IBM SPSS Statistics 19.0 software and Log-Rank, Breslow, and Tarone-Ware tests were used for survival function analysis.
A p-value <0.05 was considered to indicate statistical significance.
Results
Two hundred fifty-one patients with 399 non-muscle invasive bladder tumors were included in the study. The mean average age was 75.2 years, which included 199 (79.3%) male patients. The original histology of the majority of patients was Ta and G1–2, contributing 197 (78.5%) and 213 (84.8%) respectively. The mean average tumor size was 11.67 mm (range 3–50 mm), with 157 (62.5%) patients having a solitary tumor. Patients in this cohort had significant comorbidities, with 225 (89.6%) being classified as American Society of Anesthesiologists (ASA) score 3 or 4. The overall mean average time of follow-up [95% confidence interval (CI)] was 69.8 [65.2–74.4] months. The mean average operative laser time was 76 seconds (range 7–420 seconds). Patient and tumor characteristics are shown in Table 1.
Patient and Tumor Characteristics
ASA = American society of anesthesiologists; CI = confidence interval.
Tumor recurrence
Overall, 145 (57.8%) of the patients had at least one tumor recurrence throughout the study period. Out of these patients, 93 (64.1%) had localized (on-site) recurrence at the site of the previous laser ablation, whereas 52 (35.9%) had distant (off-site) recurrence. The time distribution of bladder tumor recurrence was right-skewed and did not fall within a normal distribution therefore boot-strapping methods were used. Table 2 displays the recurrence rate in relation to tumor grade and stage. The mean average time to bladder tumor recurrence was 16.3 months (95% CI: 13.6–19.4 months).
Recurrence Rates in Relation to Tumor Grade and Stage
Patients with original histology of grade 3 disease had the highest risk of tumor recurrence (3.14 times higher than the patients with grade 1 and 1.72 times higher than the patients with grade 2). The patients with grade 2 disease had a 1.83 times higher risk of recurrence as compared with patients with grade 1. There was a trend toward patients with tumor stage T1 having a higher risk of the tumor recurrence than patients with stage Ta disease, but this was not statistically significant.
The only other variable that affected tumor recurrence was the number of tumors in the primary laser ablation procedure (p = 0.007). Age, sex, tumor size, ASA score, and tumor position did not significantly affect tumor recurrence.
There was no significant relationship between the variables and whether tumor recurrence is localized (on-site) or at a distant site (off-site) in the bladder.
Progression
Progression to either histologically higher grade/stage disease or radiological evidence of progression
Overall, 48 (19.1%) patients had tumor progression during the study period. This included patients with histological evidence of higher grade or stage disease in subsequent biopsy specimens compared with the original histology, or patients with cross-sectional imaging confirming tumor progression. The mean average time for tumor progression [95% CI] was 50.96 [43.11–58.58] months. Table 3 displays the progression rate in relation to tumor grade and stage.
Progression Rates in Relation to Tumor Grade and Stage
Chi-squared test indicated that original tumor grade had an association with bladder tumor progression (χ 2 = 19.09, p < 0.001). Patients with grade 3 disease were more likely (44.7%) to have bladder tumor progression compared with patients with grade 1 (13.8%) and grade 2 (15.4%). There was a trend toward T1 disease being more likely to cause bladder tumor progression compared with Ta disease but was not statistically significant (χ 2 = 3.332, p = 0.079). Chi-squared test indicated that patient sex (χ 2 = 0.663, p = 0.431), age (χ 2 = 0.105, p = 0.750), number of tumors (χ 2 = 1.781, p = 0.182), size of tumor (χ 2 = 0.012, p = 0.913), position of tumor in bladder (χ 2 = 2.667, p = 0.849), and ASA score (χ 2 = 0.266, p = 0.876) had no association with bladder tumor progression.
