
Abstract
Introduction and Objectives:
To evaluate ablative safety and efficacy of thulium–holmium:YAG (TL–HL:YAG) duo laser in renal conserving retrograde intrarenal surgery (RC-RIRS) in upper tract urothelial carcinoma (UTUC).
Materials and Methods:
A retrospective study was performed on 178 consecutive patients referred for consideration of RC-RIRS UTUC-eLA (endoscopic laser ablation) in a tertiary center (January 2005 to December 2018). Key data were recorded using a standardized study proforma.
Results:
After endodiagnostic procedure, 42 declined rigorous endosurveillance protocol and went elsewhere for alternative treatment, leaving 136 patients, of whom 35 patients dropped out (25.7%) after undergoing primary radical nephroureterectomy (RNU) (unsuitable for renal preservation). This was left with 101 candidates who continued UTUC conservative management (intention-to-treat [ITT] population). Mean follow-up (FU) for these 101 patients was 28.7 months. At last FU (range 3–144 months), 70 patients (69.3%) were recurrence free, 22 (21.8%) had endoscopically treated recurrences, and a further 9 (8.9%) had undergone RNU.
In the ITT population, kidney-preserving rate was 91%, whereas in imperative indications, it was 87.5%. Clavien–Dindo grade I complications only (self-limiting hematuria) were reported in 10%.
Conclusions:
Over a 13-year period, RC-RIRS UTUC treatment with the TL–HL:YAG duo laser was safe and oncologically noninferior to alternative combination laser energy technologies used for this indication.
Introduction
Although radical nephroureterectomy (RNU) is still considered the gold standard treatment of high-grade and stage upper tract urothelial carcinoma (UTUC), 1 new technologies might help to expand the limits of treating larger lesions beyond those suggested by the guidelines, especially if lower risk (grade and stage), in imperative cases, for palliative purposes, and when RNU is declined for whatever reason.
Since its introduction into urology in 1995, the holmium YAG laser (HL) quickly superseded the small 3F Bugbee 2 and became the cornerstone of retrograde intrarenal surgery (RIRS) in renal conserving (RC)-UTUC endoscopic laser ablation (eLA).
Improvement of endoscopic techniques and dedicated instrumentation over consecutive decades have contributed to expand the indications for RC-UTUC treatment. In 2018, the European Association of Urology (EAU) guidelines changed the UTUC threshold size suitable for conservative treatment from 1.5 to 2 cm. 3 The thulium YAG laser (TL) is a widely used endourology energy source for the treatment of benign prostatic bladder outlet obstruction. 4 Others described its use in bladder tumor resection. 5 The first report concerning its use in RC-UTUC endoscopic treatment was in 59 patients, published in 2011. 6 Two further reports were published in 2018 7,8 with smaller cohorts, corroborating our initial findings.
A combination dual wavelength TL–HL:YAG laser was routinely used in endoscopic treatment of UTUC in our tertiary referral national center, and this study reports outcomes data after 13 years of its use.
Materials and Methods
In a retrospective single national tertiary referral center (Department of Urology, “Cristo Re” Hospital, Rome, Italy) study, 178 consecutive UTUC-referred patients (January 2005–December 2018) underwent diagnostic single manufacturer (Karl Storz Endoscopy, Tuttlingen, Germany) semirigid ureterorenoscopic (7F tip) and flexible ureterorenoscopy (KSE, Flex X2s 2005–2014; Flex-XC 2014–2018) evaluation. Key data were recorded using a standardized study proforma. The tumor-ablating laser throughout was the combination TL–HL:YAG laser (Revolix Duo, LisaLaser, Katlenburg-Lindau, Germany) at 10 to 15 W power, with 270 μm fibers. Biopsies were made before ablation with a 2.2F 1 cm Nitinol basket (N-Circle, Cook Medical, Bloomington) and 3F flexible (Piranha, Boston Scientific, Marlborough) or reusable forceps (KSE, Tuttlingen, Germany), performing minimum three biopsies. Both voiding and in situ renal pelvis wash cytology were collected during treatment episode. All RIRS RC-UTUC-eTLA cases were performed by four expert endourologists (two from the host center doing the bulk of cases, one from the United States, and one from the United Kingdom). Each had previously performed ≥50 cases of RIRS RC-UTUC-eLA. High-risk RC-UTUC treatment was only performed in imperative cases, for palliation, or if patients refused RNU after appropriate counseling.
