
Abstract
Introduction and Objectives:
Fluoroscopy units are routinely operated in the automatic brightness control (ABC) mode to optimize image quality. During ureteroscopy, objects may be placed within the fluoroscopy beam and the effect upon radiation exposure is unknown. The purpose of this study is to investigate the effects of equipment within the fluoroscopy beam during simulated ureteroscopy.
Methods:
ABC fluoroscopy of a cadaver was performed in eight clinical scenarios, including a control (no equipment), and seven groups with different equipment within the fluoroscopy beam. Equipment tested included electrocardiogram (EKG) leads, a Kelly clamp, camera and light cords (straight and coiled configurations), flexible ureteroscope, rigid cystoscope, and the lateral table support beam. Ten 145-second fluoroscopy trials were performed for each arm. The primary outcome was radiation dose (mGy) compared using the Mann–Whitney test with p < 0.05 considered significant.
Results:
Compared with control (18.5 mGy), radiation exposure was significantly increased with the presence of a straight camera and light cords (19.3 mGy), Kelly clamp (19.4 mGy), coiled camera and light cords (20.2 mGy), a flexible ureteroscope (21.0 mGy), a rigid cystoscope (21.2 mGy), and when the lateral table support beam was in the path of the X-ray (25.0 mGy; a 35% increase; p < 0.007 for all). The EKG leads did not affect the radiation dose.
Conclusions:
Avoiding equipment within the fluoroscopy beam using ABC mode can reduce radiation exposure. Adjusting the table and patient position to exclude the lateral table support beam will reduce radiation exposure by 35%.
Introduction
Ureteroscopy has become the most common surgical treatment for upper tract stones, 1 with the majority of these procedures performed using fluoroscopy. 2 The urologists performing these fluoroscopic-guided procedures are also exposed to significant amounts of radiation. 3 Although both reduced fluoroscopy protocols 4 and fluoroless ureteroscopy have been described, 5 the majority of urologists still employ fluoroscopy during multiple steps of the procedure. The amount of fluoroscopy required increases with the complexity of the case. 6 Owing to the potential harmful effects of ionizing radiation, efforts should be taken to reduce the exposure to the patient and surgeon to as low as reasonably achievable (ALARA). 7
Fluoroscopy machines can be operated in two modes, including automatic brightness control (ABC) or manually fixed settings. 8 The ABC setting is the most common modality used during fluoroscopy and provides optimal image quality by adjusting the milliampere-seconds (mAs) and peak kilovoltage (kVp) in response to the density of the target being imaged. 9,10
During ureteroscopy, surgical equipment (light and camera cords, clamps, and endoscopes) may be placed overlying the drape in the direct path of the X-ray beam. Although ABC maintains optimal image quality, the effects of its use on radiation exposure in the presence of different surgical equipment in the fluoroscopy beam has not been well characterized. The purpose of this study is to determine the effect of equipment clutter in the path of the fluoroscopy X-ray beam on the amount of radiation used during simulated ureteroscopy in a cadaveric model.
Materials and Methods
After the approval of the Loma Linda University's department of pathology and human anatomy, and in compliance with institutional policies for use of anatomical specimens in research, a male cadaver (height 170 cm and body mass index 24.6) was used in a simulated ureteroscopy model. The cadaver was positioned and draped in lithotomy in an identical manner to that employed during clinical ureteroscopy (Fig. 1). The cadaver underwent fluoroscopy using the ABC mode simulating a right ureteroscopy.

The cadaver is placed in the supine lithotomy position on the operating room table with the C-arm source below, and the image intensifier above the patient to simulate clinical ureteroscopy.
Fluoroscopy was performed using a GE OEC 9900 portable C-arm system (GE Medical system, Inc., Salt Lake City, UT) in the ABC setting. Pedal activation was accomplished from a lead-lined control room. The equipment used to simulate the clutter in the fluoroscopy beam included three EKG leads (including electrodes and connecting wires), a Kelly clamp, the beam splitter camera head and light cord in straight configuration (HD Pendulum Camera Head; Olympus Corporation of America, Center Valley, PA), the beam splitter camera head and light cord in a coiled configuration, a flexible fiber optic ureteroscope (URF-P6; Olympus Corporation of America), a rigid cystoscope (22F; Olympus Corporation of America), and the lateral table support beam on the fluoroscopy table (TruSystem 7000 OR Table; Trumpf Medical Systems, Inc., Charleston, SC) (Fig. 2).

