
Abstract
Objective:
To compare the clinical efficacy and safety between diode laser (980 nm) enucleation of the prostate (DiLEP) and holmium laser enucleation of the prostate (HoLEP) for treating benign prostatic hyperplasia (BPH).
Patients and Methods:
One hundred twenty-six BPH patients in our hospital from December 2016 to December 2017 were enrolled in this study. They were randomized to the DiLEP group or HoLEP group, which were administrated with DiLEP and HoLEP treatment, respectively. The patient's characteristics, such as age, body mass index, comorbidities, prostate volume, and prostate-specific antigen, were recorded before surgery. The perioperative outcomes and complications were also compared. The maximum flow rate (Qmax), postvoid residual (PVR), international prostate symptom score (IPSS), and quality-of-life (QoL) score were assessed at baseline and 3, 6, and 12 months postoperatively.
Results:
No significant differences were observed for the patient's baseline characteristics between both groups. For the perioperative outcomes, including operative time, resected tissue weight, catheter duration, and hospital stay, no significant difference was found between the two groups. However, the DiLEP group showed less blood loss and decrease in hemoglobin compared with the HoLEP group. The incidence of early or late complications was similar for both groups. The Qmax, PVR, IPSS, and QoL for both groups of patients were dramatically improved after surgery. By comparing the Qmax, PVR, IPSS, and QoL between the two groups, no significant differences were detected in the 3-, 6-, or 12-month follow-up.
Conclusions:
This study demonstrated that both DiLEP and HoLEP are efficient and safe treatments for BPH patients. DiLEP showed less blood loss and decrease in hemoglobin than HoLEP, which indicated that the diode laser (980 nm) generates a better hemostasis effect.
Introduction
Benign prostatic hyperplasia (BPH) is a prostate disease that can lead to varying degrees of bladder outlet obstruction and eventually cause harm to the patients. 1 It is a very common disease among the elderly. According to a previous study, as much as 50% of people who are older than 50 are suffering from this disease and the incidence rate increases with the growth of age. 2 The major symptoms for clinical BPH patients are storage symptoms and voiding symptoms. These lower urinary tract symptoms (LUTS), including frequency, urgency, dysuria, difficulty of urination, urinary retention, and so on, affect the quality of patients' life seriously.
Medication treatment is the first-line therapeutic strategy for BPH patients. However, it usually fails in the end for many patients who require surgical treatments. Over the past decades, transurethral resection of the prostate (TURP) is considered the gold standard treatment for BPH and numbers of clinical evidence have proved its safety and efficacy. 3 However, many severe complications were reported for TURP, such as capsular perforation (0.1%), bleeding requiring blood transfusion (2%), and transurethral resection syndrome (TURS, 0.8%). 4 In recent years, different lasers were widely used for resection, vaporization, and enucleation of the prostate, with convinced clinical safety and efficacy. 5
Holmium laser enucleation of the prostate (HoLEP) is one of the most representative procedures. It was first applied in 1998, combined with mechanical morcellation to treat BPH, and achieved a great clinical outcome. 6 Afterward, a large number of studies have demonstrated its better longtime efficacy and safety, compared with TURP. 4,7 –13 Thus, HoLEP is strongly recommended by 2018 EAU guidelines for the treatment of large-sized BPH.
The diode laser is a relatively new laser for surgical treatment of BPH. It has many wavelengths and the most two common wavelengths are 1470 and 980 nm. 11 Diode laser (980 nm) enucleation of the prostate (DiLEP) is performed by some hospitals in recent years. Xu and colleagues compared DiLEP with plasmakinetic enucleation and resection of the prostate (PKERP) and demonstrated that both methods are effective, but DiLEP provides less risk of hemorrhage because it is absorbed by both water and hemoglobin. 14 Other research also shows a similar conclusion. 15,16 In addition, some studies compared DiLEP with TURP, bipolar endoscopic enucleation of the prostate (BEEP), and thulium laser transurethral enucleation of the prostate (ThuLEP). The results showed that DiLEP provided comparable clinical efficacy, with less blood loss. 17 –19 Based on literature findings, no study was reported to compare the safety and efficacy between DiLEP and HoLEP. In this study, 126 BPH patients were enrolled and randomly divided into two groups, which were administrated with DiLEP and HoLEP, respectively. We compared the clinical safety and efficacy between the groups and aimed at providing the clinical evidence of DiLEP for BPH.