Endoscopic technique was standardized 6 : for all lesions, periodic urine wash cytology specimens, multiple biopsies (tumor and base), followed by TL coagulation of tumor and base were sequentially performed. For intrarenal inspection, an appropriately sized 35 cm long ureteral access sheath (Flexor, Cook Medical, Bloomington) was deployed after entire ureteral inspection on the way up and back down to the ureteral orifice, aiming to maintain low intrarenal pressures throughout.
Coagulated necrotic eTLA tissue was dislodged with the pulsed HL mode at identical power settings. Larger tumor fragments were removed with a Nitinol basket (N-Circle 2.2F 1 cm, Cook Urology, Bloomington). Treatment was concluded with Double-J ureteral stent(s) placement and a Foley bladder catheter overnight to minimize upper tract pressures and urine reflux alongside the Double-J stent(s). Ureteral stents were removed (local anesthesia) in the office after a week, or left in situ if patients required a second look (sensation of incomplete ablation, tumor >2 cm, or higher risk features). No patient received adjuvant intrarenal or intravesical adjuvant drug instillation unless indicated by coexistent bladder UC (urothelial cancer).
A single uropathologist in the local department of pathology evaluated and reported on all specimens according to the 2009 TNM classification system, and WHO grade staging 1973 9 and 2016. 10 For analytical purposes, grade 2 were treated as low-grade tumors. Tumor size was assessed by measuring it compared with basket 1 cm wide alongside.
Second-look RIRS was performed between 4 and 6 weeks for high-risk patients (vide infra) with imperative renal preservation indication(s) or when consistently refusing RNU from the outset, for tumors >2 cm, or when a surgeon was unconvinced of complete presenting lesion ablation at the first procedure for whatever reason. RNU was recommended–performed 4 to 6 weeks after first endoscopic diagnosis if found to have high-risk UTUC, (>2 cm, high grade, pT1, and multifocality), or during follow-up (FU) for grade, stage, or risk category progression, leading to patients' dropout of disease-free survival analyses.
Except patients requiring earlier second look, the following endosurveillance (ES) protocol was adopted: First ES with voided and in situ renal pelvis cytology wash at 3 months. For recurrence at first FU, and/or tumor >2 cm requiring staged ablation, three monthly ES was performed for the first year. If no recurrence, six monthly ES for 2 years was performed, then annually for a minimum of 5 years. Yearly Uro-CT or Uro-MRI for impaired renal function patients. At each endoscopic procedure, bladder voided and in situ wash cytology; absent or visible tumor, if neoplasia present; side; site(s); dimensions (compared with 1 cm basket alongside); pathologic grade and stage; were all prospectively recorded on the study proforma.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required and informed consent was obtained verbally from all individual participants included in the study.
Results
All FU results are shown in Figure 1. Thirteen patients (7.3% of the global population n = 176) underwent second look RIRS. Excluded from endpoint survival analyses were 42 patients (23.6%) who did not attend first FU; 8 of whom had high-risk features. These patients declined rigorous ES protocol and sought alternative treatment elsewhere. This left 136 patients of whom 35 (25.7%) underwent RNU. In the intention-to-treat (ITT) (n = 101) ES population, at 3 months, 51 patients (50.5%) were recurrence free, 50 patients (49.5%) had recurrences. Mean FU in the ITT-ES population was 28.7 months (range 3–144 months, standard deviation 29.4); median 18 months (interquartile range 25–75: 12–36). The number of patients starting the ES regimen each year is graphically shown in Figure 2.
