
Abstract
Objectives:
To assess the effect of irrigation settings and the size of ureteral access sheath (UAS) on the maximal intra-pelvic pressure (IPPmax) during ureteroscopy (URS) in pigs.
Materials and Methods:
In supine position, three anesthetized female pigs underwent cystoscopy to insert a 6F ureteral catheter in each ureter. Pigs were then turned to prone position to establish a percutaneous access, insert a 10F nephrostomy tube in the kidney, and connect it to a urodynamic device. An 8F semi-rigid ureteroscope or the Flex-X2 Flexible Ureteroscope was used with two irrigation settings: gravity flow and manual pumping using a commercial pump. URS was performed without UAS and with the UAS 9.5/11, 12/14, 14/16 at the ureteropelvic junction and the IPPmax was recorded.
Results:
Under gravity irrigation, the recorded IPPmax during semi-rigid URS in the distal ureter and the renal pelvis was 0 and 30 cmH2O, respectively. Further, the IPPmax during flexible URS in the renal pelvis without UAS, with UAS 9.5/11.5, with UAS 12/14, and with UAS 14/16 was 23, 6, 2, and 1 cmH2O, respectively. Under manual pumping, the IPPmax during semi-rigid URS in the distal ureter and the renal pelvis was 84 and 105 cmH2O, respectively. Further, the IPPmax during flexible URS in the renal pelvis without UAS, with UAS 9.5/11.5, with UAS 12/14, and with UAS 14/16 was 45, 46, 18, and 1 cmH2O, respectively.
Conclusion:
Manual pumping can significantly increase the IPPmax to unsafe levels during URS. The UAS can significantly decrease the IPPmax, even under manual pumping. The larger the UAS, the lower the IPPmax. The use of UAS can render URS safer by acting as a safeguard against the consequences of increased IPP, even under forced irrigation.
Introduction
The latest international guidelines on urolithiasis advocated endoscopic approaches for management of ureteral and renal calculi. 1,2 Retrograde intra-renal surgery (RIRS) was recommended as the first-choice intervention for management of proximal ureteral and renal stones <2 cm because it has a comparable rate of stone-free status and lower complications compared with percutaneous nephrolithotomy. 1 –3 Since the introduction of flexible ureteroscopes into urology practice three decades ago, there have been revolutionary advancements in the diameter and deflection of scopes, types and power settings of laser devices, and design and diameter of laser fibers, ureteral access sheathes (UASs), basket tools, and irrigation devices to simplify the technique and improve the outcomes. 3 However, there are concerns about the changes in the intra-pelvic pressure (IPP) that might reach critical levels, resulting in pyelovenous, pyelolymphatic, and pyelointerstitial backflow with subsequent systemic inflammatory response syndrome and sepsis. 4 The main target for this study was to assess the effect of irrigation settings and the size of UAS on the maximal intra-pelvic pressure (IPPmax) during in vivo URS in a live anesthetized pig. Our hypothesis was that the larger the diameter of the UAS, the lower the IPPmax even under forced irrigation.
Materials and Methods
Study design and experimental setting
After ethics approval was obtained from the respective Veterinary State Services, an experimental setting was designed for measuring the IPPmax while performing URS by using a semi-rigid and flexible ureteroscope with different sizes of UAS and different irrigation settings in three domestic female pigs.
Preparation of the pigs for the experiment
Food was withheld for 12 hours before the experiment. Each pig was brought to the operating table and placed in prone position; an intravenous line was secured in one of the ear veins, and Ketamine, Xylazine, and Atropine Sulfate were injected for initiation of anesthesia. After this, an intubation tube was inserted and connected to the ventilator. Maintenance of anesthesia was achieved by using intravenous propofol 5% throughout the procedure.