Patients and Methods
Patients
From December 2016 to December 2017, a total of 126 BPH patients in our department were enrolled in this study (Fig. 1). The minimum follow-up was 12 months. All these patients signed a written informed consent before the study. The study protocol was approved by the Ethics Committee of the Second Affiliated Hospital, School of Medicine, Zhejiang University. This randomized controlled trial (RCT) was registered in the Chinese Clinical Trials Register (ChiCTR190002207) and followed by Consolidated Standards of Reporting Trials (CONSORT) guidelines. The diagnosis of BPH was based on history, physical examination, prostate-specific antigen (PSA), urinalysis, urodynamic studies, and transrectal ultrasound (TRUS). If the PSA was abnormal or clinically suspicious tumors, a biopsy guided by TRUS was done. The BPH patients who required surgical treatment were qualified for this study. The additional inclusion criteria included: (1) maximum flow rate (Qmax) ≤15 mL/s, (2) quality of life (QoL) score ≥3, and (3) international prostate symptom score (IPSS) ≥8; exclusion criteria included: (1) confirmed prostate cancer or history of prostate surgery, (2) acute prostatitis or urethritis, and (3) neurogenic bladder and urethral injury. One hundred twenty-six BPH patients were randomized to the DiLEP group or HoLEP group with allocation ratio 1:1, and they were administrated with DiLEP and HoLEP, respectively. The computer-generated allocation sequence was used for randomization of the patients.
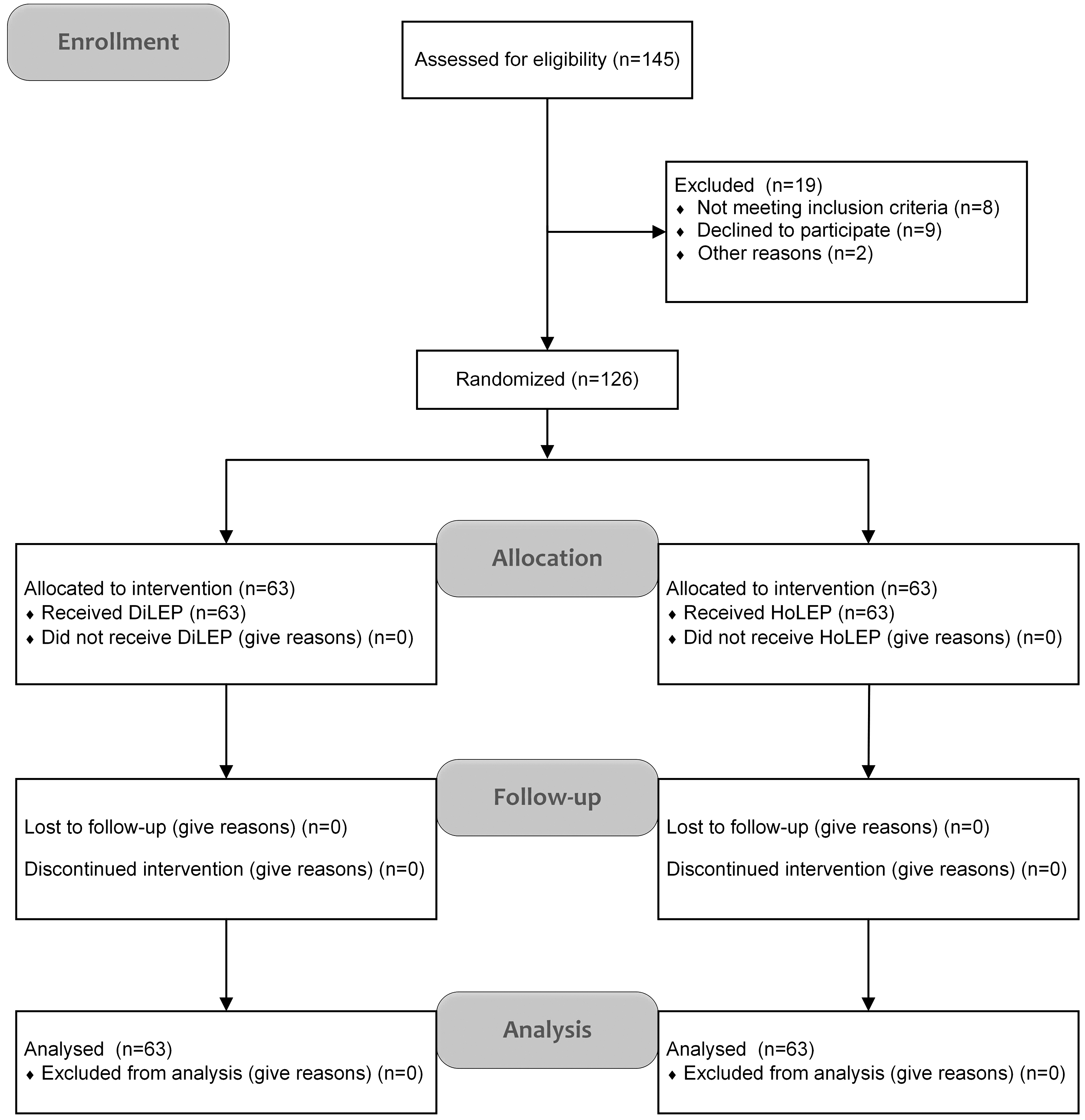
CONSORT 2010 flow diagram: A total of 145 patients were recruited at the beginning of this study. Finally, 126 BPH patients were enrolled in this study and were randomized to the DiLEP group or HoLEP group, which were administrated with DiLEP and HoLEP, respectively. BPH = benign prostatic hyperplasia; CONSORT = Consolidated Standards of Reporting Trials; DiLEP = diode laser (980 nm) enucleation of the prostate; HoLEP = holmium laser enucleation of the prostate.
Methods
