
Abstract
Introduction:
This study aims to describe robot assisted surgery of the inferior vena cava (IVC) by assessing techniques utilized, perioperative outcomes, complications, and long-term patency of the IVC.
Methods:
A retrospective review was performed on all robotic surgeries involving dissection and repair of the IVC at our institution. Patient characteristics, operative reports, and follow-up visits were analyzed. Preoperative and postoperative imaging was independently reviewed by a single radiologist to determine changes in IVC diameter. Complications were analyzed according to early (<30 days) vs late (>30 days).
Results:
Thirty-four patients underwent robot assisted surgery of the vena cava from 2008 to 2018. Twenty-six cases were performed for urologic malignancy, four were performed for IVC filter explantation, and four renal vein transpositions were performed for nutcracker syndrome. Twenty-four of the 26 patients with urologic malignancy underwent radical nephrectomy with IVC tumor thrombectomy. Three cases were converted to open. Median length of stay was two nights, and mean estimated blood loss (EBL) was 375 mL. There were five complications, ranging from Clavien-Dindo grade II–IIIa, four of which were early complications. No patients required return to the operating room, and there were no perioperative mortalities. IVC diameter was reduced by 41% on axial diameter, with no patients experiencing compromised venous return.
Conclusion:
Robot assisted surgery offers the advantage of minimally invasive surgery with the ability to apply open surgical principles. In our series, an experienced multidisciplinary team approach yielded low EBL, short length of stay, and low complication rates.
Introduction
Robot assisted surgery of the inferior vena cava (IVC) has been increasingly utilized as a minimally invasive alternative to a traditionally open approach. This surgical technique has been primarily described for renal masses with tumor thrombus; however, similar principles can be applied to other less commonly performed procedures such as removal of IVC filters (IVCFs) and left renal vein transposition (RVT) for nutcracker syndrome (Fig. 1). 1 –3 Benefits of the minimally invasive approach using robotic assistance can be extrapolated from its application for other operations, namely with benefits from three-dimensional visualization, reduced estimated blood loss (EBL), and shorter hospitalization. 4 The degrees of freedom afforded by a robot platform enables surgeons to deal with these potential complications early and effectively by adhering to well-established open surgical techniques.
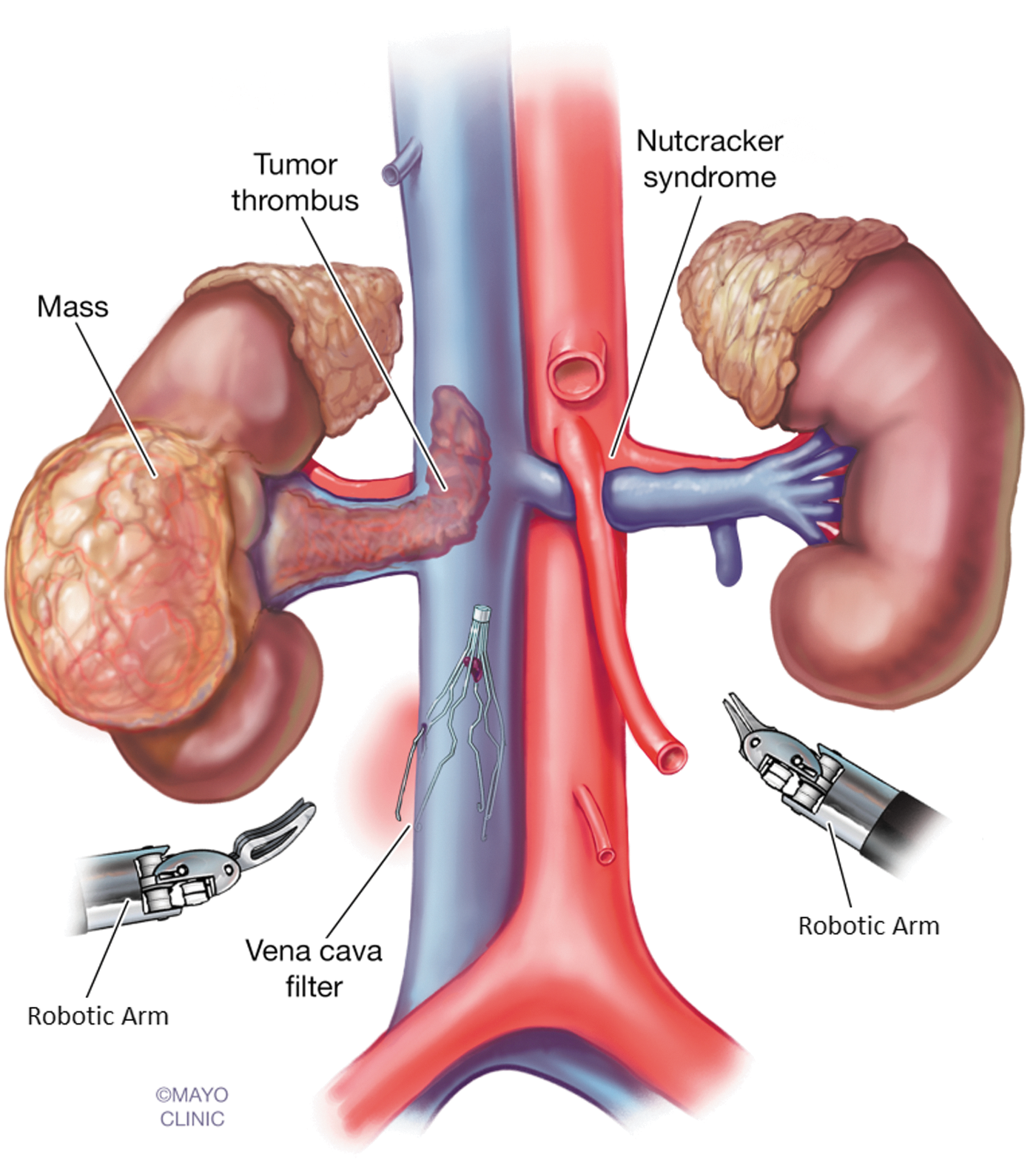
Robot assisted surgery of the IVC. IVC = inferior vena cava.
