
Abstract
Aims:
To compare early postoperative morbidity and mortality rates in obese patients (body mass index ≥30 kg/m2) who underwent minimally invasive partial nephrectomy (MIPN) vs open partial nephrectomy (OPN), utilizing the National Surgical Quality Improvement Program (NSQIP) database.
Materials and Methods:
The NSQIP database was queried to identify obese patients who underwent either MIPN or OPN between 2008 and 2016. Patient demographics, comorbidities, operative time (OT), length of stay (LOS), and 30-day postoperative complications, readmissions, and mortality rates were recorded and compared between the two groups. Multivariable logistic regression analysis was used to determine the adjusted odds of early postoperative complications in MIPN vs OPN.
Results:
A total of 6041 obese MIPN patients and 3064 obese OPN patients were identified. Mean OT (minutes ± standard deviation) was longer for MIPN vs OPN (197.2 ± 71.0 vs 189.6 ± 82.4, p < 0.001), while mean LOS (3.8 ± 2.8 days vs 5.8 ± 3.5 days, p < 0.001) and 30-day complications (8.5% vs 19.8%, p < 0.001) were lower. No difference in 30-day postoperative mortality rates between MIPN (0.4%) and OPN (0.5%) was observed (p = 0.426). In the adjusted analysis, the odds of any complication within 30 days in the MIPN group were 61% lower, blood transfusion 73% lower, pneumonia 38% lower, sepsis 70% lower, acute renal failure 64% lower, superficial surgical site infection 40% lower, and reoperation 47% lower, compared with OPN patients.
Conclusions:
When compared with OPN in obese patients, the likelihood of 30-day postoperative morbidity was significantly lower in MIPN patients. However, the odds of 30-day mortality rates were similar between the groups.
Introduction
The incidence of renal-cell carcinoma (RCC) has increased since the 1980s to 2013 from 8.2 to 12 per 100,000 per year, respectively. This is largely attributed to the higher rate of incidental detection of small renal masses because of the increase in utilization of abdominal imaging within the last three decades. 1
In the United States, a proportion of the increased incidence of RCC can be attributed to obesity as 42% of these diagnoses could be casually linked to obesity. 2 Furthermore, each unit increase in body mass index (BMI) leads to a 1.07 increase in the relative risk of developing RCC. 3 In 2015 to 2016, the prevalence of obesity in the United States was 39.8% in adults and 18.5% in youth, and since 1999 to 2000, this represents an increase in prevalence of obesity by 9.8% in adults and 4.6% in children. 2 Consequently, the increased prevalence of obesity in the United States translates into a larger percentage of the population being exposed to one of the major risk factors for RCC.
Most of the RCCs that are found incidentally are smaller (average 5.7 cm vs 8.7 cm) and more often treated with partial nephrectomy (PN) than symptomatically discovered RCCs (15.2% vs 1.2%). 4 PN can be performed either with open or with minimally invasive surgery, which includes the laparoscopic PN (LPN) or robotic PN (RPN) approach. When comparing oncological outcomes for minimally invasive PN (MIPN) vs open PN (OPN), they were found to be equivalent (p = 0.47) with 97.5% and 97.3% cancer-free survival at 7 years, respectively. 5 The current American Urological Association (AUA) guidelines recommend PN for clinical T1a RCC. However, these guidelines do not provide urologists concrete tools for determining when to perform OPN or MIPN. 6
Advances have been made in the surgical evaluation of patients for PN (e.g., RENAL nephrometry score) that can be used to guide surgical management. 7 This tool gives the urologist a standardized language to compare his/her surgical management decision based on objective renal mass characteristics. However, it does not account for patient body habitus, leaving the urologist to his/her own clinical judgment when deciding between OPN and MIPN for an obese patient. Considering the increased prevalence of obesity and the increased risk of RCC within this population, determining the risks and benefits of MIPN vs OPN in an obese patient will be an increasingly more common question posed in urologic practice.
Obesity also poses technical and physiologic challenges that make the postoperative period more complicated. Previous studies have compared outcomes of LPN vs OPN. 8,9 However, robot-assisted surgeries now account for over 50% of the renal cancer surgeries being performed. 10 In this study, we aimed to compare perioperative morbidity and mortality rates in obese patients who underwent MIPN (laparoscopic and robotic) vs OPN.