The prostate volume (PV) was calculated by height × length × width × π/6 through TRUS, and the body mass index (BMI) was counted by weight/height 2 (kg/m2). Apart from PV and BMI, the patient's age, PSA, comorbidities, Qmax, postvoid residual (PVR), IPSS, and QoL were also recorded before operations. The decrease in hemoglobin and serum sodium was measured by comparing preoperation (1–3 days) with the condition immediately after surgery. As for the blood loss during operation, we measured it by the turbidimetry method (blood loss = the number of flushing fluid × preoperative mean corpuscular hemoglobin concentration [MCHC] of flushing fluid/postoperative MCHC of flushing fluid). Other perioperative outcomes, such as operative time, enucleation time, morcellation time, resected tissue weight, bladder irrigation time, catheter duration, and hospital stay, were also collected. After surgery, Qmax, PVR, IPSS, and QoL were assessed at 3, 6, and 12 months in the follow-up. In addition, PV and PSA were measured at the third month after operation. Perioperative complications between the two groups were recorded at the same time, respectively.
Operative procedure
All operations for both groups of patients were finished by the same surgeon, who was experienced in both DiLEP and HoLEP. The surgery was performed under general or spinal anesthesia in the lithotomy position. The main surgical equipment we used for surgical operation included: (1) A 27F continuous resectoscope and the flushing fluid was normal saline. (2) The diode laser system (Bio Litec, Jena, Germany) emitting light at a wavelength of 980 nm was coupled with a 600-μm fiber. 20 (3) HoLEP was performed by using a high-powered 100-W laser device (Lumenis Medical Systems, Santa Clara, CA) with a 550-μm fiber. (4) The morcellator system (Hawk, Hangzhou, China) was used. If patients have bladder stones, the surgeon will crush the calculus with the laser first. The detailed DiLEP and HoLEP procedures are similar to those previously described. 20,21
Statistical analysis
Results for measurement data are reported as mean ± standard deviation (SD). The continuous variables were assessed by Student's t-test, and the enumeration variables were assessed by chi-squared test. All data were analyzed with the Statistical Package for the Social Sciences version 21.0 (SPSS, Chicago, IL). Figures were made by Microsoft Visio 2013 (Microsoft Corporation, Redmond, WA) and GraphPad Prism 7.0 (GraphPad Software, San Diego, CA). p-Values <0.05 were considered statistically significant.
