
Abstract
Objectives:
To evaluate the feasibility of robot-assisted fluoroscopy-guided (RAG) puncture and to compare RAG puncture, utilizing a novel robot system for percutaneous renal access, with ultrasound-guided (USG) puncture.
Materials and Methods:
We conducted a benchtop study with a renal phantom model using the automated needle targeting with an X-ray system. Seventeen urologists participated in this study and performed RAG and USG phantom punctures. The number of needle punctures, device setup time, and fluoroscopic exposure duration were recorded for the analyses.
Results:
The single puncture success rates of the RAG and USG punctures were 100% and 70.6%, respectively (p = 0.021). The median needle puncture time of RAG puncture was 24% shorter than that of USG puncture (35.0 vs 46.0 seconds; p < 0.001), and the median device setup time of RAG puncture was a minute longer than that of USG puncture (93.0 vs 30.5 seconds; p < 0.001). The median duration of fluoroscopic exposure of RAG puncture was longer than that of USG puncture (38.0 vs 6.5 seconds; p < 0.001). The surgeon's self-assessment results demonstrated that the participating urologists found RAG puncture to be safer and have better visibility than USG puncture; they were also more satisfied with RAG puncture. Subanalysis revealed that, in the RAG group, the attending surgeons had shorter total procedural time than the residents (p = 0.045).
Conclusion:
RAG puncture showed comparable results and accuracy rates with USG puncture for renal access.
Introduction
Percutaneous nephrolithotomy (PCNL) is a standard procedure for the treatment of large kidney stones, such as stones >20 mm and staghorn stones. 1,2 The common complications after PCNL are transfusion, fever, and thoracic complications. 3 To achieve the complete stone removal and mitigate renal bleeding, efficient and accurate tract placement into the renal collecting system is essential.
There have been several advances to improve the renal access technique. These include patient positioning access guide methods and navigation tool developments. For example, although the Clinical Research Office of the Endourological Society study reported that most PCNL cases were performed in the prone position, 4 the supine position resulted in a shorter mean operative time and a lower incidence of blood transfusions. 5 In addition, there is a debate regarding the optimal renal access methods (either fluoroscopy- or ultrasound-guided [USG] punctures). The USG puncture for renal access is feasible and could reduce patients' radiation exposure. 6 Zhu et al. reported in their randomized controlled trial that the USG mini-PCNL was as safe as the fluoroscopy-guided or combined technique for simple kidney stones, but the fluoroscopy-guided or combined technique was more effective for complicated stones. 7 A meta-analysis indicated that USG access resulted in shorter puncture time and lesser complications, including blood loss. 8 Another interesting access method utilizing ureteroscopy-assisted PCNL with electromagnetic guidance has been shown to be an effective and safe renal access technique in a previous trial. 9
We previously reported the efficacy of endoscopic intrarenal surgery, which utilized a flexible ureteroscope to assist percutaneous access and lithotripsy. 10 Although the combination of ultrasound (US) and fluoroscopic guidance has been our primary method for renal access, recent development in the US technique with real-time virtual sonography provided a safer access into the renal collecting system. 11
Among these technological innovations, the improvement of observation and computer-assisted optical puncture is the most significant development, which has greatly influenced our practice. Artificial intelligence (AI) and robotics are being introduced in the field of endourology. 12 These have led to increased investments of state-of-the-art devices. 13 The automated needle targeting with X-ray (ANT-X) robot-assisted device is the latest automated robot with AI for fluoroscopy-guided PCNL access. 14 The computer vision software performs fluoroscopic imaging analysis captured by the system to auto calibrate the navigation, with the algorithm calculating the required distance and direction and tilt angle compensation from skin to renal collecting system aimed. A previous article with a pig model demonstrated that this device reduced radiation exposure and complication after the procedure, which allowed us to compare the clinical efficacy between this new technology and the current renal access methods, such as USG.
In this study, we conducted a benchtop study utilizing the phantom kidney model to first evaluate the feasibility of robot-assisted fluoroscopy-guided (RAG) puncture by ANT-X for clinical use and to compare RAG puncture with USG puncture.
Materials and Methods
Study design
This prospective single-center benchtop study using renal phantom models was conducted at Nagoya City University (NCU) Hospital. Seventeen urologists, consisting of 12 residents and 5 attending surgeons from the NCU Hospital, participated in this study. The phantom models were donated by NDR Medical Technology (Singapore) and Nagase & Co., Ltd. (Tokyo, Japan).
All experiments were performed in the shockwave lithotripsy room at the NCU Hospital to be able to utilize fluoroscopy and were carried out on a single day in December 2018 to mitigate data collection bias.
