
Abstract
Purpose:
To investigate the difference, if any, in the quality of life (QoL) at specified intervals in patients undergoing same day discharge (SDD, ambulatory) vs next day discharge (NDD) after robot-assisted laparoscopic prostatectomy (RALP).
Materials and Methods:
Two hundred consecutive patients underwent RALP with either SDD or NDD. They completed validated pain and health-related QoL questionnaires at predefined intervals postoperatively and results were compared between the two groups.
Results:
Pearson's coefficient revealed significant correlations between the time of discharge and physical well-being (r = −0.139; p = 0.005), emotional well-being (EWB) (r = −0.71; p < 0.001), functional assessment of cancer therapy-general (FACT-G) (r = −0.367; p < 0.001), functional assessment of cancer therapy-prostate (FACT-P) (r = −0.273; p < 0.001), pain severity score (PSS) (r = 0.237; p < 0.001), and pain interference score (PIS) (r = 0.214; p < 0.001). Student's t-test revealed significant (p < 0.001) difference in the means of PSS, PIS, EWB, FACT-G, and FACT-P between both groups. Time of discharge was found to be an independent significant predictor (p < 0.01) of PSS and PIS. Pearson's coefficients revealed that PSS had significant correlations with age (r = −0.60; p < 0.001), body mass index (r = 0.87; p < 0.001), and console time (CT) (r = 0.63; p < 0.001). CT also correlated with the estimated blood loss (r = 0.65; p < 0.001).
Conclusions:
Patients who were discharged the same day as their RALP had lesser pain and interference in general activity scores 2 days after discharge and had better perceived overall health than patients who were discharged on postoperative day 1.
Introduction
Trends in the surgical management of diseases are shifting from minimally invasive to “minimally admissive” synonymous with same day discharge (SDD). Anterior urethroplasty, robot-assisted laparoscopic prostatectomy (RALP), and laparoscopic nephrectomy with SDD are safe. 1 –5 Over 5 years, outpatient urologic surgeries have risen from 26% to 42%. 6 Expectedly improved surgical and anesthesia techniques, evolving instrumentation, accumulated experience, payors pressure, and changing perspectives shall all lead to increasing number of surgeries falling into the domain of SDD.
Merriam-Webster dictionary describes “quality of life” (QoL) as the happiness, independence, and freedom available to an individual. 7 Numerical scales derived from validated questionnaires exist to quantify QoL. These are responsive, sensitive to changes, and reliable for scientific use. QoL post-RALP is impacted by factors such as the psychologic impact of surgery, catastrophizing, catheterization, admission duration, and status of continence/potency. SDD provides comparable functional outcomes at 45 days in terms of continence and erectile capabilities, but their final impact is manifested only later. 8 Patient-reported QoL early during recuperation has rarely been investigated. To the best of our knowledge, this is the largest study relating time of discharge to change in QoL indices within 7 days of RALP.
This study was designed and conducted to establish whether SDD patients perceived pain differently at 2 days and whether there was any deterioration in QoL indices at 7 days compared with patients discharged the next day. The secondary objective was to establish whether time of discharge is predictive of subsequent pain and QoL indices. We hypothesized that SDD patients were no different at 48 hours and at 1-week after surgery from NDD. One hundred patients in each group were interviewed about their pain and QoL using standardized questionnaires at predetermined time intervals, to establish the validity of our hypothesis.
Materials and Methods
After the institutional review board's approval (protocol no. LCH-1-11), this study of 200 consented men undergoing RALP at a single high-volume center performing >200 RALPs every year was conducted. This article was written according to the Strengthening The Reporting of OBservational studies in Epidemiology (STROBE) checklist v4 cohort guidelines. 9
Study design
Prospective observational study. Considering our primary outcomes a priori-power calculation determined that at least 180 subjects would enable us to observe a difference of 3–5% between next day discharge (NDD) and same day discharge (SDD) groups with a power of 80%.
Exclusion criteria
Absolute number of patients are in parentheses. Excluded were patients with American Society of Anesthesiologists (ASA) score ≥4 (13), body mass index (BMI) ≥35 (19), salvage procedures (2), untreated clinical depression (1), readmission within a week (0), patients who refused allotment to SDD (9), and patients who missed their scheduled appointment after discharge (4).