Results
Table 1 shows the baseline patient characteristics preoperatively. As described, the mean age in the DiLEP group is 71.7 ± 8.7 years, whereas it is 71.6 ± 9.8 years in the HoLEP group (p = 0.954). The mean BMI of both groups is 22.6 ± 2.5 vs 22.2 ± 2.0 (p = 0.371). Besides, the PV for both DiLEP and HoLEP groups is 83.0 ± 34.8 vs 75.6 ± 28.9 (p = 0.193). In addition, the mean PSA level of two groups preoperatively is 2.7 ± 1.2 vs 2.2 ± 1.8 (p = 0.100). No statistical significance was detected between the two groups regarding Qmax, PVR, IPSS, and QoL before the operation.
Baseline Patient Characteristics
Results for continuous variables are reported as mean ± SD. p-Values <0.05 were considered statistically significant.
BMI = body mass index; DiLEP = diode laser (980 nm) enucleation of the prostate; HoLEP = holmium laser enucleation of the prostate; IPSS = international prostate symptom score; PSA = prostate-specific antigen; PVR = postvoid residual; Qmax = maximum flow rate; QoL = quality of life; SD = standard deviation.
The perioperative outcomes are described in Table 2. No significant differences were observed for operative time, enucleation time, morcellation time, resected tissue weight, the percentage of resected tissue, enucleation efficiency, and morcellation efficiency in two groups (all p-values >0.05). However, the blood loss and decrease in hemoglobin level in the DiLEP group were significantly lower compared with the HoLEP group (Fig. 2). Specifically, the mean blood loss in the DiLEP group is 23.3 ± 20.9 mL, whereas it is 36.0 ± 21.4 mL in the HoLEP group (p = 0.001); the mean decrease in hemoglobin of DiLEP group and HoLEP group is 4.0 ± 2.3 g/L vs 5.1 ± 2.2 g/L (p = 0.007), respectively. The bladder irrigation time, catheter duration, and hospital stay in both groups presented no significant differences (p > 0.05). These data suggested that the blood loss of DiLEP surgery was significantly less compared with HoLEP surgery, which indicated that the diode laser (980 nm) generated a better hemostasis effect.
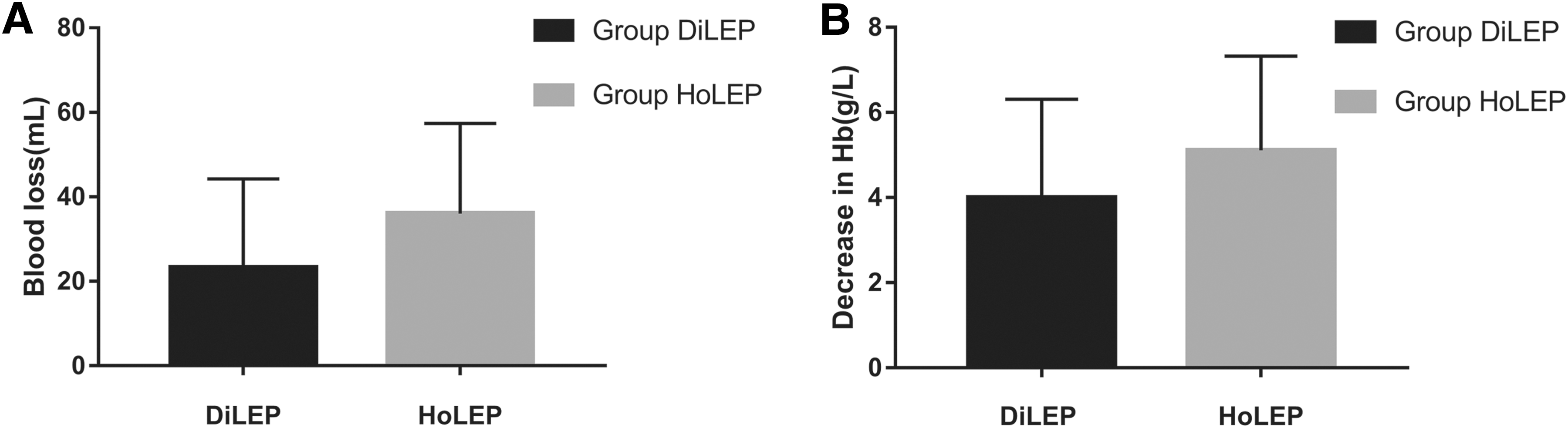
Pre- and postoperative blood loss
Perioperative Outcomes
Data are represented as mean ± SD for each parameter, and p-values <0.05 were considered statistically significant.