Operating room setup and technique
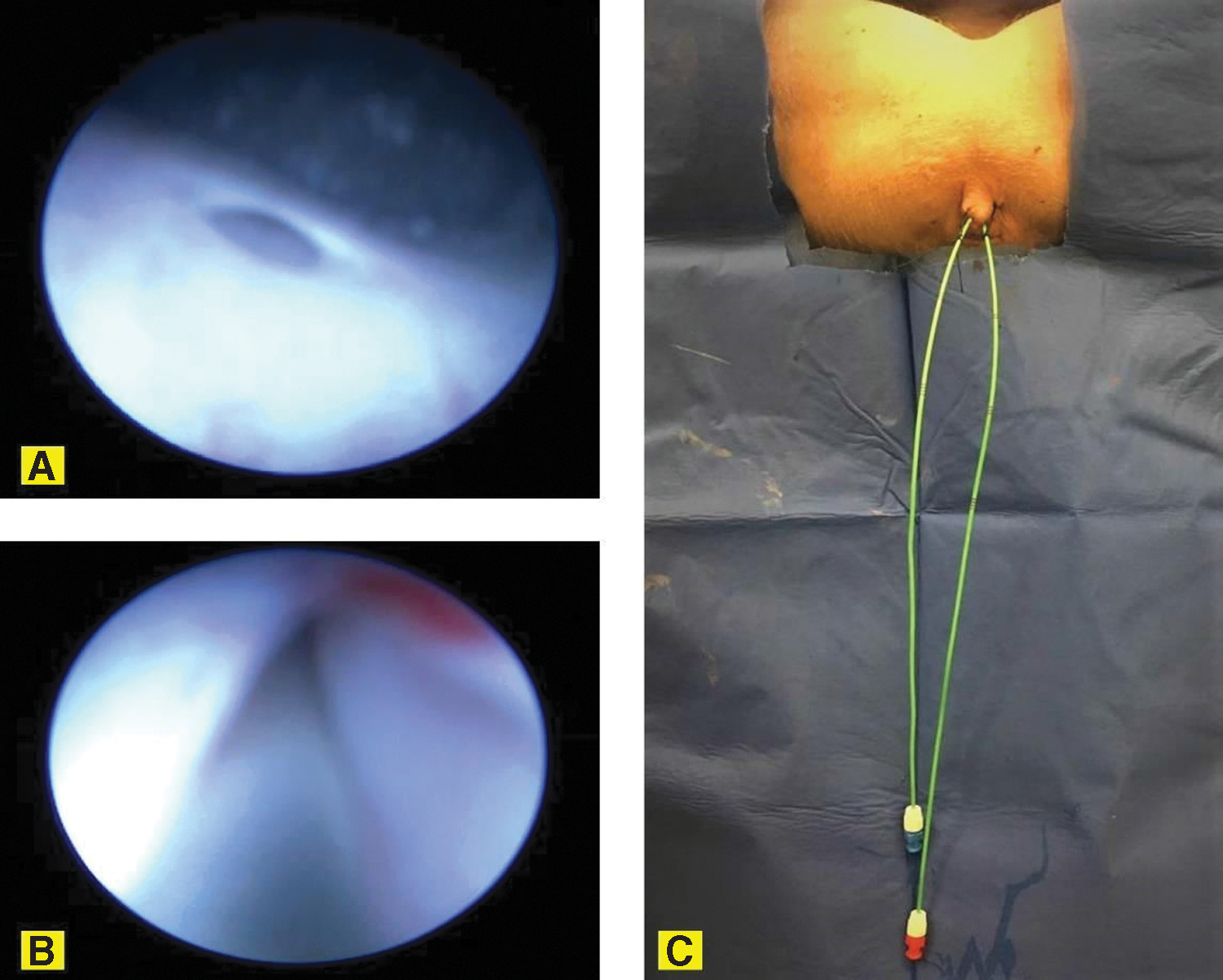
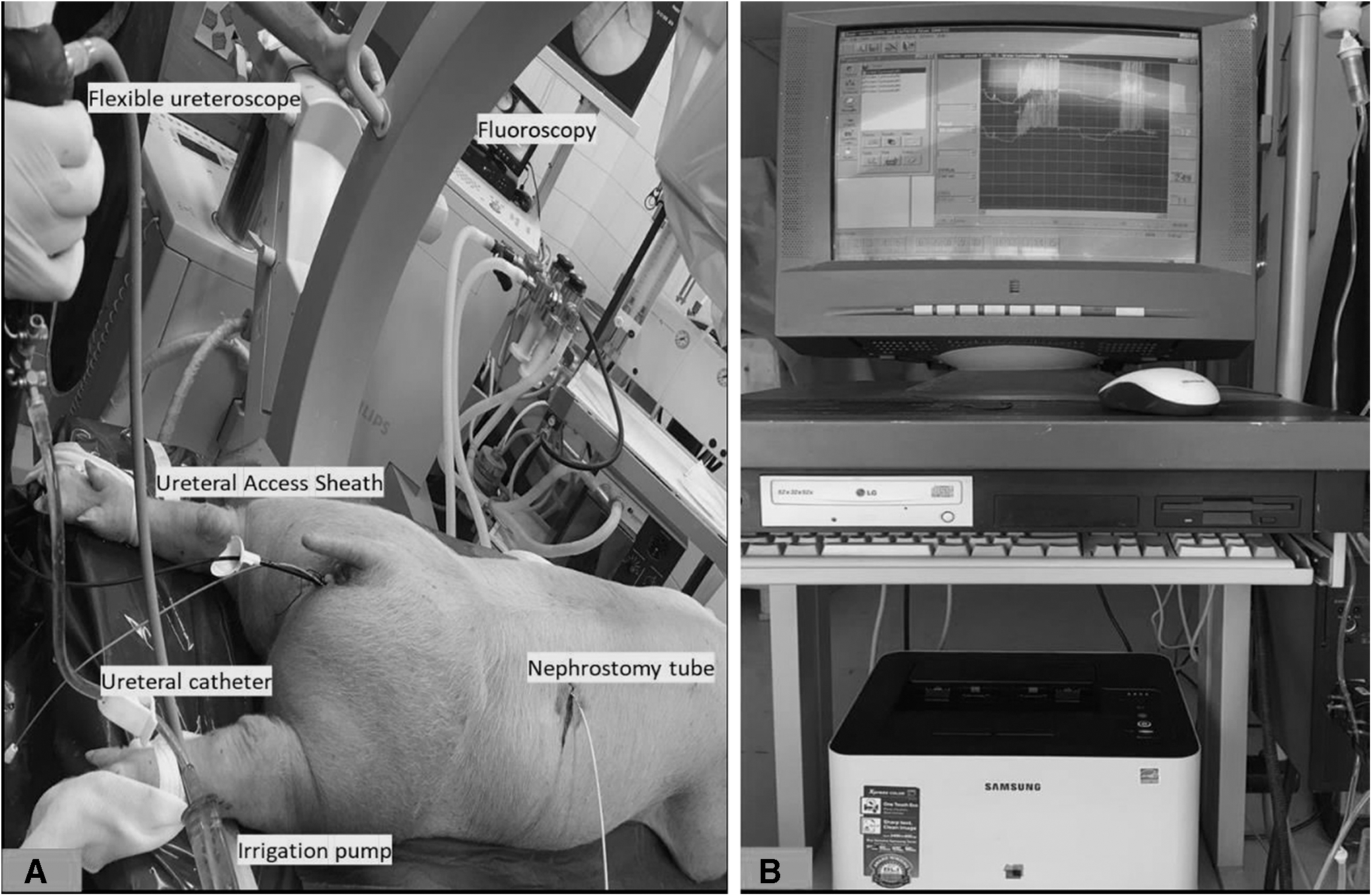
The pig was then put in supine position and tied to the operating table. Cystoscopy was then performed to identify the ureteral orifice (Fig. 1A), advance a 0.035″ hydrophilic guidewire (HiWire™ Nitinol Core Wire Guide, COOK Medical; Cook Ireland Ltd., Limerick, Ireland) up to the kidney (Fig. 1B), and insert a 6F open-end ureteral catheter (COOK Medical; Cook Ireland Ltd.) over the guidewire, leaving the tip of the ureteral catheter in the upper calix or the renal pelvis. In case ureteral tortuosity was encountered, which is frequent in pigs, a hydrophilic guidewire was advanced up the kidney and an angiographic catheter (Glidecath™; Terumo Europe N.V., Leuven, Belgium) was advanced over it to follow the ureteral tortuosity; then, the hydrophilic guidewire was withdrawn and replaced by a super stiff guidewire to straighten the ureter; and finally, the 6F open-end ureteral catheter was inserted and a contrast was injected to delineate the pelvi-caliceal system (PCS). A blue and a red marker was connected to the ureteral catheters to identify the right and the left kidney, respectively, and both were fixed to the external surface of the genitalia by using a 2/0 silk suture to prevent slippage (Fig. 1C). The pig was then turned to the prone position to establish a percutaneous access under fluoroscopy and insert a 10F nephrostomy tube to be connected to the Urodynamic device for real-time measurement of IPP (Fig. 2A). First, to delineate the PCS, a contrast dye was injected in the ureteral catheter. Employing the bull's eye technique, an 18G needle was used to puncture the PCS and a 0.035″ hydrophilic guidewire was inserted. An 8F dilator from an Amplatz percutaneous access tract dilation kit (COOK Medical; Cook Ireland Ltd.) was inserted over the guidewire into the collecting system, and the hydrophilic guidewire was replaced by a 0.035in super stiff guidewire (Amplatz Super Stiff™; Boston Scientific, Heredia, Costa Rica). Sequential dilatation was then performed, and a 10F nephrostomy tube was advanced in the renal pelvis and tied to the external surface of the skin by a 2/0 silk suture.
