
Abstract
Introduction:
Robotic-Assisted Radical Prostatectomy (RARP) has largely replaced the open technique worldwide as the first surgical modality for prostate cancer. We aim at describing the experience of RARP at a high-volume single cancer center, proposing a modified technique of nerve-sparing prostatectomy and comparing functional outcomes throughout our experience.
Materials and Methods:
We retrospectively reviewed 1088 patients divided into group 1 (operated from May 2013 to November 2014), submitted to the standard transperitoneal robotic technique, and group 2 (operated from December 2014 to December 2017), submitted to extraperitoneal RARP with complete anterior peri-prostatic preservation technique and a clipless approach (no use of clips and cautious use of bipolar energy). We constructed a retrospective 1:2 matched-pair analysis considering age, body mass index, D'Amico risk classification, and American Society of Anesthesiologists classification as matching criteria. Univariate and multivariate Cox logistic regression analysis were used to identify predictors related to recovery of continence and erectile function.
Results:
Groups were comparable by clinical and demographic variables. There was no significant difference in overall continence rate. Mean time for continence recovery was 6.6 months in group 1 and 5.8 months in group 2. Erectile function recovery, with or without drugs, in 12 months was described in 53.5% in group 1 and 75% in group 2. Potency recovery was significantly earlier in group 2.
Conclusions:
In our experience, extraperitoneal RARP with complete anterior peri-prostatic preservation and a clipless approach is a feasible and reproducible technique. It demonstrated improved erectile function recovery and similar continence results. Prospective multicenter studies are needed to validate these results.
Introduction
Prostate cancer is the most common non-cutaneous cancer affecting men worldwide. Radical retropubic prostatectomy (RRP) has been established as the standard surgical treatment option for localized disease, but the drawback of this procedure is the risk of urinary incontinence and erectile dysfunction.
Since the introduction of robotic-assisted radical prostatectomy (RARP) in 2000, intense discussion has arisen in the urologic-oncology community about safety, as well as the oncological and functional outcomes of RARP. After almost 20 years of robotic surgery, several studies have been published and demonstrated excellent outcomes associated with known advantages of the minimally invasive procedures. Therefore, RARP has largely replaced RRP worldwide as the first surgical modality option for prostate cancer.
In this study, we describe the experience of RARP at a high-volume single cancer center. In addition, we propose a modified technique of nerve-sparing prostatectomy and compare functional outcomes throughout our experience.
Materials and Methods
Study design and data evaluation
After Institutional Review Board approval, we retrospectively reviewed 1088 consecutive men with localized or locally advanced prostate cancer who were submitted to RARP and pelvic lymph node dissection (LND) at A.C. Camargo Cancer Center (Brazil) between May 2013 and December 2017. As a purpose of this study, we stratified patients into two matched-pair groups. For retrospective 1:2 matched-pair analysis, we considered age, D'Amico risk classification, body mass index (BMI), and ASA (American Society of Anesthesiologists) classification as matching criteria. Group 1 comprises 228 patients operated from May 2013 to November 2014, who were submitted to the standard transperitoneal robotic technique described. 1 In group 2, there were 456 patients operated from December 2014 to December 2017 submitted to extraperitoneal RARP with complete anterior peri-prostatic preservation technique and a clipless approach.
We collected data from patient charts and pathological reports containing information about age, ASA classification, BMI, D'Amico risk classification, prostate-specific antigen (PSA) level, prostate volume, biopsy Gleason score, pTNM stage, positive surgical margins (PSM), hospitalization time, and follow-up time. Patients who lost follow-up or with missing data regarding postoperative PSA or functional status were excluded. Metastatic patients (M1) were also excluded. The procedures were performed by 13 genitourinary and minimally invasive surgeons, who were included after completion of their training in a standardized protocol. This technical modification was implemented in our department intending to optimize functional outcomes with a better preservation of prostatic surrounding tissues.
Pathological specimens were handled and evaluated according to the International Society of Urological Pathology (ISUP) consensus by dedicated genitourinary pathologists of our institution. Patients were staged according to the American Joint Committee on Cancer criteria. 2 PSM was defined as a tumor at the inked margin of the resected specimen. We classified it as focal PSM, if unifocal and margin length ≤3 mm. Extensive PSM was defined when multifocal margins were evidenced or a margin length >3 mm. 3,4 Biochemical recurrence (BCR) was defined as a PSA level >0.2 ng/mL on two consecutive measurements. Adjuvant or salvage treatments were indicated according to the discretion of each surgeon.