Materials and Methods
Data source
We used data from 2008 to 2016 of the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP). More than 500 hospital institutions contribute to ACS-NSQIP, which is adjusted for risk differences and has been extensively used in quality improvement of surgical procedures across the United States. The information available in NSQIP data includes deidentified patient demographics, preexisting chronic medical conditions, and information about 30-day postoperative mortality rates, morbidity, readmission, and reoperation (
Study population
Adult (≥18 years) obese patients (BMI ≥30 kg/m2) who received PN either as OPN (current procedural terminology [CPT]: 50240) or MIPN (CPT: 50543) were identified. Patients with CPT codes for both procedures (OPN and MIPN) as well as those with missing BMI were excluded (Fig. 1). An institutional review board exemption was acquired since we analyzed an ethically preapproved and deidentified dataset.
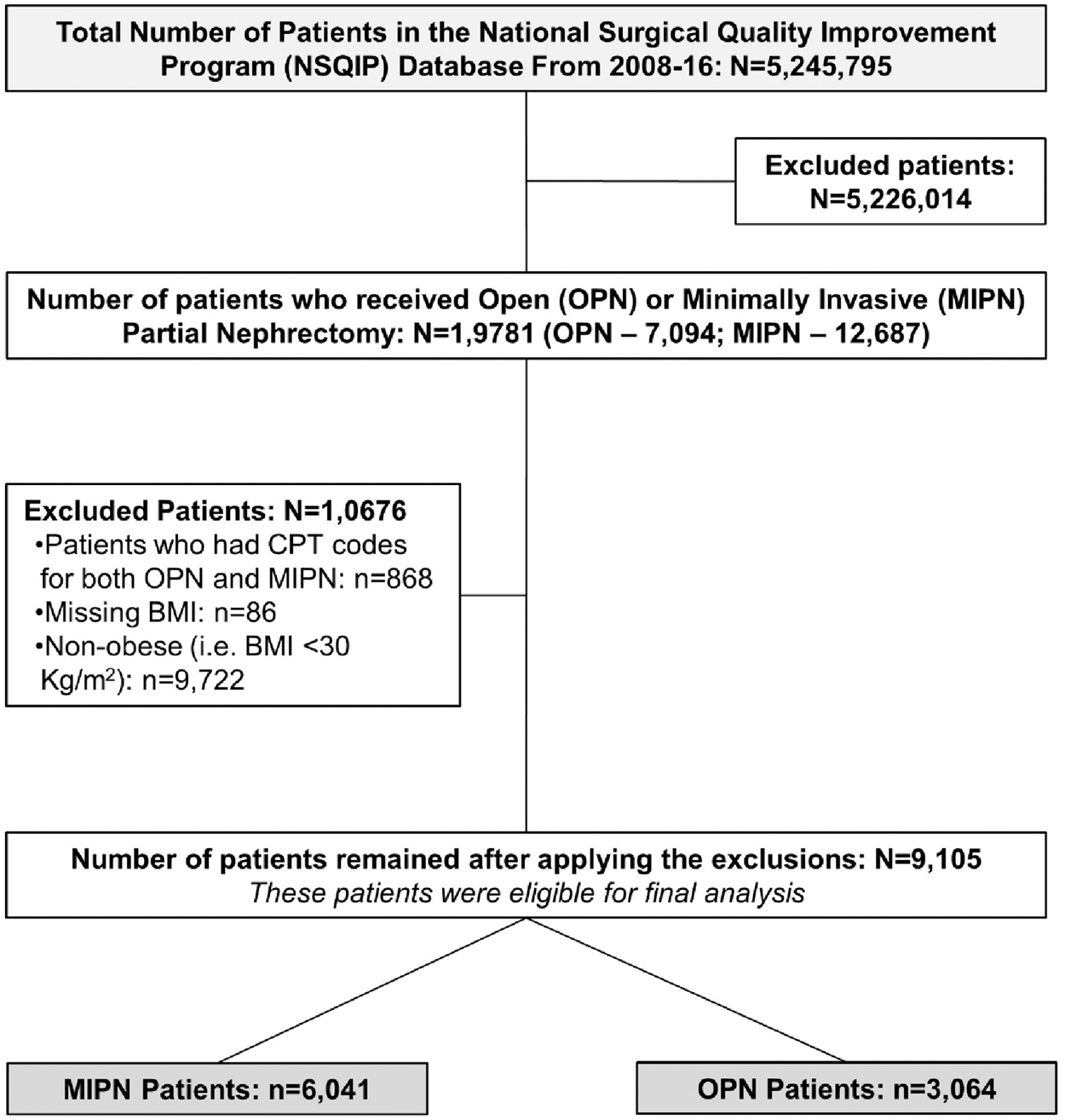
Study flowchart.