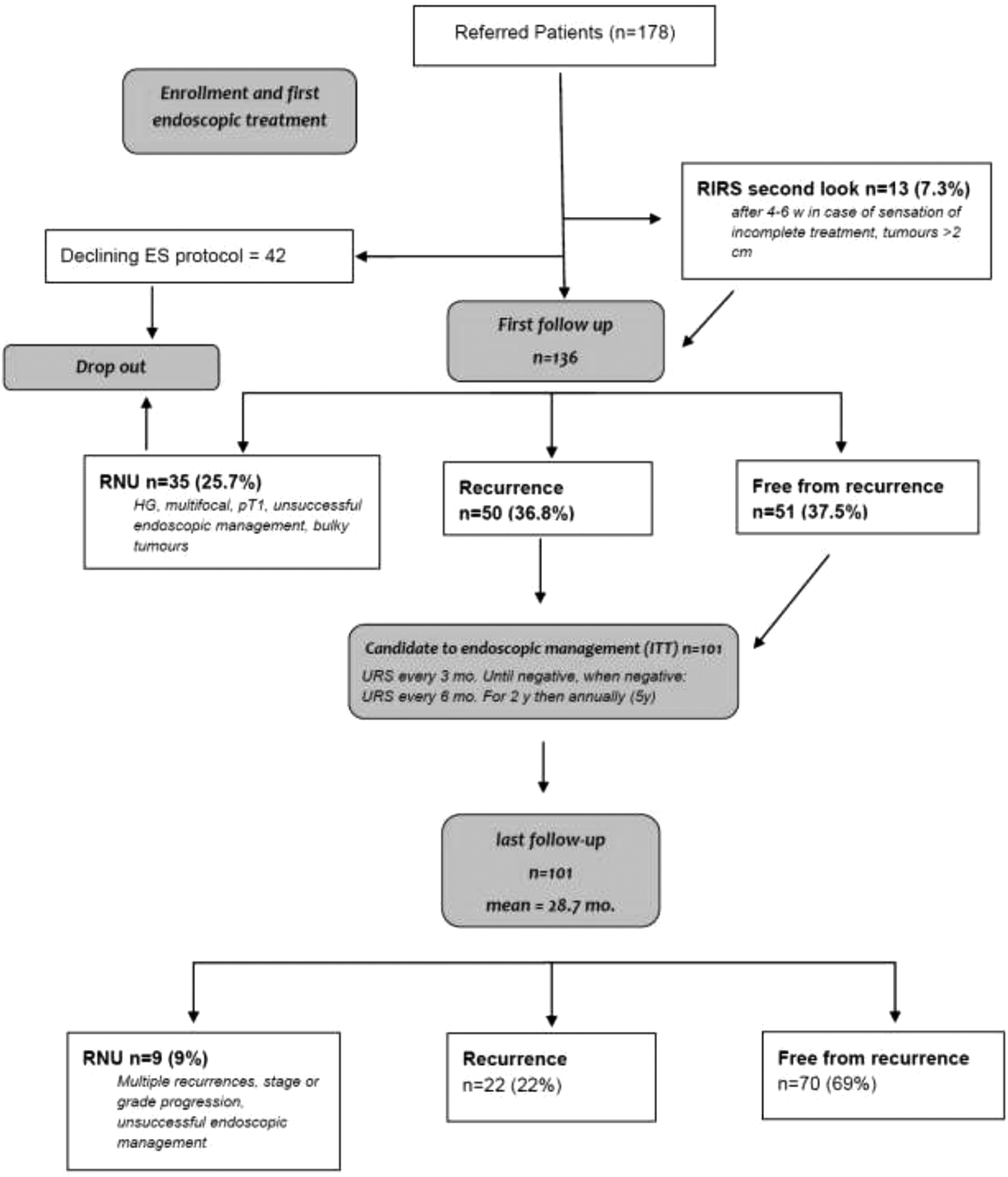
Consort diagram of the entire cohort. ES = endosurveillance; ITT = intention-to-treat; RIRS = retrograde intrarenal surgery; RNU = radical nephroureterectomy; URS = ureterorenoscopy.
