
Abstract
Purpose:
To reduce the amount of opioids prescribed at discharge after robotic surgery, we hypothesized that the majority patients do not require opioids for pain control after robotic urologic oncologic procedures.
Materials and Methods:
This prospective study aimed to reduce opioids prescribed at discharge after robot-assisted radical prostatectomy (RARP), robot-assisted radical nephrectomy (RARN), and robot-assisted partial nephrectomy (RAPN). Before 9/2018, 100% of patients were discharged on varying amounts of oxycodone (range: 75–337.5 oral morphine milligram equivalents [MME]). We implemented a standardized nonopioid analgesia pathway with escalation options (Fig. 1). To assess the safety of our approach, we analyzed pain scores, telephone encounters, and emergency department visits in our cohort.
Results:
Our cohort (n = 170) consisted of patients undergoing RARP (n = 87), RARN (n = 25), and RAPN (n = 58) between September 2018 and January 2019. Overall, 67.7% were discharged without opioids, 24.4% with 10 pills of tramadol (50 MME), and 8.2% with 10 pills of oxycodone (75 MME). On multivariable analysis, older age (odds ratio: 0.961, 95% confidence interval: 0.923–0.995, p = 0.026) was associated with lower odds of needing opioids at discharge. There was no difference in pain scores at the postoperative outpatient visit (p = 0.66) or postoperative telephone encounters (p = 0.45) between those discharged with and without opioids.
Conclusion:
The majority of robotic surgery patients do not require opioids upon discharge. Implementation of a simple, standardized nonopioid protocol resulted in a dramatic reduction in the amount of opioids prescribed in our patient population. An escalation protocol allows for a patient-centered approach to reduce narcotic prescribing, although still addressing surgical pain.
Introduction
Opioid addiction has reached critical levels in the United States. An estimated 3.3 million Americans older than 12 years are affected by substance abuse involving a prescription pain medication. 1,2
Surgeons are at the forefront of this problem; of patients obtaining long-term opioid therapy at a pain clinic, nearly one-third report that their initial opioid prescription was from a surgeon. 3 In addition, prescribed opioids are often unused, with many patients using fewer than half the amount prescribed, and as much as 90% of patients having leftover opioids. 4 –7 As a result, there is increasing interest in utilizing non-narcotic approaches to postoperative pain to curb the opioid epidemic.
Excess narcotic pills present significant safety concerns. First, they serve as the primary opioid exposure for otherwise opioid-naive patients. Even small amounts of opioid prescribed by a medical professional carry a risk of persistent use. Even with only a single day's prescription, persistent opioid use at 1 year has been shown to approach 6%. When prescribed a 7-day course, the rate of persistent use increased to 13.5% at 1 year. 8
In addition, excess retained pills after surgery present a danger to the community. Excess narcotics are rarely discarded appropriately and are improperly stored in the vast majority of cases. 7,9,10 In fact, diversion presents a significant source of abuse in people with opioid addiction. The 2017 National Survey on Drug Use and Health revealed that 50% of addicted adults obtained opioids from family/friends at no cost, and an additional 15% were able to purchase excess pills from family/friends. 11
There have been significant surgeon-led efforts to define safe and appropriate opioid prescribing practices. 7,9,12 Recently, Patel and colleagues found that patients only utilized 10% of the oral morphine equivalents (OMEQ) that were prescribed after radical prostatectomies. 7 Unfortunately, to date, there is no study directly comparing pain levels between patients managed with opioid and nonopioid protocols, and how nonopioid protocols can be implemented after common surgeries.
In this quality improvement initiative, our objective was to evaluate a novel, nonopioid protocol with an escalation pathway after robot-assisted urologic surgeries. We hypothesized that the protocol would decrease the amount of narcotics on discharge, and that the majority of patients undergoing robotic procedures do not require opioids for adequate pain control at discharge.