Study measures
Patients' demographics and clinical characteristics were used as covariates for the multivariable analyses (Table 1). Mortality and morbidity rates occurring within 30 days of receiving PN were studied. An indicator for any complication within 30 days was created if at least one of the complications was reported. Similarly, an indicator for any wound occurrence was created if at least one of the following was reported: superficial/deep surgical site infection (SSI) or wound disruption.
Demographics and Preoperative Characteristics of Minimally Invasive vs Open Partial Nephrectomy Groups
Other than kidney cancer.
ASA = American Society of Anesthesiologists; COPD = chronic obstructive airway disease; m = missing; MIPN = minimally invasive partial nephrectomy; OPN = open partial nephrectomy; PRBCs = Packed Red Blood Cells; SD = standard deviation.
Statistical analyses
Patient characteristics were described and compared across both groups. Categorical variables are reported as frequency and percentage, while continuous variables are reported as means and standard deviations. Chi-square and Student's t tests were conducted to test for differences in characteristics between the two groups. Each outcome was modeled using a separate logistic regression model to determine the odds of outcomes in MIPN vs OPN. The model was adjusted for patient demographics (age, gender, race, current smoking status, and functional status), American Society of Anesthesiologists (ASA) class, comorbid conditions, and admission year. For each outcome, adjusted odds ratios (ORs) with 95% confidence intervals (95% CIs) were estimated and reported. All the analyses were conducted using SAS®, v9.4 (SAS Institute, Inc., Cary, NC).
Results
Patient demographics
A total of 9105 obese patients who received PN were included, of whom 6041 (66%) received MIPN and 3064 (34%) received OPN. The mean age of the entire cohort was 57.9 ± 11.7 years and the mean BMI was 36.1 ± 5.8 kg/m2. Majority of the study population were males (57.4%) and white (75.9%). The most common comorbid conditions were hypertension (68%) and diabetes (27.3%). Compared with the OPN group, patients in the MIPN group were more likely to be females (43.6% vs 40.8%, p = 0.013), white (76.5% vs 74.9%, p = 0.004), had their MIPN in or after the year 2013 (80.2% vs 67.6%, p = 0.001), and had lower ASA class III (59.3% vs 63.4%) and less likely to have preoperative diabetes, chronic obstructive airway disease, or renal insufficiency/dialysis (p < 0.05) (Table 1).
Unadjusted perioperative and 30-day postoperative outcomes
Length of stay and operating time
MIPN patients had a lower average length of stay (LOS) (3.8 ± 2.8 vs 5.8 ± 3.5, p < 0.001) and a longer average operating time (OPTIME) (197.2 ± 71.0 vs 189.6 ± 82.4, p < 0.001) compared with OPN patients (Table 2).
Length of Stay, Operating Time, 30-Day Mortality Rates, and 30-Day Postoperative Complications in Obese Kidney Cancer Patients Who Received MIPN vs OPN
Any wound occurrence is defined as the presence of either superficial/deep SSI or wound disruption.
CPR = cardiopulmonary resuscitation; CVA = cerebrovascular accident; DVT = deep venous thrombosis; SSI = surgical site infection.
Morbidity
We observed any postoperative complications in 12.3% of patients and any wound occurrence in 2.2% of patients of the entire study cohort. The proportion of patients with any postoperative complications was significantly lower among the MIPN group compared with those in the OPN group (8.5% vs 19.8%, p < 0.001, respectively). Specifically, unadjusted differences were observed in the following postoperative complications across both groups, with all of them being significantly lower in MIPN patients: any wound occurrence, bleeding requiring transfusion, urinary tract infections (UTIs), pneumonia, superficial/deep/organ space SSI, sepsis/septic shock, acute renal failure, and deep venous thrombosis (DVT) (Table 2).
Mortality rates
Overall, we observed postoperative mortality rates in 0.4% (n = 35) of patients. The incidence was 0.4% (n = 21) and 0.5% (n = 14) in MIPN and OPN groups, respectively (Table 2). The average time (mean ± standard deviation [SD]) from surgery to death in the MIPN and OPN groups was 9.0 ± 8.6 and 10.4 ± 8.3 days, respectively.