Currently, there is a paucity of data assessing surgical outcomes, complications, and long-term follow-up after robot assisted vena cava reconstruction and repair. Although the benefits and complications of robotic nephrectomy with level I and II tumor thrombi have been described in the literature, it is unclear if these can be extrapolated to other robotic procedures involving the IVC. In the open approach, thromboembolism was frequently noted and linked to a greater risk of mortality rate in patients undergoing radical nephrectomy with tumor thrombus. 5 For this reason, we sought out to determine the rates of thromboembolism in the robotic setting and assess its relationship with IVC diameter and postoperative patency.
This series aims to describe robot assisted IVC procedures performed at a single institution and assess outcomes, complications, and long-term patency of the IVC.
Methods
After institutional review board approval, a retrospective review of all robotic procedures involving the IVC performed by a single surgeon at Mayo Clinic Arizona from January 2008 to August 2018 was performed. Procedures involving dissection, mobilization, incision, and closure of the IVC in each case were included. Robotic cases requiring open conversion were included in the analysis. Patient characteristics, operative reports, anesthesia reports, and postoperative encounters were analyzed. Images were reviewed by a single radiologist to describe IVC tumor thrombus, as well as IVC diameter in the sagittal and axial dimensions for patients who had comparable preoperative and postoperative imaging modalities.
Robot assisted mobilization of the vena cava was conducted adhering to open surgical principles. Namely, this included: Complete dissection and vascular isolation of the IVC with ligation and division of lumbar veins. Proximal and distal control of the IVC, as well as contralateral renal vein with modified Rummel tourniquets and robotic bulldogs. Modified Rummel tourniquets consisted of twice-wrapped vessel loops, with a sliding locking clip for cinching Utilizing a multidisciplinary approach with the intraoperative consultations of urologic, vascular, and hepatobiliary teams as deemed necessary
In patients undergoing robotic radical nephrectomy for renal cell carcinoma (RCC) with tumor thrombus, we characterized venous tumor thrombus (VTT) level according to the standardized Mayo Clinic classification (Fig. 2). 6 Cases with thrombus limited to the renal vein (Level 0) were excluded. Importantly, we did not characterize the tumor thrombus as a Level III unless the extent of the tumor reached the confluence of the major hepatic veins. Antiplatelet/anticoagulation (AP/AC) regimens were described according to the agent used and duration of therapy. Complications were graded using the Clavien-Dindo Classification system at 30 and 90 days postoperatively. 7 Mean and median values were reported with their standard deviation and interquartile range (IQR), respectively.