Equipment placement and fluoroscopic images obtained during simulated ureteroscopy:
Ten trials were performed for each arm with total fluoroscopy time of 145 seconds per trial, based on our previous description of average fluoroscopy time during ureteroscopy. 11 The C-arm was positioned over the ipsilateral UPJ in the conventional supine lithotomy position employed for ureteroscopy. The X-ray source was positioned below the table and the image intensifier was positioned above the patient with an identical skin to source distance of 30 cm maintained in all trials. Fluoroscopy was set to the default conventional ABC setting with a continuous rate of 30 pulses per second for all the study arms.
The primary outcome in this study was the total radiation delivered by the fluoroscopy machine in milligray. The secondary outcomes were the kVp and mAs readings of the machine for each trial. The Mann–Whitney U test was performed to compare mean radiation exposure between the control and experimental arms. To control for the increased likelihood of a type I error caused by performing multiple comparisons with nonparametric tests, the Bonferroni correction was used to calculate the adjusted level of significance as p < 0.007. Analysis of variance (ANOVA) and Tukey's B post hoc were used to compare the radiation exposure between different experimental groups (p < 0.05).
Results
During 145 seconds of ABC fluoroscopy activation with no equipment in the beam path (control), the mean radiation exposure delivered by the C-arm in the 10 trials was 18.53 mGy (Table 1). Compared with the control, the radiation dose was significantly increased in six out of seven treatment conditions where equipment clutter was left within the radiation beam. These conditions included the beam splitter camera head and light cord in a straight configuration (19.30 mGy; p = 0.005), a Kelly clamp (19.38 mGy; p = 0.002), the beam splitter camera head and light cord in a coiled configuration (20.25, p = 0.001), a flexible ureteroscope (21.05 mGy; p < 0.001), a rigid cystoscope (21.20 mGy; p < 0.001), and when the lateral table support beam was included in the x-ray beam path (25.01; p < 0.001) (Fig. 3).

Mean radiation dose (mGy) produced by fluoroscopy machine with different equipment placed in the path of the X-ray beam. *Statistical significance. EKG = electrocardiogram.
Mean Radiation Dose (mGy) and % Increase from Control with Different Equipment Placed in the Path of the Fluoroscopy Beam
The presence of the EKG leads within the beam path did not have a significant effect upon the radiation level (p = 0.1211). The inclusion of the lateral table support beam in the path of fluoroscopy resulted in the largest increase (35%) for radiation delivered by the fluoroscope compared with the control (Fig. 4).

Percentage increase in total radiation dose (mGy) compared with control (no equipment in path of X-ray) produced by fluoroscopy machine with different equipment placed in the path of the X-ray beam. *Statistical significance.
Comparison of mAs and kVp values were also consistent with total radiation results. The control group had the lowest mean mAs (2.16 ± 0.02) and kVp (79.9 ± 0.31) values. All equipment mAs and kVp values were significantly higher compared with the control group except for the EKG leads and the camera and light cords in a straight configuration.
Mean values of mAs and kVp were as follows: EKG leads (2.17 ± 0.01 mAs; p = 0.282 and 80.00 ± 0.00 kVp; p = 0.317), camera and light cords in a straight configuration (2.19 ± 0.02 mAs; p = 0.010 and 80.40 ± 0.5 kVp; p = 0.021), a Kelly clamp (2.20 ± 0.02 mAs; p = 0.002 and 80.6 ± 0.51 kVp; p = 0.004), camera and light cords in a coiled configuration (2.24 ± 0.03 mAs; p < 0.001 and 80.8 ± 0.42 kVp; p < 0.001), flexible ureteroscope (2.29 ± 0.04 mAs; p < 0.001 and 81.5 ± 0.5 kVp; p < 0.001), a rigid cystoscope (2.30 ± 0.03 mAs; p < 0.001 and 81.4 ± 0.51 kVp; p < 0.001), and with lateral table support beam (2.50 ± 0.02 mAs; p < 0.001 and 84.70 ± 0.48 kVp; p < 0.001) (Figs. 5 and 6).