Readmission
The data on readmission were missing for 7% (n = 635) of the entire study cohort. Among patients with available data, the readmission rate was significantly lower in the MIPN group (5%) when compared with the OPN group (8%, p < 0.001). The mean duration (days ± SD) to readmission from receipt of surgery in MIPN vs OPN was 12.5 ± 7.5 vs 14.4 ± 7.4, respectively. The most prevalent cause of readmissions was hematuria (14.1%) in the MIPN group and hemorrhage/hematoma (10.2%) in the OPN group (Table 3).
Readmission and Reoperation Characteristics
PN = partial nephrectomy.
Reoperation
Similarly, the reoperation rate was significantly lower in the MIPN group (1.8%) than the OPN group (3.5%, p < 0.001). The mean duration (days ± SD) to reoperation from receipt of surgery in MIPN vs OPN was 10.1 ± 8.4 vs 11.6 ± 8.5, respectively. The most common procedure in both groups was cystourethroscopy with insertion of an indwelling ureteral stent (32.1%). Moreover, this intervention was recorded more in the OPN group than the MIPN group (39% vs 25.9%, respectively) (Table 3).
Adjusted odds of 30-day postoperative complications
Mortality rates
After adjusting for confounders, we did not observe any difference in the likelihood of postoperative mortality rates between the two groups (OR [95%CI]: 0.81 [0.41–1.61]) (Fig. 2).
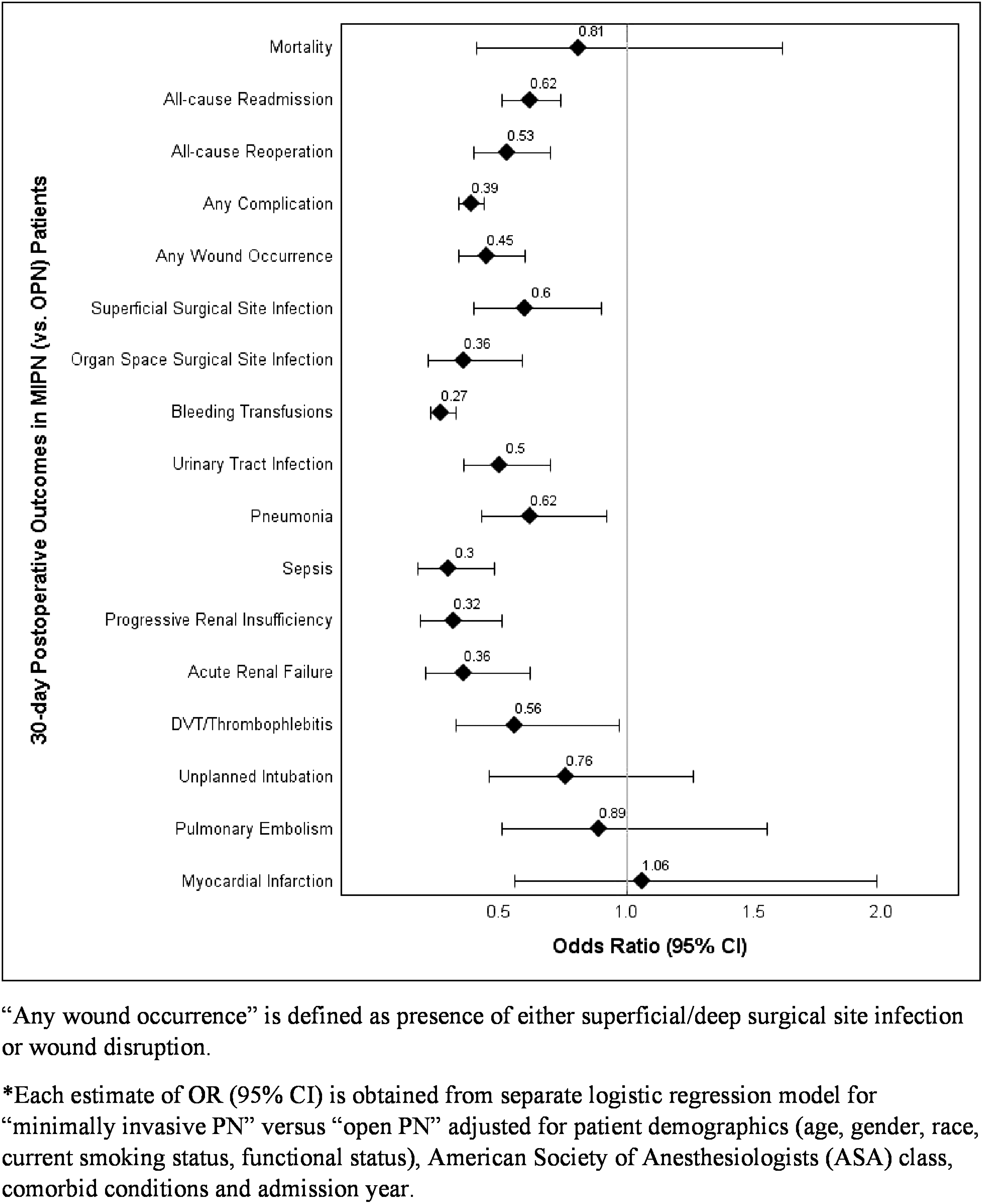
Adjusted odds ratios* (95% CI) indicating the association between postoperative mortality and morbidity rates in obese kidney cancer patients who received MIPN vs OPN. CI = confidence interval; MIPN = minimally invasive partial nephrectomy; OPN = open partial nephrectomy.
Morbidity
The likelihood of developing any complications and any wound occurrence was 61% and 55%, respectively, lower in the MIPN group compared with OPN. The likelihood of developing the following complications was lower in MIPN patients compared with OPN patients: 73% lower risk of bleeding requiring blood transfusion, 50% lower UTI, 38% lower pneumonia, 40% lower superficial SSI, 70% lower sepsis, 68% lower progressive renal insufficiency, 64% lower organ space SSI, 64% lower acute renal failure, and 44% lower DVT (Fig. 2).
Readmission and reoperation risk