Materials and Methods
Study cohort
In September 2018, we began a quality improvement initiative, the Preventing excess narcotic prescriptions in new robotic surgery discharges (PENN) Initiative, to reduce the number of narcotics prescribed upon discharge in our robot-assisted radical prostatectomy (RARP), robot-assisted radical nephrectomy (RARN), and robot-assisted partial nephrectomy (RAPN) population at the Hospital of the University of Pennsylvania. All patients undergoing these procedures were eligible and included in the study. Exclusion criteria included patients who underwent an open surgery. We did not exclude patients with a baseline opioid requirement, as we aimed to provide a standardized postoperative pain regimen to address surgical pain in all patients. All robotic surgeries were performed using the DaVinci Xi platform system.
Pain management protocol
The PENN Initiative is a standardized nonopioid analgesia pathway with escalation options, which was implemented in September 2018 across the continuum of care with preoperative, intraoperative, and postoperative treatments (Fig. 1). Based off of previous studies showing the efficacy of oral gabapentin and acetaminophen in the perioperative setting, 4,5 one dose of gabapentin 300 mg and acetaminophen 975 mg was given preoperatively approximately 1 hour before surgery. Intraoperatively, a total of 30 cc of 0.5% bupivacaine was administered in all robotic port sites before incision. All RAPN cases in this cohort were performed using a transperitoneal approach. In our cohort, all patients had five incisions, including one extraction site with a fascial closure; skin was closed with absorbable sutures.
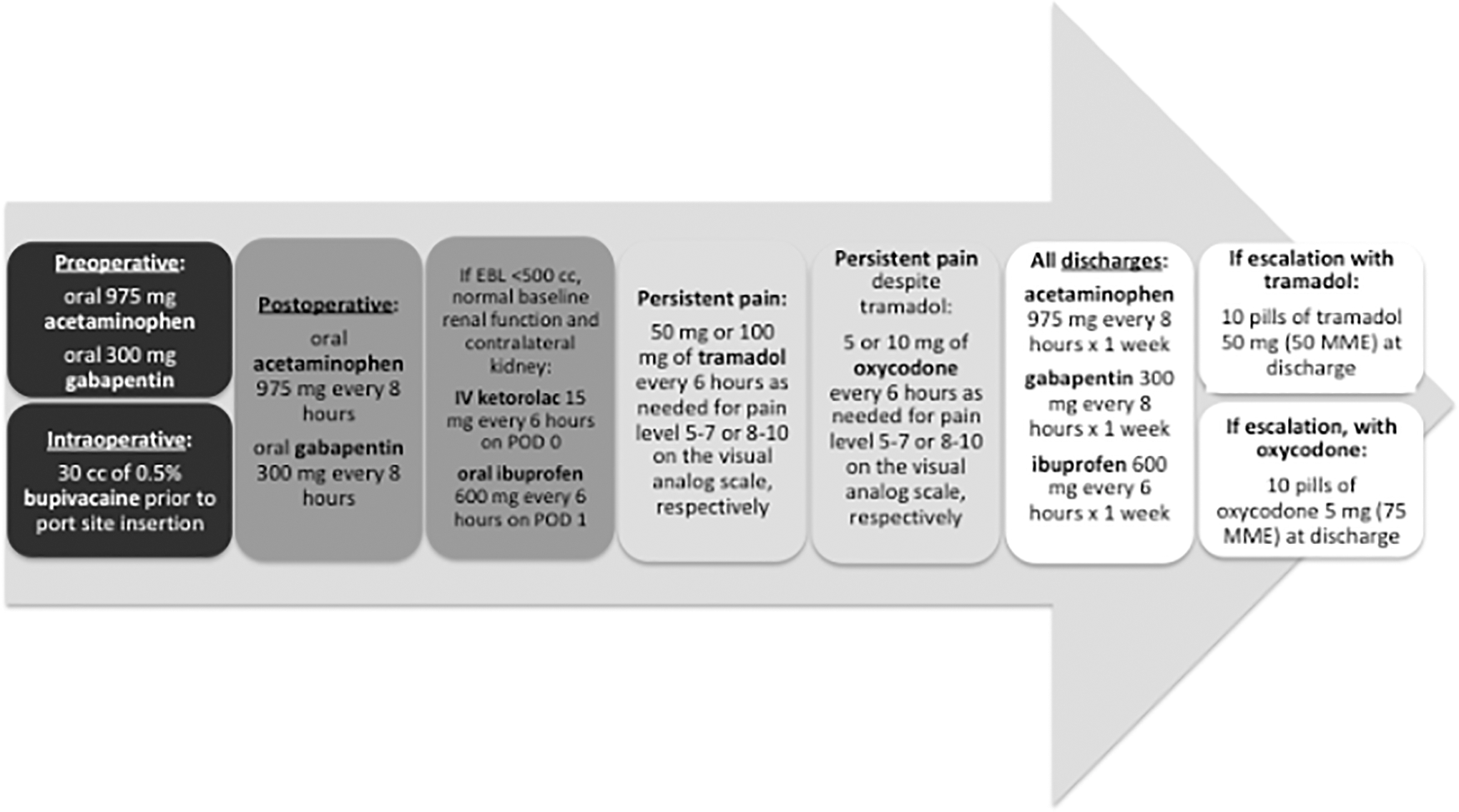
PENN QI opioid-free pilot pain management pathway. PENN = preventing excess narcotic prescriptions in new robotic surgery discharges.
Postoperatively, all patients received standing gabapentin 300 mg every 8 hours orally and acetaminophen 975 mg every 8 hours orally. Ketorolac 15 mg intravenously every 6 hours was given for the first postoperative day (POD) followed by ibuprofen 600 mg every 6 hours standing on subsequent days if the patients met the following criteria: baseline creatinine level <1.4 mg/dL, normal contralateral kidney, and estimated intraoperative blood loss <500 cc. Post-RARN patients did not receive ketorolac. All patients post-RARP were discharged with an 18F urethral catheter. In our overall cohort, all post-RARP and RAPN patients underwent 19F Blake drain placement intraoperatively, but all were removed before discharge. No patients were discharged with drains.