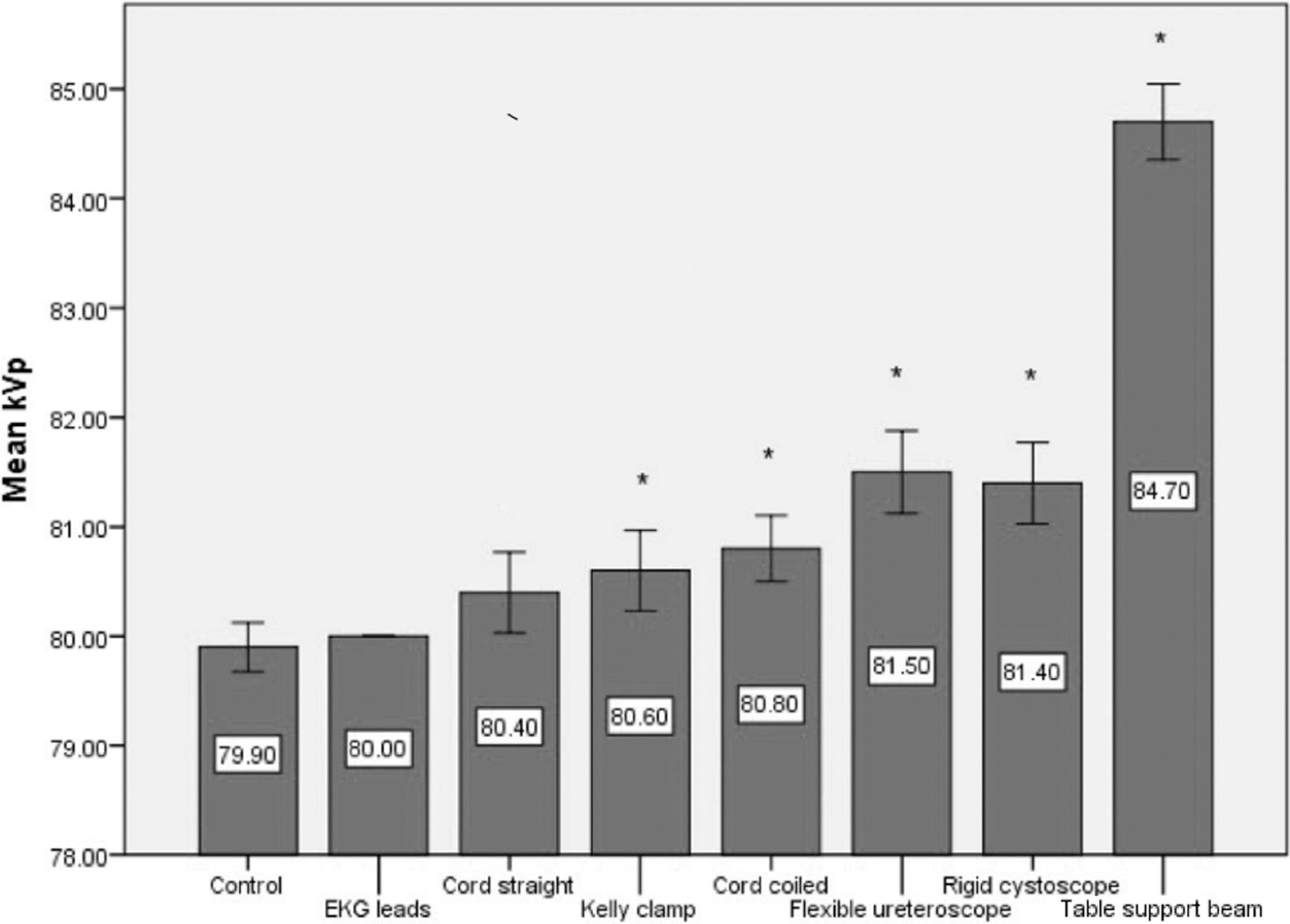
Mean kVp produced by fluoroscopy machine with different equipment placed in the path of the X-ray beam. *Statistical significance. kVp = peak kilovoltage.