Mayo Clinic classification of tumor thrombus.
Results
Thirty-four cases were included in our review, including 4 (12%) IVCF explantations, 4 (12%) left RVTs, and 26 (76%) procedures performed for urologic malignancy (24 RCC with VTT and 2 retroperitoneal masses with IVC invasion). Of the 24 RCC with VTT, 19 (79%) patients were right sided tumors, while 5 (21%) were left sided. Patient characteristics, operative information, and complications are described in Table 1.
Patient and Perioperative Characteristics
Median values are reported with IQRs in parentheses.
AP/AC = antiplatelet/anticoagulation; ASA = American Society of Anesthesiologists; EBL = estimated blood loss; IQR = interquartile range; IVCF = inferior vena cava filter; LOS = length of stay.
Three nephrectomies with tumor thrombi required conversion to open, none of which was performed in an emergency. Early in our experience, two cases converted to open to optimize control of the retrohepatic vena cava; one of these confirmed tumor thrombus above the level of robotic extent for proximal vascular control, and the other was performed to rule out proximal bland thrombus. The third case was converted due to venous bleeding from a posterior lumbar vein, which could not be controlled robotically. Thirty-three cavotomies were closed primarily, and one IVC was ligated secondary to asymptomatic preoperative IVC occlusion. No patients required interposition grafting or patch placement of the IVC. Twenty-five (74%) IVC reconstructions were performed with polypropylene (3–0 to 5–0), and eight (24%) reconstructions were performed with Gore-Tex® suture.
In patients with VTT, the median extension of tumor into the IVC was 4.15 cm. Thrombus levels included 2 (8%) level I thrombus, 21 (88%) level II thrombi, and 1 (4%) level III, which required conversion to open. Bland thrombus was present in 6 (19%) patients, all of whom had RCC with tumor thrombus. Retroperitoneal lymphadenectomy was performed in 22 (67%) patients, hepatic mobilization in 3 (9%) patients, and only 1 (3%) patient required a Pringle maneuver.
Table 2 lists the frequency of AP/AC regimens utilized by time surrounding surgery. Preoperatively, 29 (85%) patients were placed on AP/AC. Low molecular weight heparin (LMWH) was the most commonly used agent in the preoperative setting (17 patients, 59%). Intraoperative heparin was administered in 30 (94%) cases, and protamine was given as reversal in 12 (35%) patients at a median (IQR) dose of 30 (20–48) mg upon closure of the IVC. In the postoperative inpatient setting, 28 (82%) patients received subcutaneous unfractionated heparin as primary agent, bridging agent, or in combination with antiplatelet therapy. On discharge, 27 (79%) patients were discharged on AP/AC, with LMWH being most commonly used in 17 (63%) of those patients. Seven patients were maintained indefinitely on AP/AC, all of whom had preexisting conditions requiring continuous therapy, such as prior thromboembolism or coagulopathy. Of the 14 patients discharged on limited duration of AP/AC, the median duration of therapy was 14 days (IQR 14–30 days).
Antiplatelet and Anticoagulation Regimens Utilized in Robot-Assisted Surgery of the Inferior Vena Cava
AP+AC = combination antiplatelet and anticoagulation; ASA = aspirin 81 or 325; LMWH = low molecular weight heparin; Xa = factor Xa.
Complications occurred in five (15%) patients. There were no intraoperative or perioperative deaths. There were four (12%) Clavien-Dindo grade II complications within 30 days. These included a pulmonary embolus (PE), deep venous thrombosis (DVT), intraoperative hemorrhage requiring transfusion, and retroperitoneal hematoma managed nonoperatively. No patients required return to the operating room, and there were no mortalities within 90 days. The patient who returned with a PE had known metastatic disease before surgical resection. One patient developed a late grade III-A complication of pleural effusion requiring thoracentesis, who had known pancreatic metastasis.
Postoperative abdominal imaging was completed in 12 (35%) patients, at a median of 340 days (IQR 19–765 days) postoperatively. In all imaging studies, the vena cava was patent. The median (IQR) percent reduction in IVC diameter was 41% (29%–62%) on axial diameter and 63% (50%–72%) on sagittal diameter. The two patients with thromboembolic complications had a reduction in IVC axial diameter of 65% in the patient with PE and 29% in the patient with DVT.