Progression to MIBC by either histological or radiological evidence
The risk of progression to muscle invasive cancer was 5.58% (n = 14). The average time to progression to muscle invasive cancer [95% CI] was 38 [28.59–48.50] months.
Chi-squared test indicated that original tumor grade had an association with progression to muscle invasive cancer (χ 2 = 69.801, p < 0.001). The patients with grade 3 disease (34.2%) were more likely to progress to muscle invasive cancer compared with patients with grade 1 (0.0%) and grade 2 (1.0%). T stage had an association with progression to muscle invasive cancer (χ 2 = 3.332, p = 0.079). The proportion of patients with T1 stage, which had the progression of muscle invasive cancer, was 11.1% whereas for patients with stage Ta this value was 4.1%; however, these results were not statistically significant.
Chi-squared test indicated that sex (χ 2 = 0.372, p = 0.741), age (χ 2 = 0.766, p = 0.419), number of tumors (χ 2 = 1.625, p = 0.263), size of tumor (χ 2 = 0.113, p = 0.737), position of tumor in the bladder (χ 2 = 3.405, p = 0.757), and ASA score (χ 2 = 1.882, p = 0.390) had no association with the risk of progression to muscle invasive cancer.
Mortality
Overall mortality
At the end of the study, 64 patients had died, resulting in an overall mortality of 25.5% with a mean average time [95% CI] of 75.6 [66.64–84.83] months.
Chi-squared test indicated that sex (χ 2 = 0.009, p = 0.926), T stage (χ 2 = 0.618, p = 0.481), number of tumor (χ 2 = 0.347, p = 0.654), size of tumor (χ 2 = 0.114, p = 0.736), position of tumor in bladder (χ 2 = 3.354, p = 0.763), and ASA score (χ 2 = 3.119, p = 0.210) had no association with the risk of death.
Age had an association with risk of death (χ 2 = 9.631, p = 0.002). Tumor grade had a significant association with risk of death (χ 2 = 14.536, p = 0.001). The patients with grade 3 disease had a higher risk of death (50%) in comparison with patients with grade 2 (19.2%) and grade 1 disease (22.9%).