Surgical procedure
All patients were counseled about the expected course of treatment and time of discharge. Everyone underwent RALP by the standard transperitoneal six-port technique using the da Vinci surgical system Si (Intuitive Surgical, Sunnyvale, CA) by a single surgeon.
Anesthesia protocol
Enhanced recovery after surgery protocols and a multimodal approach for pain control were adopted, facilitating faster recovery. Minimal narcotics usage marginalized negative side effects. Anesthesia was induced using short acting agents midazolam (2 mg), propofol (150 mg), fentanyl (100 μg), and rocuronium (50 mg). For its ease of titration to expedite emergence, desflurane was chosen for maintenance. Rocuronium paralysis was maintained with 0/4 twitches to train-of-four while the robot was being docked, facilitated by quick reversal with Suggamadex™, minimizing residual muscle weakness. Acetaminophen (1 g) was administered intravenously (IV) 30 minutes before port extraction, causing peak effect to occur on arrival to postanesthesia care unit. Metoclopramide (10 mg), dexamethasone (10 mg), ondansetron (4 mg), and scopolamine transdermal patch were administered for prevention of postoperative emesis.
Postoperative instructions
Every patient received 30 mg ketorolac IV q.i.d. and acetaminophen (300 mg) with codeine (30 mg) t.i.d. corresponding to 13.5 mg morphine equivalent dose until discharge along with parenteral cefazolin. Discharge instructions were to rest with legs being nondependent, walking 100 yards per hour, turning around when in bed, incentive spirometry, high residue diet, and plenty of oral fluids. Acetaminophen (650 mg) t.i.d. (along with codeine only for the 24 hours after discharge), milk of magnesia (30 mL b.i.d.), docusate sodium (100 mg) b.i.d., and levofloxacin (500 mg) q.d. were prescribed for 5 days.
Breakthrough pain analgesia protocol
Breakthrough pain, defined as a pain score ≥4 or an increase in pain by one unit on a numerical pain scale, was treated with ketorolac 30 mg IV in post anesthesia care unit and on the floor if patient was admitted. After discharge, patients were instructed to take additional acetaminophen with codeine as needed for breakthrough pain.
Discharge group assignment
Patients were allocated to be discharged either on the same day or the next day of surgery. Nine patients voluntarily opted out of SDD and were discharged the next day but they were excluded from the study. One hundred patients were discharged within 8 hours after surgery, with a pain score ≤3. These were categorized as the SDD group. Another 100 patients similar in demographics and clinical and preoperative parameters, but discharged 24–36 hours after surgery, formed the control, NDD group (Table 1).
Demographics and Perioperative Features of Same Day Discharge and Next Day Discharge Groups
Data are mean ± SD.
ASA = American Society of Anesthesiologists; AUA = American Urological Association; CI = confidence interval; NDD = next day discharge; SD = standard deviation; SDD = same day discharge.
SDD patients were discharged home with Foley catheter in place, clear liquids tolerated, and after ensuring 50 yards mobility with partial assistance and acceptable functional recovery. A nurse or nurses aide accompanied SDD patients' home to monitor vital signs and ensure compliance, till next morning 6 am. NDD patients were discharged with similar instructions.
Each patient followed up in clinic 48 hours after surgery for brief pain inventory (BPI) data acquisition and on seventh postoperative day for Foley catheter removal along with estimation of health-related quality of life (HRQoL) indices by Functional Assessment of Cancer Therapy-Prostate (FACT-P) questionnaire.
Questionnaires and data collection
Qualified personnel (fellows and residents) not involved with surgery filled the survey forms, eliminating interpretation bias.
Fourty-eight hours postsurgery
The BPI was developed from the Wisconsin Brief Pain Questionnaire to evaluate the least, worst, and instantaneous pain intensity providing a pain severity score (PSS). 10 Assessing pain's interference on daily living gave an interference score (PIS). BPI is a robust tool commonly adopted in various clinical, epidemiologic, and research studies. It has been validated for use in postoperative patients and in various languages and has been utilized in >400 studies to date. 11,12 High test–retest reliability with excellent criterion validity and internal consistency has been demonstrated. 13,14 BPI scores were directly proportional to the quantum of pain and activity interference. Anchoring bias was prevented by not divulging scores to the patients.