Discussion
This series demonstrates that robot assisted IVC surgery can be performed by an experienced surgeon and multidisciplinary team, yielding low EBL, transfusion rates, thromboembolic events, and a short length of stay. In urologic oncology, robot assisted IVC surgery has gained popularity in recent years for RCC with VTT. At our own institution, the use of robot assisted radical nephrectomy with IVC thrombectomy has increased over the past decade, as outlined in Figure 3. The robotic technique has been described for VTT Level I–III 8,9 and even utilized in a hybrid manner as the initial dissection of a level IV cavoatrial thrombectomy. 10 Compared to the open approach, a retrospective review concluded that robotic nephrectomy with tumor thrombectomy offered favorable perioperative outcomes with no significant difference in progression-free survival between the robotic and open groups. 4 Of note, the median length of stay of 2.5 nights in our patients was favorable to previously published reports of 4 to 5 nights. 4,9

Surgical approach utilized for radical nephrectomy with tumor thrombus over 20 years of experience.
Current controversy exists regarding the VTT level, which becomes paramount in surgical decision making on whether to approach tumor thrombi robotically or open. In 1987, Neves and Zincke from Mayo Clinic described four levels of VTT as renal, infrahepatic, intrahepatic, and atrial. 11 While the authors did not classify these levels numerically, another study from the same institution further classified these by describing numeric levels by major venous landmarks. 6 In this study by Blute and colleagues in 2004, the major hepatic venous confluence served as the landmark dividing VTT level II and III. This becomes of critical importance, as recent case series have described the robotic approach of level III tumor thrombi while citing the Neves and Zincke classification. 8,9 If we applied this classification to our own data, we would have 2 level I, 11 level II, and 11 level III thrombi. This is in large contrast to our current classification of 2 level I, 21 level II, and 1 level III. We chose to describe our tumor thrombus levels according to the classification system used by Blute and colleagues because we utilize the hepatic venous confluence to guide our decision to approach these cases open vs robotically. The anatomic zone between the hepatic confluence and the diaphragm is a narrow region where obtaining proximal vascular control may be difficult. In the event a sternotomy is required, the robot will require de-docking while the tumor thrombus remains in the vena cava, placing the patient at significant risk for hemorrhage and mortality rate.
Robot assisted surgery was also utilized for several vascular procedures with IVCFs and RVT. Long-term indwelling IVCFs represent a hazard that can lead to overall perforation in as much as 19%. In a review article by Jia and colleagues, 40% of patients with symptomatic filter penetration required surgical intervention. 12 With standard endovascular retrieval success rates reported near 73%, 13 physicians have attempted alternative methods after failed retrieval, including various lassos, sheaths, and endobronchial forceps. 14 Previously, when endovascular methods of IVCF retrieval failed, the only option was open surgical explantation. The robot assisted transabdominal approach offers a safe alternative without the morbidity associated with open surgery. Similarly, the use of robotics to perform RVT in nutcracker syndrome avoids the need for celiotomy and is significantly more feasible than simple laparoscopic venous transposition due to the extensive amount of vascular suturing required. 1,3 In our experience, we found RVTs to be the most straightforward and reproducible of the three techniques described above.
Complications in this series occurred in 15% of cases, all of which were Grade III or lower. Thromboembolic events included one PE and one DVT (total 7% incidence), both of which occurred in nephrectomy with tumor thrombus cases. Rates of thromboembolic complications were previously reported in the Level I–III VTT groups to range from 3.6% to 7.6% in the open literature. 6 More recently, a retrospective study specifically analyzing thromboembolic disease following radical nephrectomy with tumor thrombus noted a 30- and 90-day incidence of thromboembolic events to be 17% and 22%, respectively. 5 This study identified a higher risk of thromboembolism in patients with a smoking history, poor performance status, coagulopathy, and bulky lymphadenopathy of the retroperitoneum and noted that the incidence of thromboembolism was 18% in postoperatively anticoagulated patients vs 36% in patients who were not. Comparing our own data, we do not appreciate an increased risk of venous thromboembolism with robot assisted surgery compared to these previously published reports on open surgery. There were no intraoperative or perioperative mortalities reported in this series. This may be a reflection of case selection, given that other open series report a mortality rate of as much as 4.6% in level I–III open nephrectomy with thrombectomy. 6,15,16 Median EBL for all cases in our series was 400 mL. Low blood loss can possibly be attributed to the tamponade effect from the pneumoperitoneum, as well as meticulous hemostatic control afforded by the dexterity and increased visualization of the robotic platform.