Figure 1 displays a Kaplan-Meier curve of the adverse outcomes for all patients during surveillance (either bladder tumor progression or patient death) over time.
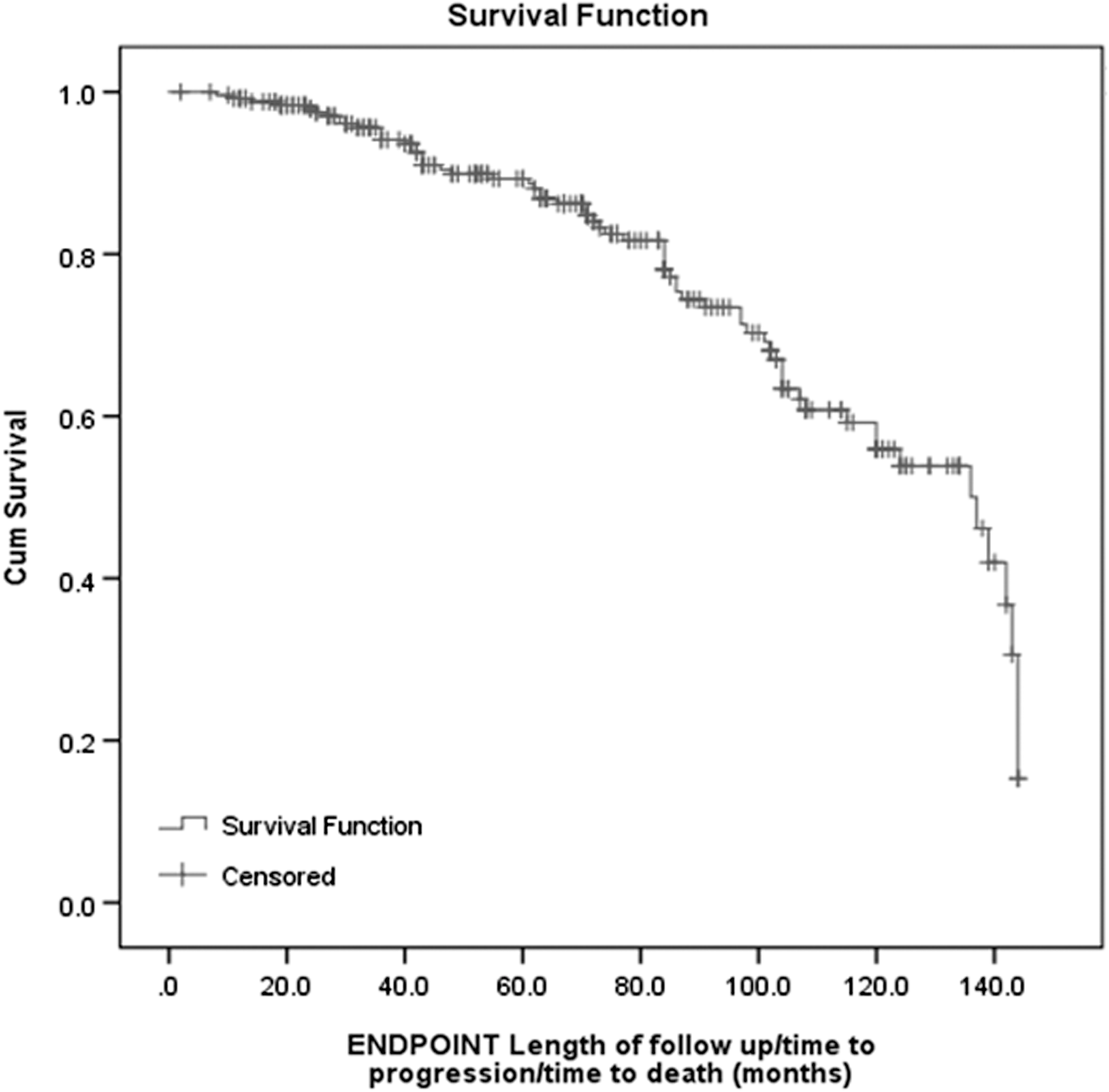
Kaplan-Meier curve of adverse surveillance outcomes (disease progression or death) over time.
Cancer-specific mortality
The risk of CSM was 5.2% (n = 13), with a mean average time [95% CI] of 71.3 [55.46–91.16] months. These patients all died as a direct consequence of their bladder cancer as documented on the official death certificate.
Chi-squared test indicated that sex (χ 2 = 0.046, p = 0.736), number of tumors (χ 2 = 0.261, p = 0.772), size of tumor (χ 2 = 0.574, p = 0.555), position of tumor in the bladder (χ 2 = 3.845, p = 0.698), and ASA score (χ 2 = 3.802, p = 0.149) had no association with the risk of CSM.
Tumor grade had a significant association with the risk of CSM (χ 2 = 41.637, p < 0.001). The patients with grade 3 disease had a higher risk of CSM (26.3%) compared with patients with grade 2 (2.9%) and grade 1 disease (0.0%). T stage also had a significant association with CSM (8.488, p = 0.009). The patients with T1 disease had a higher risk of the CSM (13.0%) compared with patients with Ta disease (3.0%). Table 4 shows the estimated time to mortality for patients having laser ablation for recurrent NMIBC in terms of original tumor grade and stage.
Estimated Mean Survival Time for Patients Comparing Different Original Tumor Grades and Stages (Months)
SE = standard error.
Patient Satisfaction Questionnaire and VAS for procedure-related pain
Overall, four patients reported dysuria, one patient had ongoing haematuria, and one patient had urinary frequency immediately post-procedure. These were isolated cases with no evidence to consider that any variables have an impact on them. All patients' symptoms resolved with no requirement for further invasive intervention. The average VAS (0–10) for procedure-related pain compared with flexible cystoscopy alone was 0.6 (0.5–0.8).