Seventh postoperative day
For QoL assessment in cancer patients, a variety of instruments are available. Some measure general health, whereas others are prostate cancer-specific instruments. The widely used general cancer instrument is the functional assessment of cancer therapy-general (FACT-G), which is a miscellany of questions pertaining to general QoL, answered on a Likert-type scale. It has four well-being subscales: physical well-being (PWB), social/family well-being, emotional well-being (EWB), and functional well-being. The overall FACT-G score is the sum of all these subscales.
FACT-P is the most widely used prostate cancer-specific instrument. It incorporates FACT-G along with a prostate cancer subscale that quizzes about prostate cancer-specific QoL issues of sexuality, bowel and bladder functions, and generalized pain. Psychometric studies have validated all the components of FACT-P. 15
An office nurse removed the Foley catheter and every patient's FACT-P was completed by the same interviewer. In situ Foley catheter made patients incapable of answering questions pertaining to continence and erections that resulted in prorating scores as per prescribed guidelines. The responses of the negatively stated questions were appropriately reversed so that all response frequencies were in the same direction. All subscale totals were obtained. Higher score in any FACT scale implied a better QoL in that index.
All qualitative information so collected was thus converted to nondichotomous ordinal numerical data for quantitative analysis later.
Statistical analysis
Hierarchical multiple regression (HMR) analysis was done to find unique and independent relationships between patient demographics, clinical features, perioperative data, and discharge time. Four models were created to show the incremental predictive value of postoperative HRQoL index scales, from the variables within each model. Model 1 contained age, ethnicity, and BMI. Model 2 added ASA and American Urological Association score, biopsy Gleason score, clinical staging, Charlson index, D'Amico grading, and prostate specific antigen. Model 3 included prostate weight, tumor volume, pathologic features, estimated blood loss (EBL), and console time (CT). Model 4 added discharge time. Pearson's correlations were used to examine the bivariate associations between discharge time and HRQoL scales. Student's t-test and chi-square were used to compare groups in continuous and categorical variables, respectively.
All statistical analyses were performed using SPSS v.22.0 software (IMB, Chicago, IL).
Results
Data were collected using standardized validated questionnaires at predetermined time intervals. Descriptive statistics with mean, standard deviation, and median were used to express the collected data unless otherwise specified. SDD and NDD had 100 patients each, analyzed as per the study protocol. No difference was observed in the demographic, clinical, and perioperative characteristics between SDD and NDD except for the earlier time of discharge since surgery (8.6 hours vs 30.5 hours, p < 0.001) (Table 1).
Pearson's correlation coefficient revealed significant correlations between the time of discharge and PWB (r = −0.139; p = 0.005), EWB (r = −0.71; p < 0.001), FACT-G (r = −0.367; p < 0.001), FACT-P (r = −0.273; p < 0.001), PSS (r = 0.237; p < 0.001), and PIS (r = 0.214; p < 0.001) (Table 2). Student's t-test revealed a significant (p < 0.05) difference in the means of PSS, PIS, FACT-G, FACT-P, and EWB between both groups (Fig. 1). Pearson's coefficients revealed that PSS had significant correlations with age (r = −0.60; p < 0.001), BMI (r = 0.87; p < 0.001), and the CT (r = 0.63; p < 0.001). CT also correlated with the EBL (r = 0.65; p < 0.001) (Fig. 2). We did not find any associations with the time of discharge and the remaining HRQoL indices (Table 3).