Measurement of IPP
The distal end of the nephrostomy tube was connected to (P-ves) side of a Medtronic Dantec Duet Multi-P Urodynamic device (Medtronic Functional Diagnostics A/S, Denmark), calibration was done, and the pressure was balanced to the zero state before starting to measure the IPP while the scope was inside the ureter or the PCS (Fig. 2B). The irrigation (Ureteroscopy Irrigation System, COOK Medical; Cook Ireland Ltd.) was connected to the 8F semi-rigid ureteroscope (Karl Storz GmbH & Co. KG, Tuttlingen, Germany) or the Flex-X2 Flexible Ureteroscope (Karl Storz). Two settings of irrigation were used: continuous flow with the level of the 3 L bag 1 m above the pig (gravity irrigation) and manual pumping. The IPPmax was recorded while performing semi-rigid URS in the distal ureter and the renal pelvis and while performing flexible URS in the renal pelvis without UAS and with the UAS 9.5/11, 12/14, 14/16 (Flexor® Ureteral Access Sheath with AQ® Hydrophilic Coating, COOK Medical; Cook Ireland Ltd.) just below the ureteropelvic junction.
Results
The median weight of the three pigs was 30 kg. Under normal irrigation while the 3 L bag was at 1 m above the pig's level (gravity irrigation), the recorded IPPmax while performing semi-rigid URS in the distal ureter was 0 cmH2O and while performing semi-rigid URS in the renal pelvis it was 30 cmH2O. Further, the IPPmax while performing flexible ureteroscopy (FURS) in the renal pelvis without UAS was 23 cmH2O, FURS in the renal pelvis with UAS 9.5/11.5 was 6 cmH2O, FURS in the renal pelvis with UAS 12/14 was 2 cmH2O, and FURS in the renal pelvis with UAS 14/16 was 1 cmH2O (Fig. 3). On the other hand, under manual pumping irrigation while the 3 L bag was at 1 m above the pig's level, the recorded IPPmax while performing semi-rigid URS in the distal ureter was 84 cmH2O and semi-rigid URS in the renal pelvis was 105 cmH2O. Further, the IPPmax while performing FURS in the renal pelvis without UAS was 45 cmH2O, FURS in the renal pelvis with UAS 9.5/11.5 was 46 cmH2O, FURS in the renal pelvis with UAS 12/14 was 18 cmH2O, and FURS in the renal pelvis with UAS 14/16 was 1 cmH2O (Fig. 3).