Potency was defined as the capacity to achieve sexual intercourse with or without phosfodiesterase-type 5 inhibitors (PDE5i). Continence was defined as the use of no pads. Early penile rehabilitation with PDE5i was prescribed after catheter removal, and pelvic floor rehabilitation was performed for patients using more than one pad per day after the first follow-up appointment. Preoperative and postoperative erectile function status were assessed by the surgeon as part of clinical follow-up practice at each one of the appointments. Follow-up generally consisted of office visits and PSA testing at 45 days after surgery, every 3 months for the first 2 years, subsequently every 6 months until 5 years, and yearly thereafter. All surgical and clinical perioperative complications (up to 90 days) were recorded. They were graded according to the modified Clavien classification system. 5
Complete anterior peri-prostatic preservation technique
The patient is positioned supine at 15° to 20° angle, and all the pressure points are padded. We usually perform an extraperitoneal approach with a small infraumbilical incision. Pre-peritoneal blunt dissection is done for placing a Spacemaker trocar (Covidien, Mansfield, MA) to access the Retzius space. Subsequently, we start insufflation and set pneumoperitoneum in 12 to 15 mm/H2O and all other trocars are inserted. In addition to the 8-mm robotic ports, we use 12- and 5-mm assistant ports. We keep at least 8 to 10 cm of distance between ports. We usually perform the procedure with four robotic instruments of da Vinci® Si robot platform (Intuitive Surgical, Sunnyvale, CA): a robotic monopolar scissor (arm No. 1—right robotic port), Maryland bipolar grasper (arm No. 2—medial left robotic port), Prograsp forceps (arm No. 3—far left robotic port), 0° lens in the camera port during the entire procedure, and only one large needle driver for suturing (we use one needle driver in arm No. 1 and keep the Maryland bipolar grasper in arm No. 2, sparing the cost of one instrument).
An incision on the anterior bladder neck is done without opening the endopelvic fascia. Suspension of the Foley catheter is performed to assess the posterior bladder neck until achieving vas deferens and seminal vesicles (Fig. 1A, B; Supplementary Video S1).
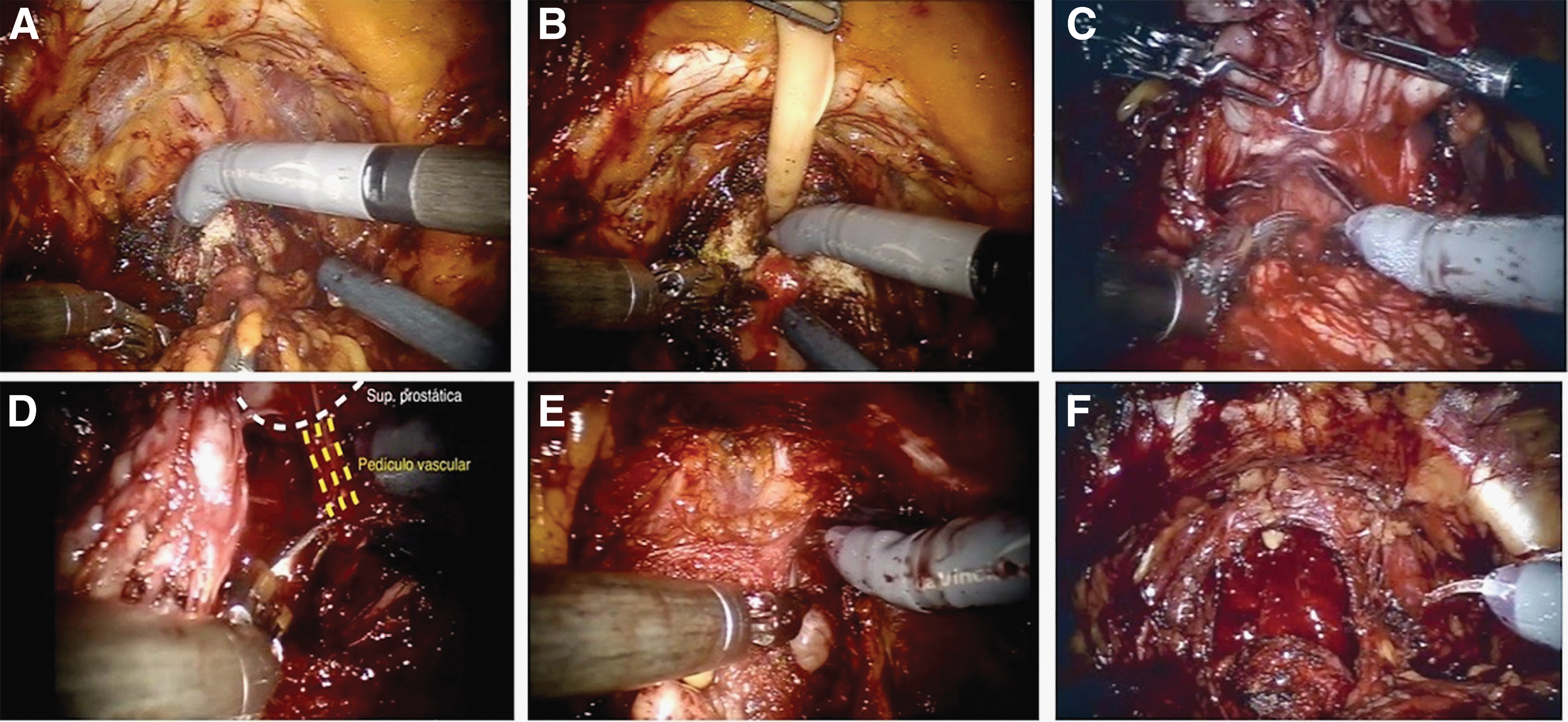
After isolation of the Denonvillier's fascia from the posterior prostatic surface (Fig. 1C), we start the dissection of the neurovascular bundles (NVB) and peri-prostatic tissue, primarily taking care to dissect into the interfascial or even intrafascial plane. If extracapsular extension is presumed or even identified, the dissection is done into the extrafascial plane. The isolation of NVB is bilaterally performed with cautious use of bipolar energy at the beginning of dissection of the vascular pedicles (Fig. 1D) and followed by a retrograde blunt dissection until achieving the posterior apex (Fig. 1E). Appropriate dissection is identified in an avascular plane. We do not advocate the use of metallic or polymer clips, which potentially overwhelm the NVB area and can eventually migrate, causing harm 6 (Fig. 1F).