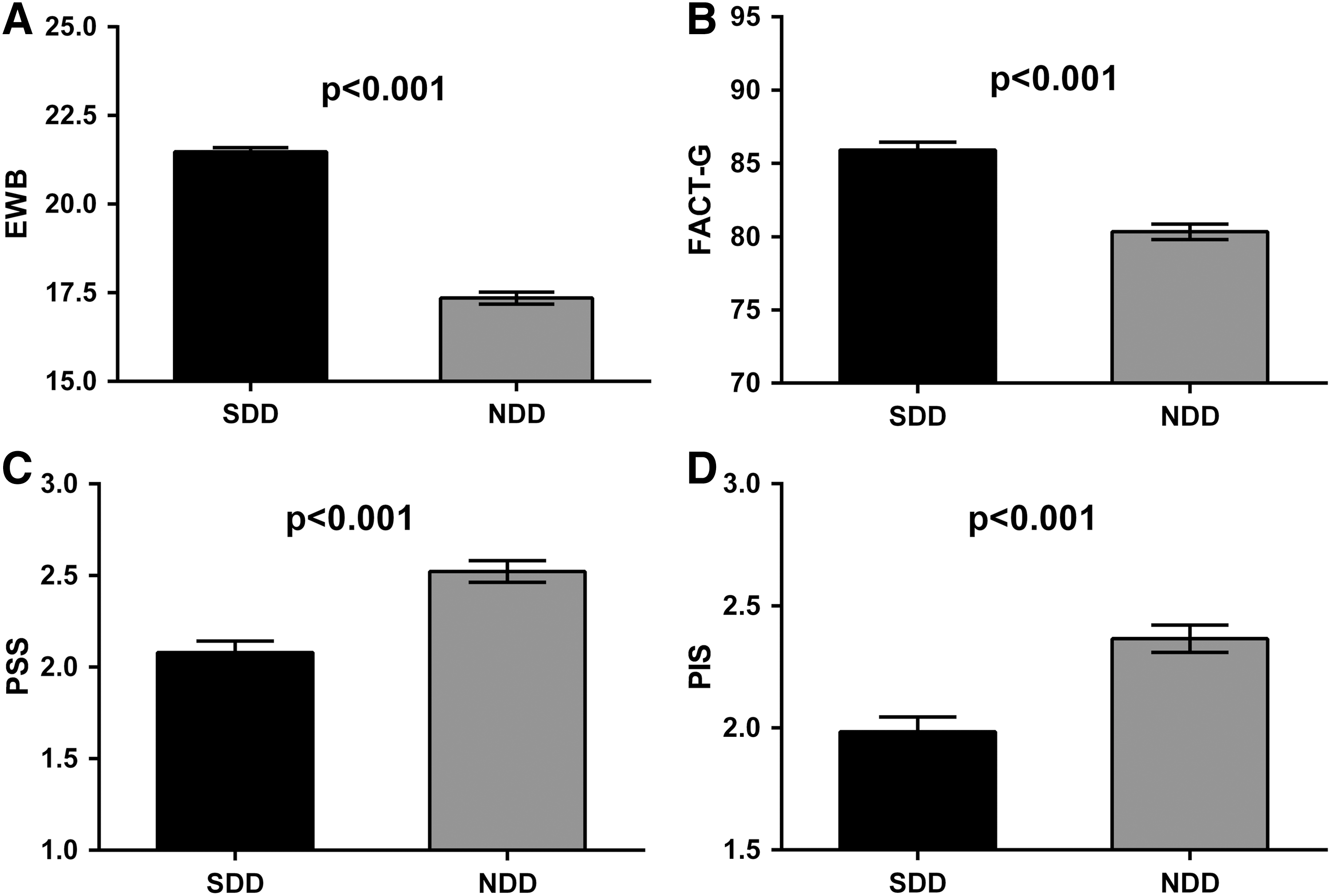
Group differences in the QoL indices between SDD and NDD. Data are mean ± standard error of the mean.