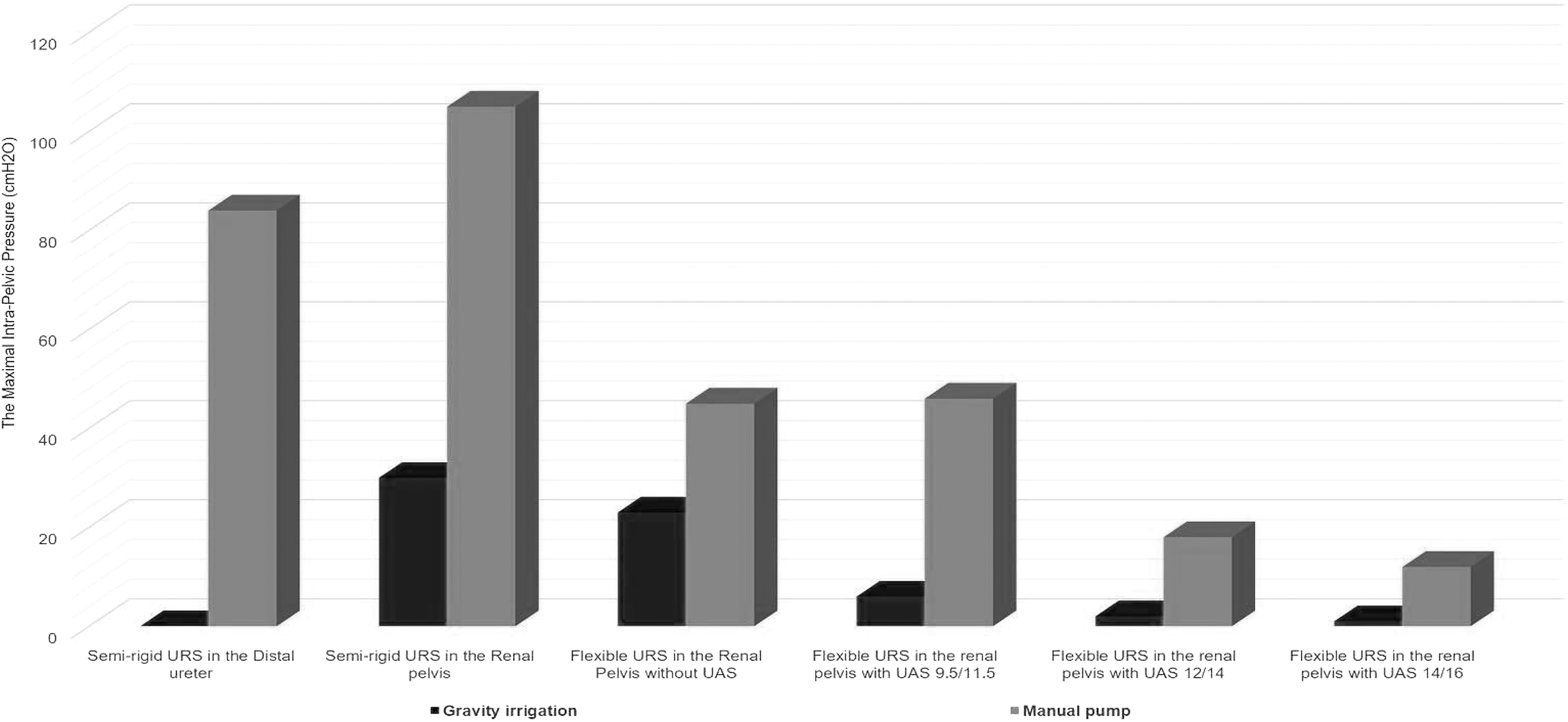
IPPmax during semi-rigid and flexible ureteroscopy in female domestic pigs under different irrigation settings and different ureteral access sheath diameters. IPPmax = maximal intra-pelvic pressure.
Discussion
The use of UAS during RIRS, especially with the introduction of new digital flexible ureteroscopes, offers advantages such as decompression of the PCS, leading to decreased IPP, which might decrease the infectious complications, and potentially facilitating in and out passage of ureteroscopes, resulting in the shortening of operative time. 5 –7 Nevertheless, traumatic and ischemic complications were reported, especially when large-diameter UAS was used. 8,9 This could be overcome by preoperative stenting of the ureter and selecting the appropriate UAS size depending on the state of ureteral lumen. 8
In our study, The IPPmax during semi-rigid URS under gravity irrigation in the distal ureter was zero. We think that this is due to the leakage of irrigation down to the bladder rather than going up to the kidney. However, it was increased to high levels during manual pumping because the diameter of the normal ureter cannot accommodate all irrigation to go down to the bladder; that is why most of the irrigation goes up to the kidney. When the semi-rigid URS advanced in the renal pelvis, the IPPmax was high during gravity irrigation because most of the irrigation goes to the renal pelvis. During pumping, the IPPmax reached critical levels due to the wide channel of the semi-rigid URS, which can allow too much irrigation fluid in the renal pelvis.