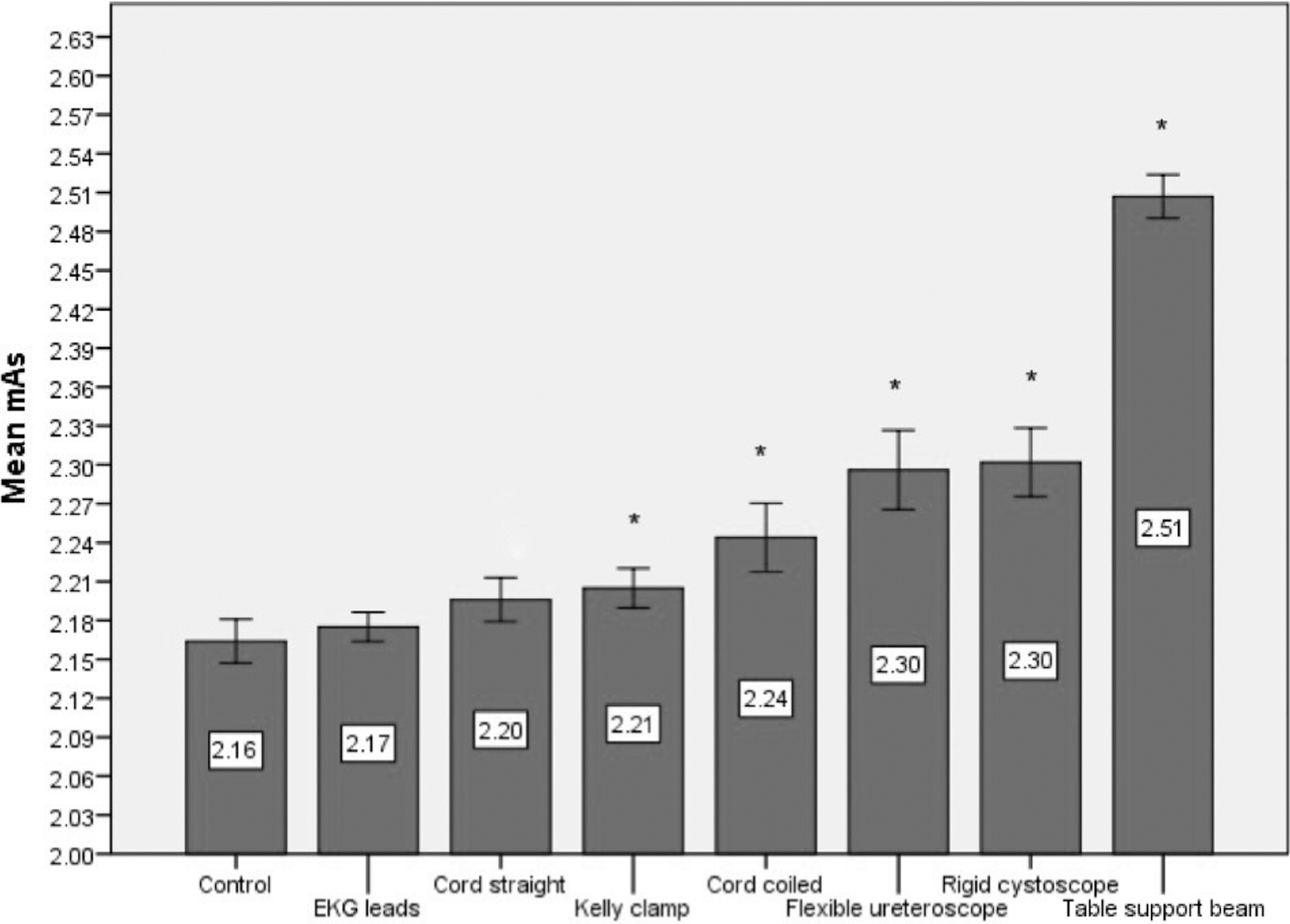
Mean mAs produced by fluoroscopy machine with different equipment placed in the path of the X-ray beam. *Statistical significance. mAs = milliampere-seconds.