An escalation pathway was implemented for patients who complained of persistent pain not controlled by the standing nonopioid regimen. First, patients were given 50 or 100 mg of tramadol every 6 hours as needed for pain level 5–7 or 8–10 on the visual analog scale, respectively. Then, if requiring further escalation, patients were given 5 or 10 mg of oxycodone every 6 hours as needed for pain level 5–7 or 8–10 on the visual analog scale, respectively. All patients, regardless of escalation status, were discharged on the standing non-narcotic protocol to continue until their postoperative outpatient visit, which was usually scheduled between POD 6 and 7. If requiring escalation with tramadol, they were discharged on 10 pills of tramadol 50 mg (50 OMEQ). If requiring escalation with oxycodone, they were discharged on 10 pills of oxycodone 5 mg (75 OMEQ). We recorded the pain scores measured in the preoperative area, ∼1 hour before surgery, as well as the morning of postoperative day 1, as measured by nursing.
All housestaff and advanced practice providers involved in inpatient and outpatient prescribing after robotic surgery were provided with educational materials outlining PENN Initiative. We worked closely with the Informatics Department to adjust the computerized physician order entry and adjust the preferences in the electronic health record so that providers would preferentially select the PENN initiative orders perioperatively.
Analysis
All patients who underwent any of the three robotic urological surgeries from September 1, 2018, to January 9, 2019 were included in this analysis. Our primary outcome was discharge narcotic prescribing rate, as measured by the percentage of patients who were discharged without narcotic, with 10 pills of tramadol (50 OMEQ), and with 10 pills of oxycodone (75 OMEQ). As a secondary outcome, we also examined the rate of escalation to the use of narcotics in the inpatient setting, which was similarly calculated as the percentage of patients who were escalated to either tramadol or oxycodone every 6 hours as needed, although admitted.