During FURS without UAS, the IPPmax was high during gravity irrigation and manual pumping. Nonetheless, it was still lower than the IPPmax during semi-rigid URS in the renal pelvis due to the narrower irrigation channel in the FURS and the smaller diameter of the FURS compared with the semi-rigid URS. However, it was clearly demonstrated that the presence of UAS during FURS decreased the IPPmax and the wider the diameter of the UAS, the lower the IPPmax during FURS.
Previous studies on pigs' kidney have demonstrated acute harmful effects in the form of flattening of the urothelial mucosa, edema of the submucosa, and vacuolization of renal tubules when exposed to high-irrigation pressure >150 mm Hg (≈204 cmH2O). 10 In a cadaveric porcine model, RIRS was performed by using a Flex-X2 flexible ureteroscope and 10/12F and 12/14F Re-Trace™ UAS; the IPP was significantly lower while using the 12/14F UAS, and manual pumping was associated with significantly higher IPP (121 cmH2O with 10/12F UAS and 29 cmH2O with 12/14F UAS). 11 These results were higher than our findings where the IPPmax was 18 cmH2O and 46 cmH2O, respectively. This might be due to the changes that occur in the ureter of pigs after death, which might result in loss of elasticity, leading to higher IPP values.
In an ex vivo study on human cadavers, Rehman and colleagues performed a similar study to ours where RIRS was performed by using a 7.5F flexible ureteroscope without UAS and with 10/12F, 12/14F, and 14/16F UAS and the IPP was recorded while the ureteroscope was in the distal ureter, middle ureter, and renal pelvis under irrigation pressure of 50, 100, and 200 cmH2O, respectively. Interestingly, the IPP did not exceed 30 cmH2O under all sizes of UAS and the IPP was almost similar between the 12/14F and the 14/16F UAS. 12 These results were congruent with the results in our study where the IPPmax was almost similar between the 12/14F and the 14/16F UAS and it did not exceed 46 cmH2O even under manual pumping using the 9.5/11 UAS. Also, another study in an ex vivo anatomical model highlighted the importance of using a large-diameter UAS. 13 The compatibility between the ureteroscopes and UASs was emphasized in a study by Dr. Traxer's group where they assessed IPP by using an artificial ex vivo kidney bench model using eight types of FURS and five types of UAS. 14 In a recent interesting study by Fang and colleagues using fresh porcine cadaver, the ratio of the inner diameter of UAS to the outer diameter of FURS was found to be a more important predictor of IPP rather than the diameter of the FURS, the size and the length of the UAS. 15 A ratio of ≤75% was accompanied with a potentially safe IPP during flexible URS. 15 According to our knowledge, this study was the first to assess the IPPmax in the live anesthetized pig under different irrigation settings and different UAS diameters. However, it has some limitations such as the small number of pigs. Nevertheless, this number was convenient to perform our experiment and obtain appropriate results. Another limitation is the presence of other studies in the literature that assessed the IPP during URS; however, the IPP was measured under nonideal circumstances in a cadaveric porcine model, 11 ex vivo human cadavers, 12 an ex vivo anatomical model, 13 an artificial ex vivo kidney bench model, 14 or fresh porcine cadaver. 15 Given the fact that the urologic anatomy and physiology of pigs are similar to humans and the IPP is affected by several physiological factors such as pyelovenous, pyelolymphatic, and pyelointerstitial backflow during endourologic procedures, 16 –19 we performed our study in a live anesthetized pig to ensure the normal physiologic conditions and avoid any bias of the results that might have occurred in previous studies. An extra limitation is that we did not obtain samples from the kidney for pathological examination to assess any deleterious effects of increased IPP during URS, but this study was just a proof-of-concept experiment and we plan to obtain samples for pathological examination in future studies. It is worth noting that the findings of this study were accepted for presentation during the upcoming 39th Congress of the Société Internationale d'Urologie in Athens.
Conclusion
Manual pumping can significantly increase the IPPmax to unsafe levels during URS. The UAS can significantly decrease the IPPmax, even under manual pumping. The larger the UAS, the lower the IPPmax. The use of UAS can render URS safer by acting as a safeguard against the consequences of increased IPP, even under forced irrigation.
Footnotes
Acknowledgments
This study was partially funded by a 1-year scholarship from the European Urological Scholarship Program (EUSP) to Dr. Yasser Noureldin.
Author Disclosure Statement
All authors declare no conflict of interest.