Percentage of resected tissue (%): enucleated prostate weight/preoperative prostate weight × 100%.
Enucleation efficiency (g/min): enucleated prostate weight/enucleation time.
Morcellation efficiency (g/min): enucleated prostate weight/morcellation time.
Table 3 shows the functional outcomes at baseline and at 3, 6, and 12 months postoperatively. Compared with preoperative values, the Qmax, PVR, IPSS, and QoL for both groups of patients were dramatically improved in the 3-, 6-, or 12-month follow-up. By comparing the Qmax, PVR, IPSS, and QoL between the two groups, no significant differences were detected in the 3-, 6-, or 12-month follow-up, which indicated that DiLEP and HoLEP generated an equal clinical long-time efficacy for BPH.
Functional Parameters at Baseline and at 3, 6, and 12 Months
Data are represented as mean ± SD for each parameter, with n = 63 and p-values <0.05 were considered statistically significant.
In regard to intraoperative complications, bladder injury, ureteric orifice injury, and capsule perforation were not observed for both groups of patients (Table 4). In addition, TURS was not observed in the DiLEP group or HoLEP group and blood transfusion was not applied for all patients. The overall postoperative complications for both groups were low and the major complications are dysuria, re-catheterization, retrograde ejaculation, temporary urinary incontinence, postoperative bleeding, urethral stricture, and bladder neck contracture. The rate of postoperative complications between the two groups showed no significant difference. The incidences of temporary urinary incontinence for DiLEP group and HoLEP group are 6.3% and 7.9%, respectively. The incidences of bladder neck contracture were 1.6% and 0.0%, respectively. All perioperative complications of patients were improved or cured after treatments, as previously described. 22 In the DiLEP group, one patient was retreated with bladder neck incision 58 days after DiLEP surgery due to bladder neck contracture. However, for the HoLEP group, no patient underwent reoperation during our follow-up. These data suggested that DiLEP and HoLEP generate similar clinical safety.
Perioperative Complications in the DiLEP and HoLEP Groups
TURS = transurethral resection syndrome; UTI = urinary tract infection.
Discussion
BPH is an extremely common disease in aging males around the world. According to a study, as much as 50% prevalence was observed in men who were older than 50 and the incidence increased with the progression of age. 2 LUTS affect these patients' QoL very seriously. As we all know, TURP is regarded as the gold standard treatment for BPH in the past decades. 3 But because of its disadvantages of bleeding and TURS, the surgical risks were significantly increased for old patients with serious internal medicine diseases (such as coronary heart disease, pulmonary insufficiency, etc.). In recent years, different lasers were widely used for resection, vaporization, and enucleation of the prostate, which generated better clinical safety and efficacy.
As an early laser type, Nd-YAG has been replaced by other lasers mentioned earlier because of its low absorption coefficient and tissue penetration depth. 23 At present, HoLEP has been the most widely accepted for the treatment of BPH and recommended as the first-line therapeutic option for large-sized BPH by 2018 EAU guidelines. Its safety and efficacy were demonstrated by a number of high-level clinical studies. 6 –10,12,13,24,25 Moreover, many surgical approaches have been used for BPH, which generated good clinical outcomes, such as ThuLEP, BEEP, and PKERP. 15,16,26,27 Also, the transurethral split of the prostate (TUSP) has been getting increasing attention by urologists in recent years. A study with 565 cases showed that TUSP was a safe and long-term effective treatment for BPH. 28 In conclusion, great progression was made for the treatments for BPH in recent years, and high-level RCTs were required for clarifying their safety and efficacy.