Phantom models
To provide a variety of needle trajectories to the desired target, a three-dimensinal nonanthropomorphic phantom was designed by the NDR Medical Technology. Considerations during the design of the phantom were as follows: radiotranslucency, simplicity in construction, physiologically relevant physical size, and inclusion of different target diameter sizing. The size of the phantom was constrained to 170 × 130 × 75 mm to ensure that the entire phantom was visible within the field of view of clinical fluoroscopic systems. Each phantom consisted of five titanium target balls mimicking the lesions, which were 1 cm in size and separated from each other by 2 cm. These balls were also easily detectable in US view (Fig. 1).
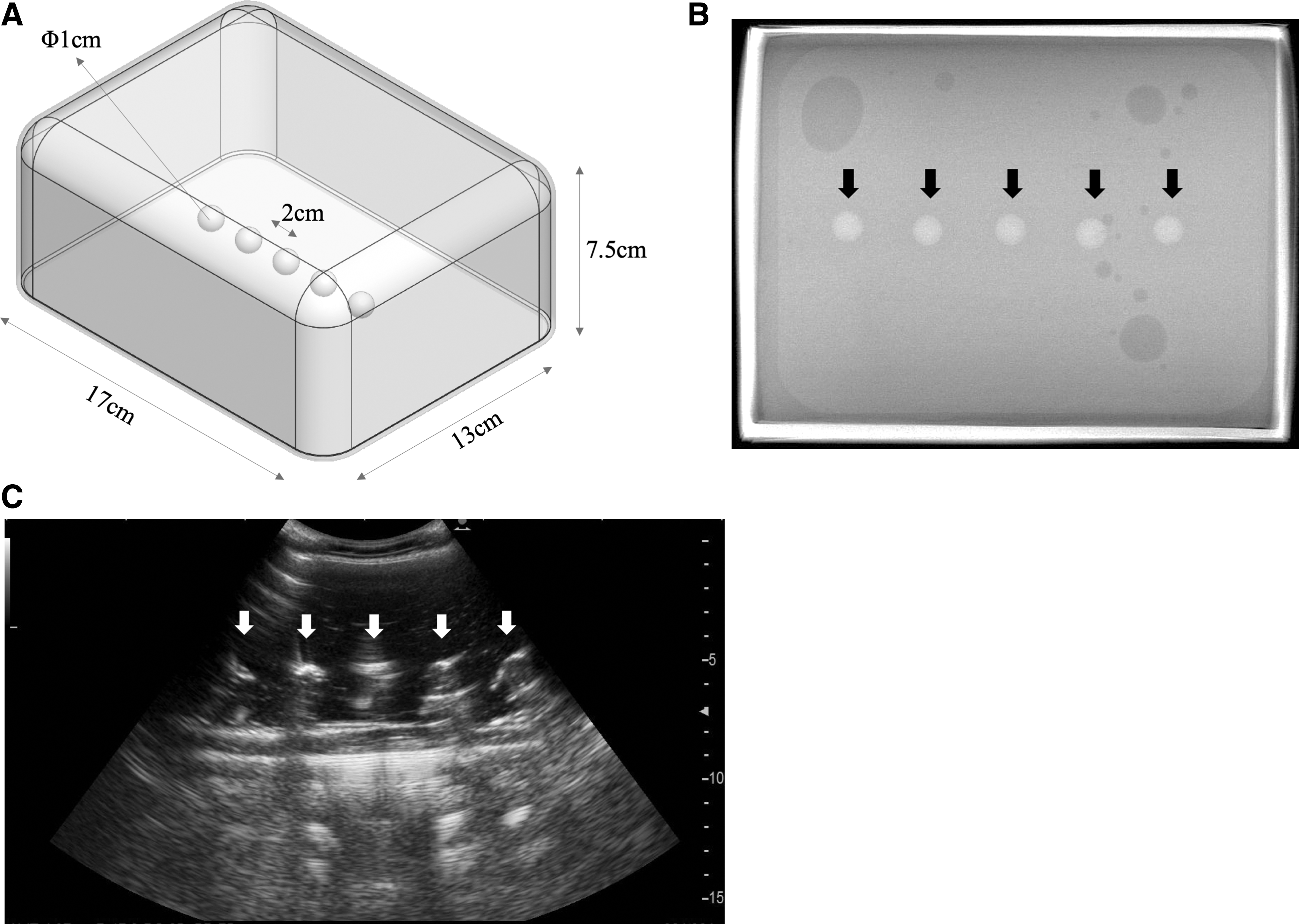
Appearance of a phantom model.