The dorsal vein complex is isolated from the anterior prostatic surface with no ligature until the dissection of the apex and section of the urethra. A regional or extended LND is performed according to the preoperative risk group and the discretion of each surgeon. The low-risk group underwent no pelvic lymphadenectomy. The discussion to undergo an extended LND has been presented only to the high-risk group. When a PSMA-PET/CT is available, its results can help this decision. An extended LND involves the areas of the obturator fossa, external and internal iliac vessels, and common iliac artery until the ureter crosses. Finally, vesicourethral anastomosis is performed by using a running barbed suture with two units of V-Lock 180 3-0 (Covidien). We usually do not perform the posterior musculofascial reconstructions described by Rocco and colleagues. 7 A 20F Foley catheter is maintained for about 7 to 10 days and a closed suction drain is maintained until a decrease of secreted fluids.
Statistical analysis
Demographic and clinical data were correlated between groups. Mann-Whitney test was applicable in continuous variables and they were presented as median and range, whereas categorical variables were presented as absolute number and percentages. Fisher's exact test or Pearson Chi-squared test were used when appropriate. Kaplan-Meier method using the log-rank test assessed the functional outcomes of continence recovery and potency. Univariate and multivariate Cox regression analysis were used to identify predictors related to recovery of continence and erectile function, using variables with a proportional hazard assumption. Only variables with a p-value <0.2 were included in the multivariate stepwise-backward analysis. Statistical analyses were performed by SPSS v. 21.0 (IBM Corp., Armonk, NY) and R software (
Results
Demographic and clinical data are summarized in Table 1. After matched-pair analysis, all demographic and clinical data were equivalent. Pre-surgical D'Amico classification accounted for about one third of low, intermediate, and high risk in both groups.
Analysis of Demographic, Clinical, and Pathological Data Between Groups from 2013 to 2017
Boldface type indicates p-value considered significant < 0.05.
Robotic-assisted radical prostatectomy performed with the classical technique.
Robotic-assisted radical prostatectomy performed with an extraperitoneal, complete anterior peri-prostatic technique with a clipless approach.
p-Value considered significant <0.05. Non-parametric variables used the Mann-Whitney test and parametric variables used Pearson Chi-Squared test or Fisher's exact test when appropriate.