In this study, we designed an RCT to compare the clinical safety and efficacy between DiLEP and HoLEP and aimed at collecting the clinical evidence for DiLEP to treat BPH. The result showed that both DiLEP and HoLEP generated outstanding clinical efficacy and safety, which has also been proved earlier by other studies. 13,15,19,20,24 In this study, DiLEP and HoLEP were finished by one skilled surgeon. The energy of the diode laser (980 nm) we used was 120 W for DiLEP, and the energy of the holmium laser was 80 W for HoLEP. The mean operative time was 62.9 ± 18.2 minutes for the DiLEP group and 68.7 ± 19.7 minutes for the HoLEP group, which was similar to previous studies. 14,16,20
The holmium laser was delivered through 550 nm fibers in short pulses. 23 The wavelength of the holmium laser was about 2140 nm and its penetration depth was 0.5 mm in prostate tissue. 29 However, for diode lasers, the normally used wavelengths include 940, 980, or 1470 nm, and different wavelengths have different penetration depths. 23 In this study, we used the 980-nm diode laser in our department for treating BPH, which is a relatively new wavelength for clinical using. Thus, the clinical evidences for the 980-nm diode laser were relatively lacking. In this study, we designed an RCT to compare the 980-nm diode laser with the holmium laser for enucleation of the prostate. The results showed that no serious complications, including bladder injury, ureteric orifice injury, capsule perforation, and TURS, were observed in all patients, which indicated that both 980-nm diode lasers and holmium lasers were safe for treating BPH. However, the blood loss and decrease in hemoglobin were dramatically lower in the DiLEP group compared with the HoLEP group, which indicated that the 980-nm diode laser generated a better hemostasis effect. This difference was a result from different wavelengths of two lasers: The holmium laser is absorbed by water, and 980-nm diode lasers are absorbed by both water and hemoglobin.
To determine the longtime efficacy of two groups of patients, follow-up was made 3-, 6-, or 12 months after the surgery. Qmax, PVR, IPSS, and QoL were recorded for each patient. The Qmax, PVR, IPSS, and QoL for both groups of patients were dramatically improved in the 3-, 6-, or 12-month follow-up. No significant differences were detected between two groups, which indicated that DiLEP and HoLEP generated equal clinical longtime efficacy for BPH. These data provided strong evidence for DiLEP in the treatment of BPH. However, it requires to be clarified by a larger sample size and multiple center studies in the future.
One of the drawbacks for HoLEP and DiLEP is their long learning curve. Naspro and colleagues reported in 2006 that to train a skilled surgeon, 200 cases were required. 30 In our department, the beginner was trained by a skilled surgeon and usually became more confident with HoLEP after 15 patients.
Although current laser surgeries are safer than TURP with high efficiency, there are still some perioperative complications. The most common postoperative complication is temporary urinary incontinence (stress or urgency). Krambeck and colleagues showed a prevalence of 11% to 12% in 1065 cases for HoLEP surgery. 8 In our study, a total of 9 (7.1%) patients displayed temporary urinary incontinence after the operation in two groups and the incidence of temporary urinary incontinence between two groups was close with no significant difference. For all of the patients, the temporary urinary incontinence disappeared in 3 months after the operation. Bladder neck contracture is a serious postoperative complication of BPH; its incidence in our study is extremely low since we used the lasers for enucleation of the prostate. Besides, 4 (3.2%) retrograde ejaculation cases and 7 (5.6%) urinary tract infection cases were observed in two groups of patients. Taken together, the overall postoperative complication is low for both HoLEP and DiLEP surgery.
In our study, the incidence of retrograde ejaculation was 3.2% for both groups. The operations for both DiLEP and HoLEP groups of patients were finished by the same surgeon. We tried to keep a complete bladder neck during DiLEP and HoLEP surgical procedures to decrease the incidence of retrograde ejaculation. In addition, the sexual activities were absent for many old Chinese patients, which may also lead to the low incidence of retrograde ejaculation.
Although this is a prospective study, there are still some limitations of our work. First, it is a single-center experience. Second, the small sample size is not large. Therefore, a multicenter study with a larger sample is required to verify this result.
Conclusions
In summary, our study demonstrated that both DiLEP and HoLEP are efficient and safe treatments for BPH patients. DiLEP showed less blood loss and a decrease in hemoglobin than HoLEP, which indicated that the diode laser (980 nm) generates a better hemostasis effect.
Footnotes
Acknowledgments
This work was supported by grants from Zhejiang Provincial Natural Science Foundation of China (No. LY18H040007 to J.W.) and the National Natural Science Foundation of China (No. 81871153 to J.W. and 81500532 to B.W.).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.