One hundred seventy-five patients (69.7%) estimated pain during the procedure of 0 out of 10 (indicating no difference compared with flexible cystoscopy alone), with a maximal score of 6 out of 10 for pain (4 patients). Considering that there is a non-symmetrical distribution of the pain scores, the non-parametric Mann-Whitney U test was used to conduct a multivariate analysis to evaluate for any relationship with intra-operative pain. The results indicated that there is no association between any variables and patients' pain scores.
The only trends in mean pain scores were that patients with severe co-morbidities and an ASA score 4 (mean pain score 0.68) had a minimally higher average pain score than healthier patients with an ASA score 2 (mean pain score 0.46), but this was not statistically significant (p = 0.084).
All 251 patients reported that they were overall satisfied with the treatment, and all patients reported that they would undergo the procedure again if required.
Discussion
Our present prospective study is the largest evaluating the natural history of recurrent NMIBC after Ho:YAG laser ablation under topical anesthesia with the longest follow-up. With a mean tumor burden of 11.7 mm, we studied 399 tumors in 251 patients with a mean follow-up of 69.8 months.
The Ho:YAG laser is ideally suited for endourology and its use has evolved significantly over time. Although it has become commonplace in the surgical treatment of urolithiasis and benign prostatic hyperplasia, it is also clinically useful for the management of bladder cancer. Although our study focuses on photoablation of tumors, a meta-analysis has also reported on the benefits of holmium laser enucleation of bladder tumor compared with conventional electrosurgical methods. 15 It is a pulsed, solid-state laser that has a short extinction length (penetration depth of ∼0.4 mm) due to strong absorption at around 2100 nm by water molecules. The highly absorbed power and immediate increase in temperature leads to vaporization in the irrigant fluid next to the fiber tip where pulsatile steam bubbles are generated. The tissue effect is rapid, and haemostasis of the Ho:YAG laser is excellent. Despite our study including some large tumors up to 5 cm, we only report one procedural-related complication of monosymptomatic hematuria that settled without intervention. Theoretically, the lack of deep penetration as compared with conventional diathermy should reduce the pain perception for the patient, making it ideal for use under topical anesthesia. Although no head-to-head study of bladder tumor ablation under topical anesthesia between Ho:YAG laser and cysto-diathermy has been conducted, our present study has demonstrated excellent patient satisfaction ratings, with only 3% reporting a pain score of 5 or higher compared with flexible cystoscopy alone. In contrast, Davenport and colleagues evaluated outcomes of patients undergoing cysto-diathermy under topical anesthesia and reported that 12% of patients found the procedure painful using a VAS. 16
The current evidence for the natural history of recurrent NMIBC treated by endoscopic Ho:YAG laser is heterogenous and mainly based on small population studies with limited follow-up. Although short-term recurrence rates have been consistently reported, no data have been published on long-term tumor recurrence and progression rates, as well as CSM (Table 5).
Summary of Evidence Evaluating the Outcomes of Patients After Holmium:Yttrium Aluminium Garnet Laser Ablation Treatment of Recurrent Bladder Tumor Non-Muscle Invasive Bladder Cancer
n.a. = not applicable; MIBC = muscle invasive bladder cancer; NMIBC = non-muscle invasive bladder cancer.
Tumor recurrence rates varied significantly between studies, ranging from 0% to 73%. One of the reasons for this is the differences in the proportions of original tumor histological grades and stages between studies. Our current study found significant differences in tumor recurrence, progression, and CSM when comparing patients with differing original histological tumor grades and stages. Another reason for this variation is the differences in follow-up periods and frequency surveillance cystoscopy. The sub-population studied have all had at least one tumor recurrence to be included in these studies, so one would suspect higher rates compared with a population with primary bladder tumors. Interestingly, we found that the overall average time to tumor recurrence was more than 16 months, which is longer than the follow-up periods for the majority of the other studies. For the reasons just cited, the current evidence from the literature regarding tumor recurrence rates is non-comparable.