ASA = American Society of Anesthesiologists; BMI = body mass index; PSA = prostate-specific antigen.
Pathological reports evidenced the majority of localized disease (78.1% in group 1 and 77.2% in group 2). In the first group, 2.2% had evidence of nodal disease and, in the second group, 2.7% were pN1 (p = 0.917).
On performing a pathological analysis of surgical margins, 39 cases (19.6%) of extensive PSM were found in the first group, and 42 cases (9.3%) were found in the second group (p < 0.001). Further, focal PSM was found in 24.1% in the first group, and in 16.6% in the second group. The mean number of lymph nodes dissected was 5 (0–38 nodes). Positive nodes were evidenced in 5 patients in group 1 (2.2%), and in 14 patients in group 2 (3.1%).
Median follow-up time was 33.5 months for patients in group 1 and 12 months for those in group 2. During this period, an increase was demonstrated in locally advanced prostate cancer cases. In 2017, 28.5% were classified as pT3 in the final pathological report, whereas 6.6% represented these cases in 2013.
Surgical complications were also reported in both groups, with no significant difference between them (p = 0.908). The majority of complications in both groups were mild complications (Clavien-Dindo I and II) accounting for 8.8% and 9% in the groups, respectively (Tables 2 and 3). One death was reported in each group related to intraoperative bleeding necessitating reoperation and followed by hemorrhagic complications at the intensive care unit.
Description of Early and Late Complications Reported Throughout the Overall Series
Comparison of Perioperative Complications in Paired Groups According to the Clavien-Dindo Classification System
p-Value considered significant <0.05.
Patients with at least 18 months of follow-up were analyzed about BCR and the need of salvage treatments in the whole series (Table 4). A total of 87 patients (15.1%) had BCR according to a PSA value ≥0.2 ng/dL followed by a confirmatory test. Due to a short follow-up time, particularly in group 2, we were not able to provide comparative oncological outcomes in this study.
Analysis of Oncological Outcomes in Patients with At Least 18 Months of Follow-Up (n = 575)
ADT = androgen deprivation therapy; HIFU = high-intensity focused ultrasound; NED = no evidence of disease.
Functional outcomes were compared between the techniques (Fig. 2). In group 1, time to continence recovery was 42.6%, 55.4%, 76.3%, 87.1%, and 97.2% in 30 days, 3 months, 6 months, 12 months, and longer than 12 months, respectively. In group 2, continence rate was 31.9%, 44.6%, 71.8%, 90.6%, and 98.1% in 30 days, 3 months, 6 months, 12 months, and longer than 12 months, respectively. Mean time for continence recovery was 6.6 months in group 1 and 5.8 months in group 2. Log-rank test was not statistically significant (p = 0.145).
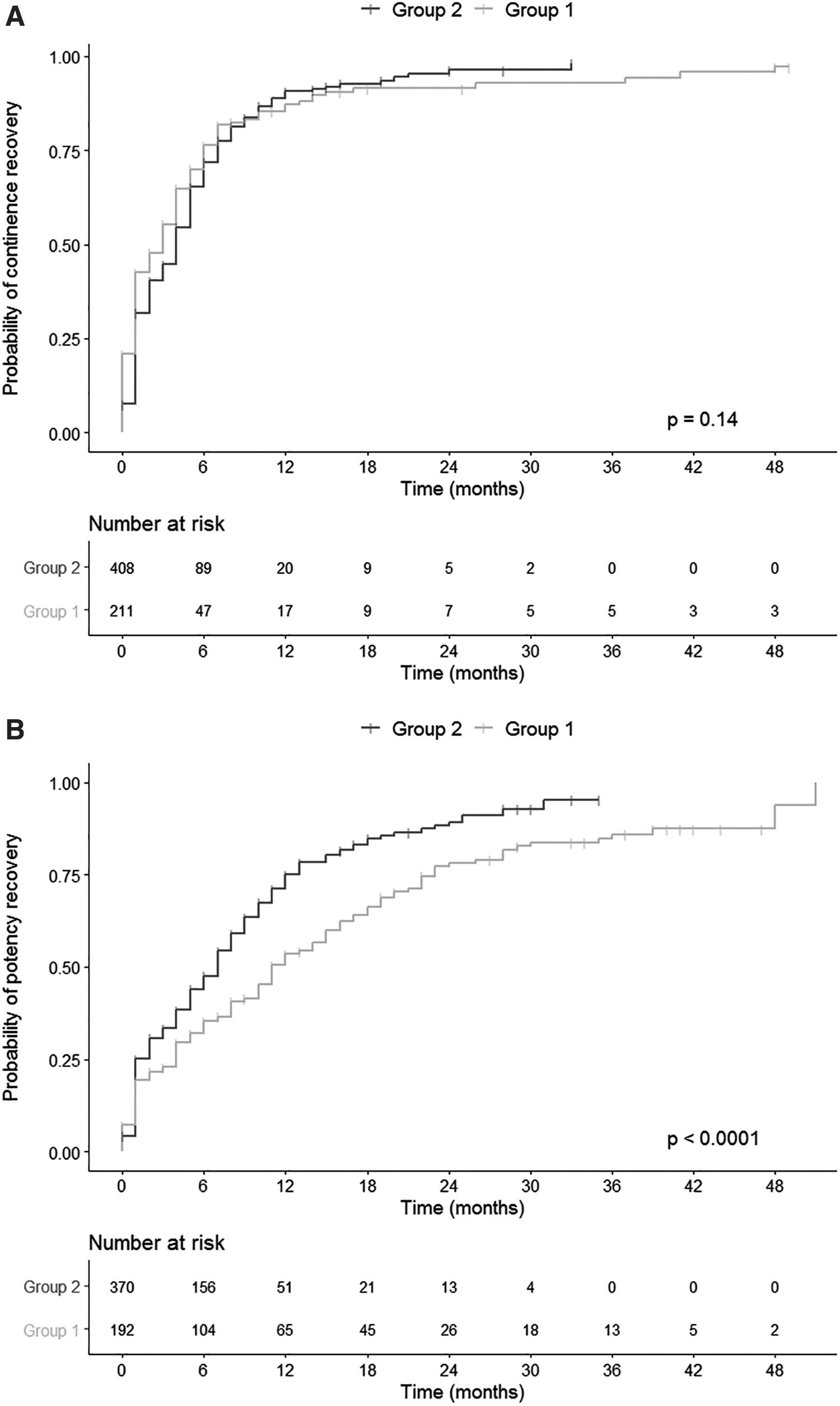