ANOVA paired comparison with Tukey's B post hoc analysis between different experimental groups showed no significant difference in radiation exposure for EKG leads, camera and light cords in the straight configuration, and the Kelly clamp (Table 2). However, the camera and light cords in a coiled configuration had significantly more radiation exposure compared with the EKG leads, camera and light cords in the straight configuration and the Kelly clamp. The flexible ureteroscope and rigid cystoscope were similar to each other but greater than all other equipment except the lateral table support beam (p < 0.05). The lateral table support beam resulted in the highest increase in radiation exposure compared with all other experimental groups (p < 0.05) (Table 2).
Comparison of the Mean Radiation Dose (mGy) Between Different Equipment Placed Within the Path of the Fluoroscopy Beam
NS = not significant.
Discussion
There have been significant advancements in imaging technology for the past 30 years. 12 Although this has provided obvious benefits with improvement in medical diagnosis and treatment, it has been associated with a significant increase in the use of ionizing radiation. It has also been shown that most physicians underestimate the amount of radiation exposure associated with radiologic imaging. 13 In the United States, the annual radiation exposure per capita from medical radiation has increased from 0.54 mSv in 1980 to 3.0 mSv in 2006, an increase of 600%. 14 It has been estimated that up to 2% of all malignancies diagnosed in the United States result from medical imaging. 15 There is no safe minimum dose of ionizing radiation as the risk follows a linear no-threshold exposure model. 16
Nephrolithiasis is prevalent and rising, with an incidence of up to 13% in North America. 17 Patients with renal stones are at a higher risk for radiation exposure attributable to a recurrence rate of up to 50% within 5 years. 18 A study by Ferrandino and colleagues showed stone patients receive a median effective dose of 29.7 mSv from diagnostic imaging alone. In this study, 20% of patients received >50 mSv of radiation, which is higher than the National Council on Radiation Protection and Measurements (NCRP) recommended yearly occupational threshold, without considering the radiation received during intraoperative fluoroscopy. 19
The reduction of radiation exposure to patients and operating room personnel without compromising health care outcomes is of paramount importance. The implementation of basic strategies, such as lead aprons and thyroid protection serve as an effective initial step. A recent study demonstrated that radiation doses were reduced by >90% by usage of lead aprons and thyroid shields during ureteroscopy. 20 There are a number of strategies described to help reduce the radiation exposure when using fluoroscopy for image-guided procedures, including the use of collimation, pulsed fluoroscopy, last image hold, and placement of the image intensifier as close as possible to the patient. 21
A surgeon's familiarity with the fluoroscopy machine and its dose settings is also crucial for minimizing the effective dose. Our center has previously shown that switching from continuous (30 pulses per second) to pulsed fluoroscopy at 1 pulse per second will reduce the radiation exposure by 64%. 22 Although this is a step in the right direction, additional measures need to be taken to further reduce radiation exposure. This study highlights an often overlooked aspect of potential increased radiation exposure to both patient and surgeon during fluoroscopy. Our findings suggest that any significantly dense material placed into the path of the fluoroscopy beam has the potential to increase radiation exposure when operating fluoroscopy in the ABC setting.
We showed that the amount of increase in radiation exposure was dependent on the type of equipment placed in the path of the fluoroscopy beam. The head-to-head comparison of different equipment found a similar increase in exposure for the EKG leads, Kelly clamp, and camera and light cords in straight configuration. However, denser equipment such as the flexible ureteroscope and rigid cystoscope resulted in a significantly higher increase in radiation exposure. The lateral table support beam resulted in the highest increase in radiation exposure.
There are several important clinical recommendations that arise from the evidence revealed by our study. First, it is important to position the patient on the bed in a manner that the ipsilateral side does not overlap with the lateral table support beam as this resulted in a 35% increase in radiation exposure when the C-arm was operated in the ABC mode. Second, dense equipment, including endoscopes, should not be positioned overlying the surgical site within the fluoroscopy beam as these also resulted in up to a 14% increase in radiation exposure. Third, the position of the camera and light cords should be placed on the contralateral side outside the path of the fluoroscopy beam.