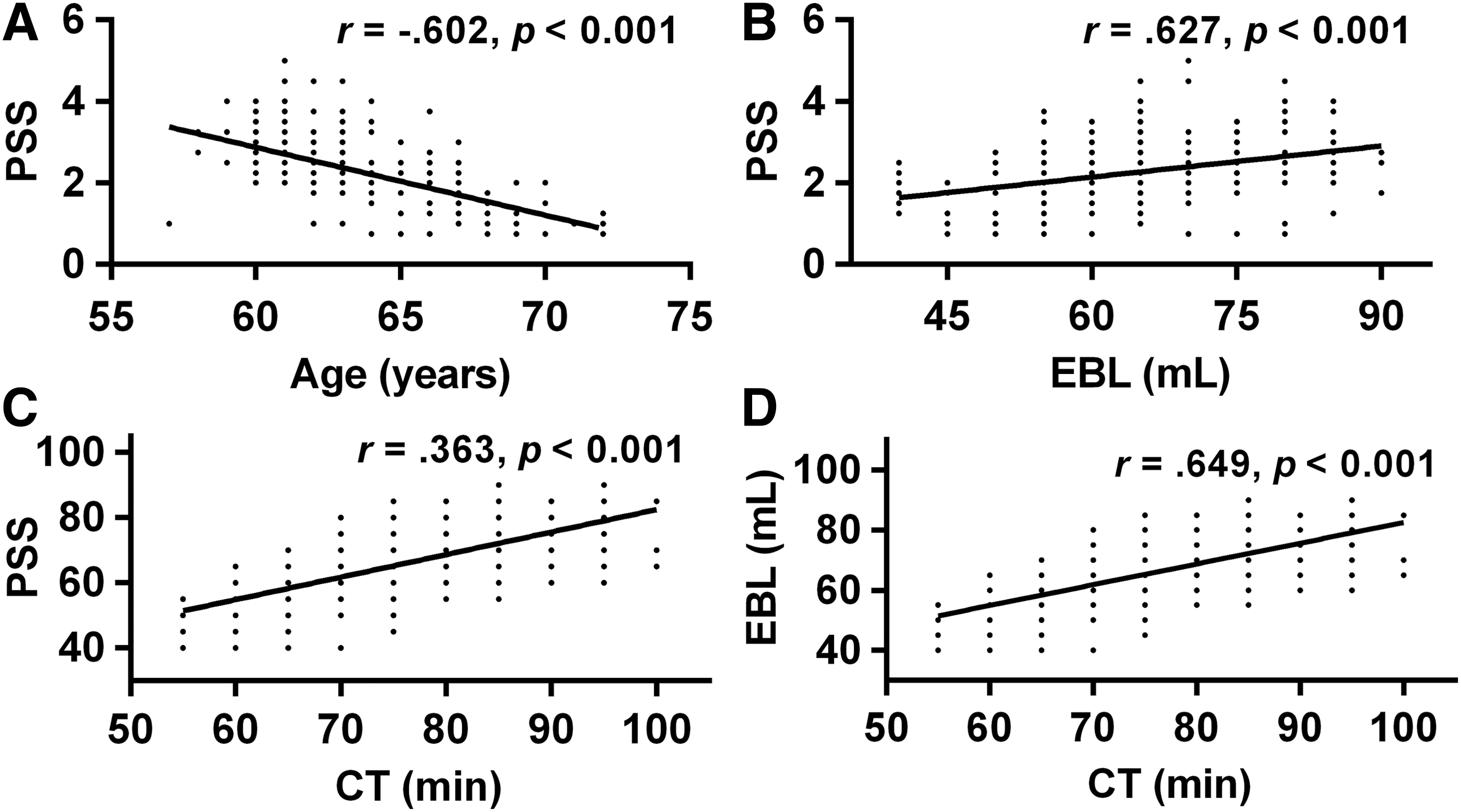
Bivariate relationships between selected variables. Data are mean ± standard error of the mean. CT = console time; EBL = estimated blood loss.
Pearson's Correlation Matrix
Correlation is significant at the 0.01 level (two-tailed).
Correlation is significant at the 0.05 level (two-tailed).
Data are mean ± SD.
EWB = emotional well-being; FACT-G = functional assessment of cancer therapy-general; FACT-P = functional assessment of cancer therapy-prostate; FACT-P PS = functional assessment of cancer therapy-prostate pain score; FWB = functional well-being; P cancer = prostate cancer; PIS = pain interference score; PSS = pain severity score; PWB = physical well-being; SWB = social well-being; TOI = trial outcome index.
Brief Pain Inventory and Health-Related Quality of Life Scores
Data are mean ± SD.
BPI = brief pain inventory.
HMR analysis revealed that time of discharge was an independent significant predictor of PSS and PIS 2 days after discharge (p < 0.01) and of EWB and FACT-G 7 days after discharge (Table 4).
Hierarchical Multiple Regression Details for Pain Severity Score, Pain Interference Score, Emotional Well-Being, and Functional Assessment of the Cancer Therapy-General as Dependent Variables
Data are mean ± SD.
PSS = Pain Severity score.
Eight patients from SDD were migrated to NDD after being admitted because of suboptimal respiratory status (3), more than minimal hematuria (2), and breakthrough pain (3). Four patients in NDD had breakthrough pain that required additional analgesia. After discharge, one patient in each group had to take additional analgesia for breakthrough pain. However, all these patients fell inside the 95% confidence interval for the tested outcome variables.