As a balancing measure to assess the adequacy of the pain control protocol, pain levels were measured using the visual analog scale, which rates pain levels from 0, no pain, to 10, highest intensity of pain. Pain levels were measured in the preoperative holding unit approximately 1 hour before surgery, the morning of POD 1, and at the first postoperative outpatient visits (POD 6 or 7). To assess the safety of our protocol, we analyzed the number of telephone encounters and emergency room visits for any reason and specifically for pain between the discharge date and first postoperative outpatient visit through chart review.
Univariable analyses were performed using chi-square tests and Kruskal–Wallis for categorical variables and continuous variables, respectively. Multivariable logistic regression was performed to determine the associations of between demographic factors (age, sex, race, and prior abdominal surgeries) or perioperative characteristics (operative time, estimated blood loss, and length of stay) and the need for an opioid prescription at discharge. A p-value of <0.05 (two sided) was considered statistically significant and all the analyses were performed using STATA 15 (StataCorp LP, College Station, TX). This project was reviewed and determined to qualify as Quality Improvement by the University of Pennsylvania's Institutional Review Board.
Results
A total of 170 consecutive patients were available for analysis, of which 87 (51.2%) underwent RARP, 58 (34.1%) underwent RAPN, and 25 (14.7%) underwent RARN. Overall, median operative time was 2 hours and 13 minutes, median estimated blood loss was 100 cc, and median length of stay was 1 day. Additional baseline demographic and surgical characteristics are described in Table 1.
Baseline Preoperative and Perioperative Characteristics
BMI = body mass index; EBL = estimated blood loss; IQR = interquartile range; LOS = length of stay; RAPN = robot-assisted partial nephrectomy; RARN = robot-assisted radical nephrectomy; RARP = robot-assisted radical prostatectomy.
A total of 67.7% (115/170) of patients were discharged without a narcotic prescription, 24.1% (41/170) were discharged with 10 pills of tramadol 50 mg (50 OMEQ), and 8.2% (14/170) were discharged on 10 pills of oxycodone 5 mg (75 OMEQ). Figure 2 illustrates the rates of discharge prescribing stratified by the robotic procedure type.

Percentage of patients discharged with and without narcotic escalation.
There were no significant baseline demographic or surgical characteristic differences between patients who were discharged without narcotics, with tramadol escalation, or with oxycodone escalation (p = 0.11). Pain scores collected on POD 1 did show a significant difference: median pain score among the non-narcotic, tramadol escalation, and oxycodone escalation populations were 2, 3, and 5, respectively (p = 0.007). Pain scores returned to normal and demonstrated no difference across any of the groups by the 1-week postoperative visit (p = 0.66). Of the 24.1% (41/170) patients discharged on tramadol, two patients had a history of prior opioid usage. Of the 8.2% (14/170) patients discharged on oxycodone, four patients had a history of prior opioid usage.
On multivariable analysis, age was the only demographic or surgical characteristic associated with requiring a narcotic prescription upon discharge. An increasing age by 1 year was associated with an odds ratio of 0.961 (95% confidence interval: 0.923–0.995, p = 0.026) (Table 2).
Multivariable Analysis of Demographic and Perioperative Variables Associated with Discharge Narcotic Prescription
CI = confidence interval.
There was no significant difference between the number of telephone encounters documented in the electronic medical record between patients who were discharged with and without narcotic (p = 0.42). There were 7 (4%) emergency room visits in the overall cohort, and only two of these visits had a documented chief complaint related to pain. The first patient, status postrobotic radical nephrectomy, presented with pleuritic chest pain and underwent negative evaluation for a pulmonary embolism. The second patient presented with abdominal pain and was found to have appendicitis on cross-sectional imaging.
Discussion
In this prospective quality improvement initiative, we demonstrated that the majority of patients who undergo robotic urological procedures can have adequate pain control with a nonopioid analgesia pathway before utilization of narcotic medications. Within our institution, we decreased our opioid prescribing rates in this cohort from 100% to 32.3%. Furthermore, of those requiring narcotics, the minimum OMEQ was decreased by 33.3% from 75 to 50, and the maximum OMEQ prescribed was decreased by 36.2% from 117.5 to 75.