The likelihood of postoperative readmission and reoperation was also 38% and 47%, respectively, lower in the MIPN group compared with OPN (Fig. 2).
Discussion
In this study, we utilized the validated NSQIP dataset to compare perioperative mortality and morbidity rates in obese patients who underwent MIPN with those who underwent OPN over the course of 8 years. We observed no difference in 30-day mortality rates in MIPN when compared with OPN. However, we found that obese patients who underwent MIPN had a shorter LOS, longer OPTIME, and lower risk of 30-day postoperative complications, readmissions, and reoperation when compared with OPN. MIPN, after adjusting for confounders, resulted in significant decrease in almost all categories of complications that were measured. The 30-day postoperative complications that were not significantly different between the groups were unplanned intubations, pulmonary embolism, and myocardial infarction.
Data comparing perioperative outcomes for MIPN and OPN have become more widely available as utilization of MIPN has increased. One reason for the increased utilization of MIPN is the rapid adoption of RPN. 10 However, the RENAL nephrometry score of renal masses still provides an objective standardized tool for deciding the best approach for PN patients. In the Canter and colleagues study, results showed that among patients who received PN (n = 407), the OPN group had more complex lesions (mean nephrometry score = 8.19) when compared with those who underwent MIPN (mean score = 6.62, p < 0.0001). 7
There are several multi-institutional studies comparing perioperative outcomes for MIPN and OPN in the nonobese patient population. One study conducted by Pereira and colleagues using the NSQIP database concluded that MIPN was independently associated with reduced rates of 30-day complications, perioperative blood transfusion, prolonged LOS, hospital readmission, and reoperation, compared with OPN. 11 Other large contemporary studies have also supported a reduction in perioperative complications, LOS, and readmission rates in patients who underwent MIPN compared with OPN. 12 –16 The results of the present study among the obese patient population are also consistent with what has been found in other studies among patients with normal BMI.