According to potency rates, in 12 months, up to 53.5% of patients in group 1 were potent with or without drugs, whereas up to 75.1% of patients in group 2 were potent with or without drugs. It was found that about 89.2% of patients in group 2, followed up at least for 24 months, were self-declared as potent. Figure 2 shows Kaplan-Meier curves for continence recovery and erectile function recovery. Mean time for recovery of erectile function was 9.4 months in group 2 and 16.3 months in group 1, with significant difference in the log-rank test.
Finally, possible factors contributing to a better continence recovery and erectile function were analyzed by a univariate and a multivariate Cox regression analysis (Tables 5 and 6).
Univariate Analysis of Prognostic Factors for Continence Recovery Considering the Use of No Pads per Day (Pad-Free) and Postoperative Erectile Function With or Without Drugs: Cox Regression Model
Boldface type indicates p-value considered significant < 0.05.
Statistical significance related to p-value <0.05.
Erectile function recovery with or without drugs.
CI = confidence interval; HR = hazard ratio; PSM = positive surgical margin.
Multivariate Analysis of Prognostic Factors for Continence Recovery Considering the Use of No Pads per Day (Pad-Free) and Postoperative Erectile Function Recovery With or Without Drugs: Cox Regression Model
Boldface type indicates p-value considered significant < 0.05.
Statistical significance related to p-value <0.05.
Erectile function recovery with or without drugs.
CI = confidence interval; HR = hazard ratio.
Discussion
Post-prostatectomy oncological and functional outcomes are related to the achievement of the trifecta criteria, which includes undetectable PSA, urinary continence, and erectile function. 8 Intending to optimize these results, the advanced knowledge about the peri-prostatic surrounding tissues is crucial to this purpose. 9,10
The development of robotic surgery has provided a large high-resolution, three-dimensional view and the feasibility of complex movements. A detailed analysis was published by Eichelberg and coworkers. This study revealed that more than 20% of peri-prostatic nerves were situated at the most ventrally surface of the prostate. 11 This area is usually sectioned in the standard open nerve-sparing techniques, previously described by Walsh and colleagues or even in the posteriorly standardized laparoscopic and robotic approaches. 12 –14
A systematic review by Yossepowitch and coworkers synthesized an average PSM rate from 6.5% to 32%. 15 Studies analyzing, independently, focal and extensive PSM rate showed results from around 21% to 27% and from 9% to 17%, respectively. Kwon and coworkers showed that their first 50 cases had a significantly higher rate of PSM than the next ones (38% vs 20%; p = 0.010). 16,17 If the overall PSM rate were considered, our data evidenced a higher incidence. However, considering only the extensive PSM rate, we had correlated results, particularly after the standardization of the proposed technique. Further, the incidence of pT3 stages should be highlighted throughout the series. It could be explained by the fact that we are a reference center in the treatment of complex cases in our country.