ABC is the most frequently utilized setting for fluoroscopic image guidance because of its capabilities of achieving optimal image quality. 8 This is done by an automatic increase of kVp and mAs until optimal image quality is achieved. With increased density and thickness of the target, the mAs is increased to generate more photons and the kVp is increased to raise the energy of photons, thus allowing for better penetration of the beam through the target to create a brighter and clearer image. The kVp and mAs levels necessary to obtain these images are automatically calculated through the comparison of a reference signal to a feedback mechanism from the ionization chamber or photodetector. 8
We have previously shown that shielding can cause a patient's tissue density to be overestimated, resulting in the values of kVp and mAs to be unnecessarily increased, leading to the patient receiving a higher dose of radiation while also hindering image quality. 10 However, a lead shield is much denser than the equipment commonly left within the fluoroscopy beam. This study was designed to determine the effect of leaving equipment within the fluoroscopy beam during ureteroscopy.
This study highlights the importance of avoiding clutter within the fluoroscopy beam during operation of the C-arm in the ABC mode. Another alternative, which can avoid this increase in radiation delivery caused by the sensor detecting dense material in the beam, is to operate the fluoroscopy machine using fixed and intentionally lowered mAs and kVp settings. Although this may decrease the image quality slightly, the mAs and kVp can be set to allow adequate recognition of important landmarks and surgical structures. While in ABC, if dense objects such as a lead shield or surgical equipment are in the fluoroscopic path the radiation dose will be increased. The results of our study indicate that fluoroscopy using ABC, performed while objects routinely used during ureteroscopy are within the beam path will lead to an unnecessary and inadvertent increase in radiation exposure and should be avoided.
This is the first study to evaluate the effect of equipment clutter in the path of the X-ray when using ABC fluoroscopy during urologic surgery. Use of a cadaver model and an actual operating room equipment and setting allowed for a realistic assessment of the effects of equipment clutter upon radiation exposure without endangering a patient. In our study, higher radiation doses were recorded when the X-ray passed through the patient and additional equipment to reach the image intensifier. Similarly, in a recent ureteroscopy-simulated phantom model study it was concluded that an increased thickness of the model resulted in higher radiation exposure. 23 Also, the fluoroscopy time of 145 seconds selected for our study is below some other reported ureteroscopic fluoroscopy times in the literature 24 and if longer fluoroscopy time was employed, the radiation exposure from equipment clutter while using ABC would be increased.
There are some limitations to our study. Although use of the cadaveric model closely replicates the anatomy of a live person, it is possible that it underestimates the density of the living human tissue caused by natural desiccation of the cadaver. Therefore, it is possible that the amount of radiation exposure when using ABC fluoroscopy is underestimated. A denser patient model would further increase the radiation exposure to the patient and surgeon. However, the use of live human subjects would have been unethical for such a study design, and a cadaver model is the most realistic and ethical model to evaluate the radiation exposure in multiple different settings as done in this study. We accounted for the most common scenarios of equipment clutter in urology (cords, clamps, EKG, endoscope, and lateral table support beam); however, there may be other equipment that could be placed in the path of the fluoroscopy beam.
The results of our study suggest that any significantly dense material placed in the path of ABC fluoroscopy will result in increased radiation exposure and should be avoided. Another limitation of this study is that we measured output from the machine instead of directly measuring radiation exposure using Thermoluminescent dosimeter (TLD) chips. Since we were trying to determine the effects of dense objects within the fluoroscopy beam, we could not place TLDs within the beam path as the density of the TLDs would themselves alter the radiation exposure.
Conclusion
The use of ABC fluoroscopy with surgical equipment clutter within the fluoroscopy X-ray beam results in an increase in radiation exposure. Careful positioning of the patient on the operating room table and avoiding inadvertent placement of equipment within the path of the fluoroscopy beam may reduce the radiation exposure by up to 35% and improve patient and staff safety.
Footnotes
Author Disclosure Statement
D. Duane Baldwin, MD, has the following disclosures: BARD: Speaker; Olympus America, Inc.: Consultant/Advisor, DARRT Medical, Inc.: Board Member/Officer; StepLite, Board Member/Officer; Cook Medical: Lecturer. There are no disclosures for the other authors.