The optimal prophylaxis and treatment of thromboembolism in the setting of tumor thrombectomy and IVC reconstruction have not been clearly established. Boorjian and colleagues described the use of preoperative anticoagulation in patients with evidence of bland thrombus undergoing open surgery and then utilized intravenous unfractionated heparin for close monitoring to ensure therapeutic levels. 16 One series of robotic nephrectomy with VTT utilized prophylactic dose of LMWH for 30 days postoperatively. 8 In our series, one patient experienced DVT and one patient suffered a pulmonary embolism, both of which required therapeutic anticoagulation. The selection of the optimal AP/AC regimen is complex and devoid of evidence based guidelines. Several factors are taken into consideration when defining a postoperative AP/AC regimen, including presence of preoperative and postoperative DVT/PE, clot propagation, and risk of perioperative hemorrhage. However, it is possible that given the quicker return to baseline mobilization and regular activities of daily living, extended-duration prophylactic anticoagulation may not be necessary in robotic setting. Overall, RCC patients are likely at an increased risk of DVT/PE in the preoperative and perioperative setting given the presence of malignancy, and consideration should be given toward anticoagulation administration. Our practice in patients with urologic malignancy has been to administer anticoagulation preoperatively to patients without ongoing bleeding from the urinary tract to prevent bland thrombus formation, followed by prophylactic anticoagulation for 30 days postoperatively. In patients with IVCFs, many present therapeutic anticoagulation and are maintained for roughly 2 to 4 weeks postoperatively, although there is no well-defined regimen.
In our series, all but one cavotomy was closed using a running primary closure with nonabsorbable suture (polypropylene or Gore-tex). While alternative options for IVC repair include interposition grafting or patch angioplasty, primary repair enables shorter IVC reconstruction times with lower risk of complications such as graft infection. Primary closure can, however, cause IVC stenosis. 17,18 One study analyzing the postoperative IVC diameter found that open repair created a less than 20% reduction in the IVC diameter without compromising lower extremity venous return. 19 Our series demonstrated median IVC diameter to be 58% of the preoperative axial value. Despite this reduction, no patients had postoperative lower extremity swelling or signs of lower extremity venous stasis.
Limitations of this study include its retrospective nature, sample size, and heterogeneity of patients. Age groups were markedly different between groups, likely due to underlying indication for surgery. Likewise, duration of procedure, EBL, and length of stay may have been influenced by a larger degree of dissection required for cases performed for urologic malignancy. Although we stratified nephrectomy with tumor thrombus patients by VTT level, there may have been a selection bias in that patients with complex anatomy were chosen to undergo open excision and repair and, thus, were excluded from this review. This highlights the importance of appropriate patient selection for robotic cases involving the IVC. Future studies should directly compare the open and robotic approach in various surgeries involving the IVC. While retrospective reviews have been published and well received, the direct comparison of matched, randomized control trials comparing the two modalities would be of paramount value.
Lessons learned and evolution of technique
Over the past several years, our surgical approach to the IVC has been modified in several ways (Table 3). We utilize a multidisciplinary approach for numerous cases, including radical nephrectomy with tumor thrombus, complex testis cancer, and retroperitoneal vascular surgeries. A robotically trained vascular surgeon is available and in the operating room for guidance and assistance regarding complex vascular reconstruction. Importantly, this intraoperative consultation guides the decision for primary closure vs patch or interposition grafting. In our series, the intraoperative evaluation of the IVC was felt to leave less than 50% stenosis in almost all cases. There was one case in which infrarenal IVC ligation was considered the safest approach. While we are prepared for intraoperative patch angioplasty, we did not feel compelled to do so in any specific case. Finally, the hepatobiliary service is available if open conversion is needed and to provide guidance during advanced hepatic mobilization, such as caudate lobe mobilization.
Lessons Learned from Robotic Surgery of the Inferior Vena Cava
IVF = inferior vena cava.