Our reported overall complications rates between the groups were not statistically significant (13.12% vs 12.68%). A U.S. published series reported an overall complication rate of 9.7% and an average hospital stay of 1.2 days. Their most common complications were clot and urine retention, necessitating recatheterization. 18 Another study accomplished a systematic review and evidenced a mean complication rate of 9%, ranging from 3% to 26%. In this review, the most common complication was lymphocele/lymphorrea (mean: 3.1%), followed by urine leak (mean: 1.8%). 19 The fact that we usually perform a clipless surgery did not compromise our rate of lymphocele, and we reported only five cases of hematoma into the prostatic surgical bed.
BCR varies from 5% to 15.7% in literature. 20 –22 We demonstrated similar results with 15.1% of BCR and 0.7% of cancer-specific mortality in patients with at least 18 months of follow-up. Reviewing two large series, the 5- and 8-year BCR-free survival was 84.9% and 81%, respectively. Similarly, they described the 8-year metastasis-free survival of 98.5% and the 8-year cancer-specific survival of 99.1%. 21,22 We need a further maturation of our data to conduct a better analysis of our oncological outcomes.
Better functional outcomes are expected with the preservation of the described Aphrodite's veil and the endopelvic fascia. In literature, the comparison between techniques with or without the preservation of the Aphrodite's veil has been published. Kwon and coworkers evidenced a higher significant continence rate at 12 months in patients with preservation of endopelvic fascia. Nonetheless, this significant improvement occurred only when defining continence as a pad-free status (97% vs 88%). 16 Our cohort was not able to demonstrate better continence outcomes in the group with the complete anterior peri-prostatic preservation technique. Similarly, with other studies, age was a significant factor involved in continence recovery, particularly in elderly patients ≥70 years-old. 16,23 Elderly patients ≥70 years-old and recovery of the erectile function were statistically significant factors influencing the multivariate analysis of continence recovery.
RARP has evidenced encouraging outcomes in terms of recovery of erectile function. Studies with similar techniques provided outcomes ranging from 47% to 70% at 3 months to 69% to 90% at 12 months. 1,24,25 Our results are comparable with the literature. Our model was able to predict, in univariate analysis, that elderly, prostate volume >60 cm3, multiple comorbidities in ASA3 population, earlier continence recovery, and the proposed technique are factors that improve potency recovery. In multivariate analysis, only elderly patients ≥60 years-old and proposed technique persisted as independent prognostic factors.
Our institution is a reference cancer center in the country and it has been in the vanguard of many treatment strategies. However, several limitations of the study can be mentioned. The procedures were performed by 13 different surgeons in different stages of their learning curve. Despite this, the procedures rigorously maintained a standardized protocol. First, cases were performed in a more initial stage of surgeons' experience. This could have influenced the outcomes. The study has a retrospective design in a single center and it is important to be validated for prospective multi-institutional studies. Questionnaires were not able to provide an assessment of postoperative outcomes. Positive points were the large number of patients, the standardization of a feasible and reproducible technique, and the comparison between techniques.
Conclusions
RARP has become the preferred technique for surgical treatment of prostate cancer. Several technical modifications have been proposed as a way to improve results. In our experience, extraperitoneal RARP with complete anterior peri-prostatic preservation and a clipless approach is a feasible and replicable technique. It demonstrated improved potency outcomes and similar continence results. Prospective multicenter studies are needed to validate these results.
Footnotes
Acknowledgments
The authors thank all members of the Urology Department at A.C. Camargo Cancer Center. They are particularly grateful for the cooperation and support of their pathologists: Dr. Isabela Werneck da Cunha and Dr. Stephania Martins Bezerra. They also thank Vinicius Calsavara, PhD, for the assistance with statistical analysis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Video S1