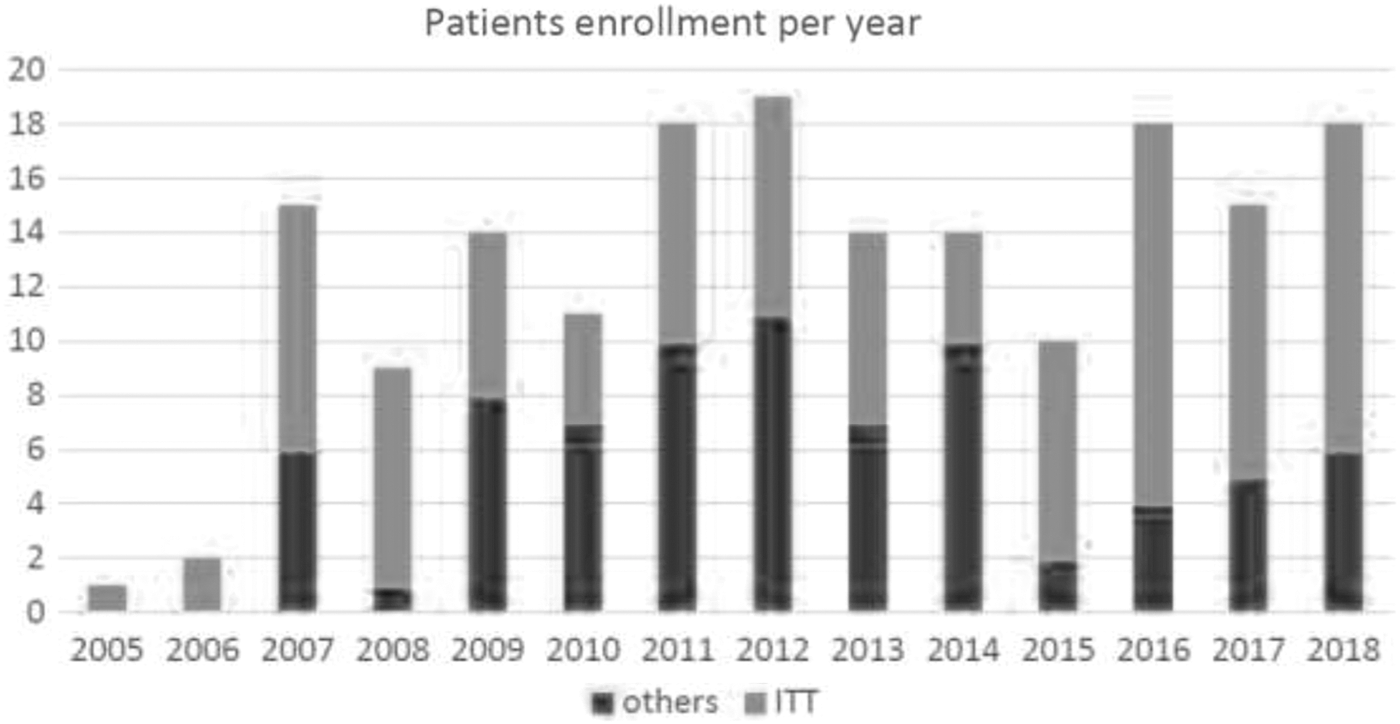
Number of patients starting the treatment each year.
Among the ITT population, there were 32 patients (31.7%) wherein endoscopic treatment was imperative because of “solitary” kidney or poor global renal function 2 kidneys (24 patients), and bilateral UTUC in 8 patients (16 renal units).
At last FU, 70/101 patients (69.3%) were recurrence free, 22 (21.7%) continued conservative treatment for low-risk recurrences, and a further 9 (8.9%) had undergone RNU for progression to higher risk parameters defined in the EAU guidelines 1 during lifelong ES: 5 in imperative cases (persistent high-risk from diagnosis) and 4 for risk progression in nonimperative patients. Patients' demographic and tumor characteristics are summarized in Tables 1 and 2, divided by subgroups.
Patient Demographic Characteristics
ITT = intention-to-treat; SD = standard deviation.