We have taken advantage of the pivoting boom on robotic platforms, making the need for undocking and repositioning sparse. Our first step in the surgical approach to the IVC for right-sided renal masses includes dissection of the interaortocaval space, which not only exposes the great vessels but also aids in identifying and allowing for immediate control of the right renal artery in cases of radical nephrectomy. This method decreases bleeding when mobilizing the kidney and additionally minimizes bleeding from parasitic vessels around the primary renal mass once the inflow is cut off. The benefits of this approach allow us to avoid endovascular embolization. Finally, this critical step is required during the radical nephrectomy, and we therefore prefer to perform it as our first step. For left sided tumors, we adhere to the same surgical principle of kidney mobilization and renal artery ligation before incising the IVC. In these cases, we will begin with the patient in the modified left lateral position and completely isolate and mobilize the left kidney, leaving it attached only by the renal vein. We will then re-dock in the right lateral position and address the tumor thrombus at the vena cava. When free, the tumor thrombus is then delivered under the window in the mesentery for safe and immediate placement into a specimen bag. To complete the procedure utilizing the same open surgical principles and maintain integrity of the thrombus, left sided tumors do require repositioning and re-docking of the robot.
During dissection and isolation of the IVC, we advocate for total control of lumbar veins. Of note, posterior lumbar veins are not encountered suprarenally, and realization of this landmark can save time during the procedure. We initially controlled lumbar veins using locking or titanium clips, but have transitioned to using suture ligature for large vessels and the EndoWrist One Vessel Sealer Extend™ in appropriately sized vessels. The use of the vessel sealer allows for division of lumbar veins with minimal thermal spread and is especially helpful in mobilization of the caudate lobe for suprarenal medial IVC exposure. We utilize intraoperative intracorporeal ultrasound, visualized through the robotic console and controlled by the surgeon in cases of VTT. This allows identification of the level of tumor or bland thrombus in real time, which guides our dissection to reach the point of proximal vascular control. Importantly, when performing thrombectomy, the kidney is completely mobilized and left dangling only by the renal vein before cavotomy. We use a modified Rummel tourniquet, with twice-wrapped vessel loops around the vein or IVC, which is then cinched with a locking clip. We have not found that these clips slip or loosen, but rather have found some cases in which complete cinching does not provide full occlusion, and therefore, additional control is needed. For this purpose, we will often utilize a robotic bulldog clamp on the distal IVC, where the pressure of venous return is highest. Interestingly, proximal control on the IVC is not as difficult to maintain as the pneumoperitoneum prevents retrograde flow of blood.
As a backup, we have a 5 mm straight laparoscopic DeBakey clamp available to access. When clamping the IVC before cavotomy, patients have not demonstrated a significant hemodynamic change in venous return and have never required extracorporeal circulation in any cases. During thrombectomy or removal of IVCF, we utilize robotic scissors to assist in stripping and excising the tumor or filter from the endothelium of the IVC. At least 3 minutes before IVC clamping and cavotomy, we routinely administer 3 to 5 thousand units of intravenous unfractionated heparin for thrombosis prophylaxis.
Cavotomies were traditionally closed using Prolene® sutures, which are ideal for open vascular repair, but can crimp and fray due to the grasping strength of the robotic jaws. Recently, we have incorporated the Gore-Tex monofilament stitch to our arsenal for cavotomy repair and rescue suturing; we prefer CV-4 suture on a TH-18 needle. The Polytetrafluoroethylene microstructure expands to fill the width of the hole created by the needle, with minimal surface area allowing for secure knot tying without compression or breakage. Finally, we feel that true level-III thrombi, which reach the hepatic venous confluence, can rarely be controlled in a safe manner from a strictly robotic approach. We advise that these patients are best served using an open approach in the event that a sternotomy is required. Figure 4 depicts the arsenal of robotic instruments and devices utilized in our current technique.