Syed and colleagues 20 reported the only tumor progression data in the literature. They found a tumor progression rate of 6% for patients with G3pT1 as the original histology over a 24-month follow-up. 20 In this study, the overall tumor progression rate was 19.1%, with 5.6% progression to muscle invasive disease. The majority of these patients had either G3 or T1 disease. Of the 17 patients who had G3pT1 disease, 6 (35.5%) progressed to muscle invasive disease with an average time of 34 months. The higher rate of progression in our series is due to the longer follow-up period as only 1 (5.8%) patient had tumor progression before 24 months, making both studies comparable. Tumor progression to muscle invasive disease in the lower grades (G1 and 2) and stage (Ta) was rare, with only 0%, 1%, and 4.1%, respectively.
Our study population was elderly with significant co-morbidities, with the majority being assessed as ASA 3 or 4. Many were not deemed fit or declined formal TURBT under general anesthesia. This significantly influenced the overall mortality rate, which was 25.5%, with the main risk factors being age older than 77 years and original histology tumor grade 3. Despite this, we only encountered 5.2% CSM in the study with an average time to death of ∼6 years. The only significant risk factors that influenced this were original tumor grade and stage, with a trend toward older patients having more chance of CSM.
Current evidence for the outcomes after treatment for NMIBC are based on standard TURBT using the European Organisation for Research and Treatment of Cancer risk calculator, which contains the combined data of 2596 patients with a median follow-up of 3.9 years. 7 Despite the widespread use of laser ablative techniques for management of recurrent disease, there are no validated predictive nomograms of outcomes for these patients. We believe that our study can, therefore, be a useful guide for patient counseling in terms of providing long-term data of tumor recurrence, progression, and CSM for patients with recurrent NMIBC after laser tumor ablation.
Although treatment cost was not analyzed in this study, Planelles-Gomez and colleagues compared the cost of laser tumor ablation under topical anesthesia with formal TURBT under general anesthesia for recurrent NMIBC and calculated an overall saving of €2,007.09 per procedure with laser treatment with comparable safety profiles. 22 Wong and colleagues evaluated the cost difference between laser tumor ablation under topical anesthesia and cysto-diathermy under general anesthesia for recurrent NMIBC and found that over the course of a patient's lifetime, laser ablation was more clinically effective, measured in quality-adjusted life-years, than cysto-diathermy and less costly (£2576.42 [standard deviation = £7293.07]). 21
There were some limitations in our study. A minority of patients declined formal bladder biopsies or repeat TURBT; therefore, histological progression may have been under-represented, with delays in subsequent management that could have led to poorer CSM. Due to the high proportion of patients with significant co-morbidities, the overall mortality rate was high at 25.5% at just more than 6 years follow-up, which inevitably affects the reported outcomes. Although all patients had immediate post-operative intravesical mitomycin C at the time of the primary TURBT, intermediate and high-risk groups had further intravesical therapy (either maintenance mitomycin C or induction and maintenance BCG) through the course of their management according to the clinical need and wishes of the patients. This would affect the tumor profile and, ultimately, outcome.
In conclusion, outpatient Ho:YAG laser tumor ablation is a safe alternative to both TURBT or cysto-diathermy under GA for recurrent NMIBC, particularly in the elderly and co-morbid subpopulation with low-risk disease. Procedure tolerance and patient satisfaction were excellent. Long-term cancer outcomes are encouraging and although tumor recurrence rates were high, progression to MIBC and CSM was very low and mainly affected patients with grade 3 or stage T1 disease at initial histology. Careful patient counseling is required, and optimal outcomes are achieved in younger patients with low-grade and low-stage disease.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.