Obesity adds to the complexity of minimally invasive surgery. This is likely due to the increased adipose tissue that can limit mobility of instruments and increased perinephric fat thickness, which requires more extensive dissection and was associated with increased blood loss and OPTIME during RPN. 17 Additionally, in a multivariate analysis of 81 patients with RCC, increasing visceral fat was associated with worsening Fuhrman grade (p = 0.017). 18 In a retrospective study by Eaton and colleagues on 126 patients who underwent LPN, authors observed no significant differences in regard to OPTIME, transfusion rate, or complications between obese and nonobese patients. 19
Another study examined the effect of BMI on perioperative outcomes among patients undergoing RPN and determined that increased BMI was an independent risk factor for several poor outcomes such as increased LOS, increased blood loss, and increased OPTIME. 20 Similarly, in another single-institution study, obese patients who underwent RPN had a higher blood loss and a trend toward greater OPTIME and warm ischemia time, which did not achieve statistical significance. However, the postoperative complication rate in obese patients was not statistically significant when compared with nonobese patients (8.3% vs 4.3%, p = 0.377). 21
Recently, a multi-institutional analysis of 1770 patients who underwent RPN has concluded that obesity did not correlate with an increased complication rate (p > 0.05). Interestingly, authors concluded that obese patients were more likely to have malignant (>77% vs 68%, p < 0.001) and larger tumors (3.0 cm vs 2.8 cm; p = 0.061) in comparison with the nonobese population. 22 These findings were in accordance with results by Sperling and colleagues who used the NSQIP database and concluded that BMI does not independently predict the likelihood of overall complications or readmission within 30 days and should not be considered a major barrier for MIPN or radical nephrectomy; in this study, there was no open surgery group as in our study. 23
Romero and colleagues compared the perioperative outcomes of OPN and LPN in obese and nonobese patients. Results showed that obese patients undergoing OPN had longer OPTIME and clamp time, higher blood loss, intraoperative complications, and postoperative complications, and longer LOS than those undergoing LPN. 24 A study conducted by Malkoc and colleagues compared 237 obese patients who underwent PN, of whom 25% underwent OPN and 75% underwent RPN. Based on their multivariable analysis, they concluded that OPN independently predicted longer OPTIME, longer LOS, and higher overall complications. However, they did not observe a significant difference in major complications. 25
In our study, we also observed that OPN was associated with longer LOS and overall more complications. However, we found that MIPN was associated with a statically longer OPTIME, although the difference in the mean OPTIME between the two groups was under 10 minutes (OPN: 197.2 ± 71.0 vs RPN: 189.6 ± 82.4, p < 0.001). The learning curve of surgeons performing the robotic surgery, which may vary when comparing a single-institution experience with a national dataset, may play a role in the reported OPTIME.
A multi-institutional study by Abdullah and colleagues found that among obese patients who underwent RPN, longer OPTIME was predicted by the ASA score, tumor size, and nephrometry score. 26 Another study by Web and colleagues compared outcomes for 66 obese patients who were divided into three groups based on procedure type: laparoscopic (n = 31), open (n = 21), or robotic (n = 14). They concluded that on multivariate analysis, both LPN and RPN were associated with significantly less blood loss than OPN and there was no significant difference in LOS between the three modalities. 27 Similarly, our study demonstrated that the likelihood of blood loss was lower in the MIPN group. However, we found LOS to be significantly shorter in the MIPN group compared with OPN.
In our study, we observed that bleeding requiring transfusion (5.8%) was the most commonly recorded postoperative complication in both groups. This is an obvious advantage of MIPN over OPN. A recent meta-analysis showed detrimental oncological outcomes of perioperative blood transfusion following renal surgery for kidney cancer. 28
Cystourethroscopy with insertion of ureteral stent (32.1%) was the most common procedure performed in patients who required reoperation in both groups. While the specific complication of urine leak is not reported in the NSQIP dataset, insertion of ureteral stent is a common procedure for management of persistent urinary leak following PN. These findings are in line with a multi-institutional study that surveyed 2932 consecutive cases of RPN and LPN performed in five high-volume centers. The average BMI in both cohorts was 30. The authors observed bleeding requiring embolization and urinary leak requiring a stent to be the most commonly encountered complications. 29
We acknowledge the limitations of our study being retrospective and nonrandomized. In addition, due to unavailability of information about patient's tumor characteristics (e.g., nephrometry score), we were unable to account for them in our study. However, the NSQIP database is the largest dataset reporting on perioperative outcomes in North America. It is regularly used to report and compare perioperative outcomes among surgical procedures and different subsets of patients with excellent inter-rater variability. 30
Conclusions
In this study, early postoperative morbidity, blood loss, and LOS were significantly lower in the obese patients who received MIPN vs OPN, while the operative time was slightly longer in the MIPN group. No difference in early postoperative mortality rates was noticed between the two approaches. Our results add to the growing knowledge on the advantages of MIPN in the obese patient population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.