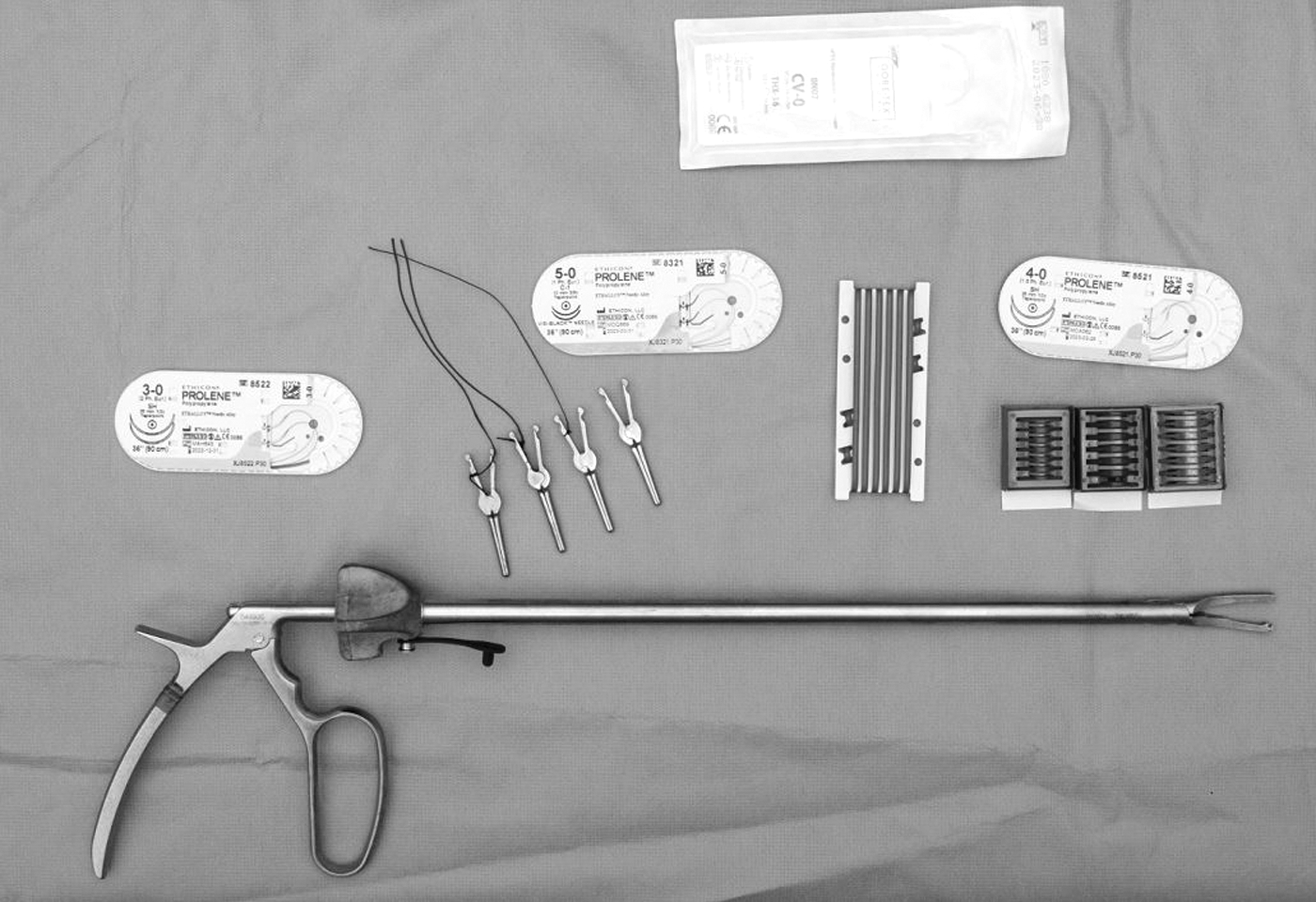
Arsenal of instruments, stitches, and surgical equipment used in robotic surgery of the IVC. Stitches include 3–0 to 5–0 polypropylene sutures, vessel loops and locking Clips, and robotic bulldog clamps.
Conclusions
Robot assisted IVC surgery appears to be a safe and effective option for pathology involving the IVC. We have demonstrated its use in robotic resection of urologic malignancy, IVCF explantation, and RVT. The advantages afforded by this approach include low EBL, short length of stay, and the ability to apply well-known and established surgical principles. This study also describes the use of anticoagulants commonly used perioperatively and postsurgical changes in IVC diameter. We demonstrate that an experienced multidisciplinary team approach to robotic surgery of the IVC yields excellent and consistent perioperative outcomes.
Footnotes
Author Disclosure Statement
K.M.R., A.K.N., H.M.A.-M., K.S.F., S.A.E., A.A.M., W.G.E., W.M.S., S.R.M., V.J.D., and E.P.C. have no commercial associations to disclose and have no conflicts of interest.
Funding Information
No funding was received for this article.