Tumor(s) Characteristics
There were no major intra- or postoperative complications, with 90.4% discharged on the first postoperative day. Only Clavien–Dindo grade I complications (10% self-limiting hematuria) were reported. 11
Kidney-preserving rate (KPR) in ITT-ES 101 patient population was 91% and in the imperative indication patients (total renal units 40), KPR was 87.5%. Imperative patients were older and had more EAU guidelines 3 high-risk features as given in Table 3.
Comparison Within Imperative vs Nonimperative: Intention-to-Treat
IQR = interquartile range.
Kaplan–Maier (K-M) curves for time to first recurrence for imperative and nonimperative patients were plotted and were statistically significantly different for longer recurrence-free survival in nonimperative patients (33.17 months vs 26.87 months—log rank test p = 0.038—Fig. 3).

Kaplan–Mayer curves for time to first recurrence comparing between imperative ITT and nonimperative ITT. Log rank test 0.038 (p < 0.05).
Progression (stage or grade) occurred in 16 patients overall, of whom 8 of 69 (11.5%) were nonimperative (4 treated with RNU), and 9 of 32 (28.1%) were imperative (5 treated with RNU). Patients who refused RNU continued treatment with palliative RIRS. K-M curves for time to progression for imperative and nonimperative patients were not statistically significantly different.
Discussion
Published dual wavelength combination TL–HL:YAG laser technology experience in RC-RIRS management of appropriately selected UTUC patients is extremely limited. A previous expert rating collaborative study group comparing RIRS-eTLA with RIRS-eHLA 6 reported better subjective median parameter performance scores in fiber-tip stability, precision, reduced bleeding, and mucosal perforation. The current literature lacks data of >5 years FU, concerning the oncologic safety of RC-RIRS UTUC-eTLA:HLA dual treatment. The study with the largest cohort remains our last report in 2011. 6 Endoscopic laser coagulative properties are key when dealing with urothelial neoplasia characterized by frequently found papillary morphology core angioneogenesis. 12 The continuous TL mode delivers focused energy precisely into smaller cavitation microbubbles at the fiber tip, reducing collateral energy spread in contrast to HL pulsed disruptive larger cavitation microbubbles. 6 Reported benefits 6 may potentially improve ablative efficiency, and coupled with operator expertise may lead to reduced bleeding and shorter operating time, raising the possibility of treating larger superficial lesions more comprehensively than is possible with other isolated laser sources.
Use of TL–HL duo for RIRS UTUC-eLA for appropriately selected candidates is not yet FDA approved from paucity of data, limited patient eligibility, and for manufacturer's financial cost reasons, but interest in other urologists for this indication is finally emerging. 13 –15 For UC, besides the 2011 publication, 6 the first use of TL in bladder cuff excision during RNU comparing with the electrocautery technique was reported in 2014, demonstrating shorter coagulation time and resection in the TL group, with no significant differences in the incidence of bladder or retroperitoneal UC recurrence. 16 Although Emiliani et al. in an editorial comment in 2015 disagreed with the safety of UTUC-eTLA, 17 it is being progressively used by more institutions as demonstrated by recent publications from Europe and Asia, which reported its safety and oncologic outcomes noninferiority compared with HL in RIRS UTUC-eLA. 7,8
Musi and coworkers described 42 patients treated with UTUC-eTLA, reporting only 2.5% of CD grade III postoperative complications, 20% recurrence, and median estimated recurrence-free survival of 44 months, concluding that TL laser conservative UTUC management was safe and efficacious. Others have also reported optimal vaporization and hemostatic control in the absence of major complications. 7 A Chinese group described 32 patients treated with UTUC-eTLA compared with 107 patients undergoing RNU, demonstrating that the TL group was associated with a reduced loss of renal function, a shorter hospitalization, but a higher tumor recurrence rate. They concluded that ureteroscopic TL therapy could be acceptable for selected UTUC cases. Lifetime surveillance was necessary, 8 which is well recognized already because of the polychronotropic nature of the underlying disease process. A case report in 2018, of two consecutive session UTUC-eTLA treatments of a bulky renal pelvic tumor without recurrence after 3 months, concluded that eTLA may facilitate RIRS by providing clear visibility (little bleeding), enabling complete tumor resection and minimal intraoperative complication risk. 18,19