It is unfortunate that prolonged narcotic use should now be considered one of the most common long-term complications after undergoing any operation. 2 Beyond the issue of personal use, the release of opioids into the community is a major concern. The majority of opioids are not properly stored or appropriately disposed of with some estimates placing disposal as low as 9%. 6 These findings highlight the surgeon's contribution to this national crisis.
Specifically, urologists are also guilty of overprescribing opioids after surgery. In a cohort of 587 patients who underwent urologic surgery at a single institution, surveys administered to patients 2–4 weeks after their procedure demonstrated that 67% of patients reported unused narcotics. 3 Of those with excess pills, 91% retained leftover medication at home for future use. 3
This practice of overprescribing was the impetus for our intervention. We began with robotic surgery as prior studies have demonstrated that this is a population most commonly provided with narcotic prescriptions at discharge despite most patients reporting minimal need and use. For example, in a recent analysis of robotic prostatectomy cases, 83.9% consumed equal to or less than 112.5 OMEQ (15 pills of 5 mg oxycodone). Within their robotic radical prostatectomy population, only 10% of patients did not fill their opioid prescription and there was an association between the amount of opioid prescribed and the amount of opioid consumed. 7 This suggests that the number of pills prescribed may be more impactful than the dosage or strength. In addition, 87% of patients reported retaining their leftover narcotic pills, despite having no narcotic consumption requirement. 7
We observed a similar trend in our cohort after RARP. A total of 80.5% (70/87) of RARP patients did not require a discharge narcotic. Of those discharged with opioids, 12.6% were discharged with tramadol (50 OMEQ) and 6.9% were discharged with oxycodone (75 OMEQ). The majority of RAPN patients also did not require opioids upon discharge (58.6%, 34/58).
However, similar findings were not demonstrated within the RARN; the majority of patients did require additional analgesia with narcotics. Only 44% (11/25) of patients after robotic radical nephrectomy were sent home without either tramadol or oxycodone. Despite the need for additional narcotics, our protocol still demonstrated a decrease overall compared to our preimplementation prescribing. The increased utilization of opioids in the RARN population may be a reflection of a larger extraction site compared to partial nephrectomy or prostatectomy.
The issues of opioid exposure and diversion after surgery highlight the utility of a baseline non-narcotic protocol, which eliminates the exposure to otherwise opioid-naive patients who do not need the therapy. Our PENN postoperative pathway marks an incremental step toward achieving this goal and represents the only multimodal non-narcotic pain management strategy after robotic surgery described in the literature.
Our study had several limitations. First, our cohort consisted of a subset of patients who underwent robotic surgery at a single institution, which limits the generalizability of our results. In addition, although we did record preoperative narcotic use, which was few overall, we did not quantify the degree and length of prior use. This represents potential confounders, as patients with prolonged use and higher doses would have higher postoperative pain medication requirements. Future iterations of our protocol will include the collection of validated patient-reported outcomes, as well as medication logs to record accurate utilization rates after discharge. Although we did compare pain scores at various time points, these varied slightly in that patients had outpatient visits that varied by one POD (6 or 7). Finally, this was a quality improvement study, not a randomized controlled trial; therefore, we cannot draw comparative conclusions regarding pain control between patients who were discharged with and without opioids.
Despite these limitations, our study provides evidence that an initial non-narcotic analgesia pathway with escalation to use of opioids only when appropriate is safe, reduces total narcotic dispensed, and appears to adequately control postoperative pain at discharge. Our initiative illustrates a simple way to dramatically reduce the amount of opioid medication released into the community. This hopefully will be an iterative step toward further evidence-based studies and prescribing guidelines after urological surgery.
Conclusion
Through the standardization of a standing, non-narcotic pain regimen spanning from the preoperative, intraoperative, and postoperative period, we were able to discharge the majority of patients undergoing robotic surgery without any opioids. Implementation of this protocol across institutions can lead to opioid stewardship within urology.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.