Discussion
The study aimed to evaluate the impact on QoL of SDD in comparison with NDD, after RALP. The novel results demonstrate SDD improves some parameters of HRQoL early and 7 days after discharge, which seems to suggest that an early discharge approach is desirable.
“Trifecta” comprising oncologic control and return of erections with urinary continence measures RALP's outcomes. Main components of RALP-related QoL are the latter two. Perfect continence and erections are achieved weeks after surgery, hence most studies measuring them have been done long after RALP. 16 QoL measurement soon after surgery necessitates different parameters and instruments, quantifying the impact of surgery/postoperative care. Furthermore, at 7 days the recall potential of details is high in contrast to studies done later in time. As postoperative pain is experienced maximally within the first 48 hours causing utmost disruption in HRQoL in the first week, we evaluated patients with relevant instruments at these time intervals. 17,18 The preoperative cognitive preparedness about pain and its remedial measures helps in reducing pain perception and analgesic requirements. This may have contributed to both groups of our patients having low PSS and PIS scores. Post operative pain is contributed by trocar incisions, bladder spasms, and Foley catheter related discomfort. Actual pain scores reported by patients may have been on the higher end of the spectrum because of these added confounders. In the SDD group, within 7 days of discharge, emergency room visits were for low grade fever (1), hematuria (1), and nausea (2). In the NDD group, the visits were for hematuria (1) and constipation (2) (p = 0.7). All were Clavien Dindo class 1, needing no admission. Discharge time was significantly negatively correlated with PWB, EWB, FACT-P, and FACT-G, and positively correlated with PSS and PIS. Pearson's coefficient assumes a perfect linear relationship between the variables that is not flawless, subsequent analysis of variance nullified the difference in PWB and FACT-P when all other parameters were accounted for.
HMR showed SDD to be the single most important predictor of lower PSS and PIS scores and higher EWB and FACT-G scores. EWB depicts how the patient feels emotionally and is independent of his social interactions. FACT-G total score was expectedly better in SDD as EWB is one of its components. Thus, improvement of emotional status alone can lead to an overall better QoL, all other parameters remaining constant. Remarkably, better FACT-G score did not translate into improved social interactions or into better functionality like ability to continue working. It is noteworthy that the FACT-P scores did not show any significant difference in HMR. Between SDD and NDD, means of all the contributing variables of PSS were significantly different (p < 0.05), but means of only walking ability and general activity components were different in PIS (p < 0.05), on Student's t-test.
BMI positively correlated with PSS in both groups. A similar correlation has been demonstrated by Chung et al. 19 A higher BMI and increased CT also independently predicted a higher PSS. In agreement with this study, a negative correlation of advancing age with decreased PSS was reported by Chang. 20 Suggestions exist that the peripheral painful stimulus is altered in the elderly leading to decreased pain perception, additionally notwithstanding the blunting of mental faculties and under-reporting of pain with aging. 21 It has been proposed that the influence of certain pain perceiving genes is also altered with age. 22 All this implies that younger patients perceive pain to a greater extent and the same conclusion was attained by Ene KW et al. after robotic prostatectomy. 23
Since opioids can potentially prolong hospital stay, they were used for only 24 hours postoperatively. This strategy was authenticated by Joshi GP et al. 24 CT was positively correlated with EBL and higher PSS, suggesting that when additional time was spent on hemostasis, it led to higher PSS. This was in accordance with the findings of Chung and colleagues that higher surgical times lead to increased pain. 19 Wolboldt reported larger blood loss after laparoscopic prostatectomy in patients going home the same day. 2 We did not find the same correlation (p = 0.07). With increasing operator experience, EBL and CT decrease and that may translate into better QoL later.
Limitations
Surgery-associated psychoemotional stresses especially anxiety and individual pain tolerance are capable of confounding the QoL assessment postoperatively. We could not negate them. To eliminate single-surgeon bias and achieve generalization, we need multicenter studies, with more power and different surgeons.
Conclusions
SDD discerned significantly lesser pain and interference with general activities, along with better EWB and overall general health perception than NDD. SDD was found to be an independent predictor of all these parameters. No such correlation was found between other indices. These findings are adequate to conclude that SDD is superior to NDD at least in the first week after discharge. Further experimental studies are warranted to explore other implications of SDD, including cost-effectiveness and the achievement of the trifecta.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.