According to data presented in this 13-year long retrospective analysis, based on the ITT population who accepted the ES protocol requirements, duo eTLA:HLA RC-RIRS represents a valid alternative to eHLA:NdYAG in the future, especially if additional studies were to corroborate our findings. The main difference between TL and HL modes is the continuous TL mode of smaller cavitation microbubbles, rather than the pulsed HL mode with larger cavitation microbubbles. The reduced ensuing penetrative effect makes TL better suited to coagulation of vascular exophytic tumor tissue growing on the thin upper urinary tract collecting system wall. 20 Together, these characteristics under low pressure irrigation conditions improve endovisibility through photothermal coagulation, provide better fiber tip stability, and less penetrative energy capability, all culminating in greater precision during treatment, and ultimately reducing the incidence of inadvertent muscularis perforation when judiciously applied with an expert-based skill set. 6
The main disadvantage of eTLA alone in ablating UTUC is laser fiber tip coating with adherent coagulated necrotic tissue when used in contact mode for larger vascular lesions with deeper vasculature. The solution was to use the dual block laser (Revolix-Duo®), shifting readily from TL after initial tumor blanching to HL mode to cut and disperse necrotic tissue piecemeal to get better access to the tumor base with a clean fiber tip, which could then be definitively ablated with the TL mode. Using the described combined technique of UTUC-eLA (TL and HL), our long-term data indicate that it represents a valid tool in RC-RIRS of selected UTUC patients, leading to high KPRs (91%) in committed compliant ES patients. Moreover, in treatment of patients unfit for RNU (i.e., imperative cases), use of eTLA:HLA combination facilitates endoscopic treatment of higher volume tumors, allowing safe delay to RNU, preserving renal function, and preventing patients from suffering associated morbidity and mortality of dialysis, thereby leading to significant health care cost savings. 21 In the imperative patient group, a higher recurrence and progression rate (28.1%) was observed, at least partly because of more high-grade cancers for which conservative treatment was advocated because of greater competing risk of dialysis-related morbidity and mortality, whereas the influence of worse renal function on recurrence may also play a role as yet undefined. Patients meeting endoscopic management selection criteria (ITT—nonimperative population) had lower progression rate (11%). When progression occurred, RNU was promptly suggested and performed.
In our study, the high early rate (42/178) of patients “lost to FU” after referral was because of those who sought another opinion or alternative treatment elsewhere, or did not want to commit to the lengthy and rigorous FU that was required for the renal preservation strategy as recommended. Their outcomes, good or bad, will remain unknown. The KPR was stated for those accepting the renal preservation treatment recommendation from the outset and adhering to the recommended FU regimen, which was a real-world experience.
Our mean FU (28.7 months) for a 13-year experience study might seem short. Slow growth in referral pattern to the center over time would account for some of this and it may also be partially explained by elderly patients dying of other causes rather than dying from disease and, therefore, dropping out of endoscopic FU. Unfortunately complete data on cancer-specific mortality and global mortality were not available for a variety of systemic reasons, including referral to medical oncology off-site for adjuvant therapy after RNU, return to local hospital FU after RNU, and switchover from paper-based to electronic patient medical record systems during the 13-year study period because of change of ownership and hospital management resulting in lost or unavailable complete medical records, and inability because of legal restrictions to trace causes of death retrospectively in the Italian health care system.
The low complication rate observed (10%—Clavien–Dindo I) of RC-RIRS is possible because of the minimal invasiveness of endoscopic procedure and the skills of the endoscopic surgeons involved.
Conclusions
RC-RIRS UTUC-eLA with TL:HL-YAG duo laser was safe and oncologically effective over 13 years with good renal preservation in 9 out of 10 patients, and seemingly noninferior to alternative combination laser energy technologies used for this indication. Recurrence and progression were not directly related in this predominantly low-risk study population.
Footnotes
Acknowledgment
We appreciate the hard work of our colleagues who assisted in extracting and collecting the relative patient data.
Author Disclosure Statement
L.D., M.A., M.D.D, G.F., and A.P. declare that no competing financial interests exist.
Funding Information
No funding was received for this article.