Participants and procedures
We divided the phantom model accesses according to the participating doctors into two arms, which were referred to as the RAG and USG groups. Both residents and attending surgeons performed a trial and an actual puncture using 18G needles in each group. Given that all participating doctors were familiar with USG renal access in their usual practice but had never experienced fluoroscopy-guided renal access, each participant observed a demonstration of RAG access, and then randomly performed US and RAG accesses to mitigate procedure bias. The background experience in renal access of the participants is summarized in Table 1. Location of target ball, duration of device setup, time and number of punctures, total duration of fluoroscopic exposure, and questionnaire responses for surgeons' self-assessments of the procedure were recorded (Fig. 2).
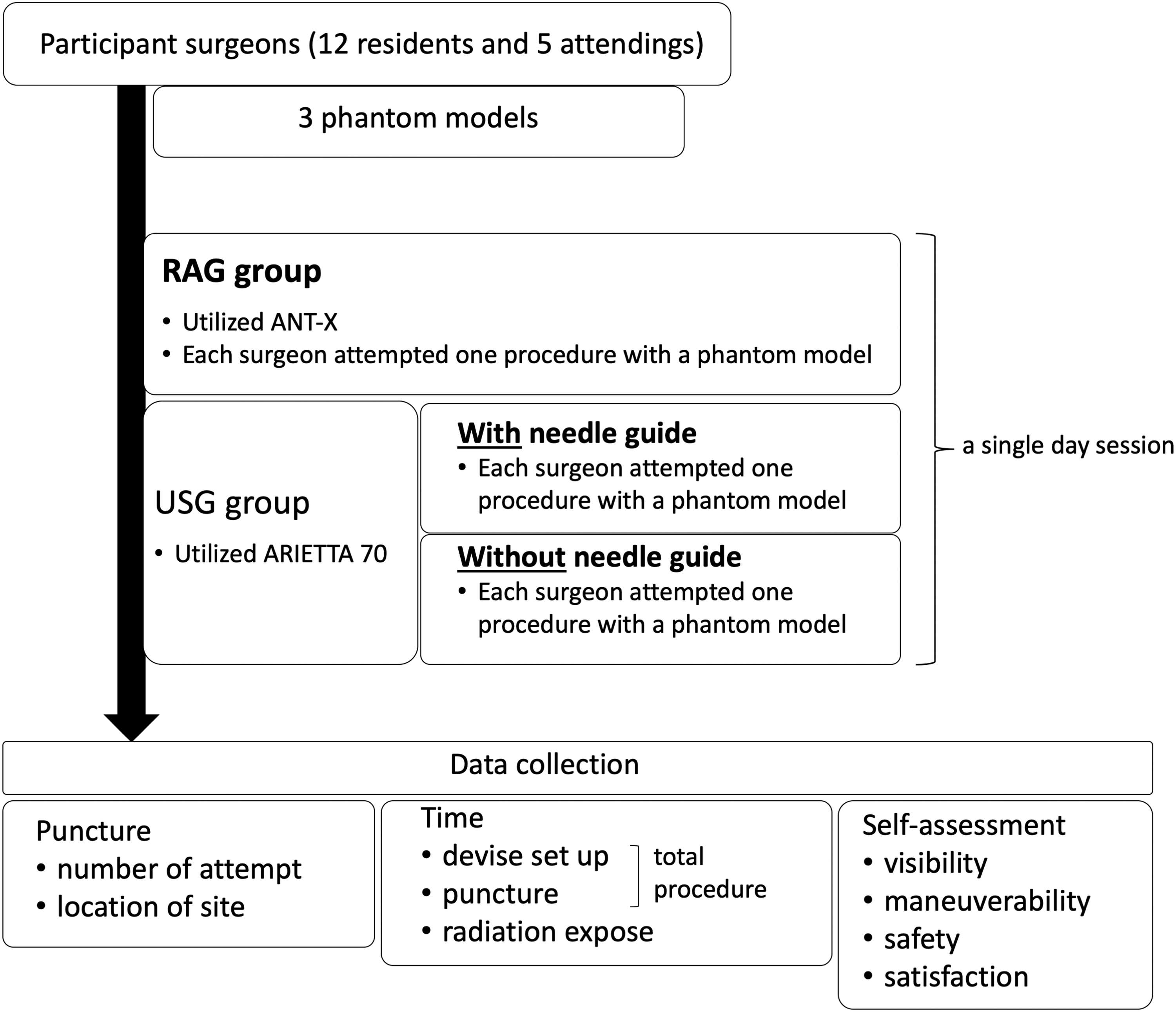
Study flowchart. Among 17 participating surgeons, each one performed three punctures on the phantom models: one RAG puncture, one USG puncture with needle guide attachment, and one USG without needle guide attachment. These procedures were performed on a single day to avoid the data collection bias. ANT-X = automated needle targeting with X-ray; RAG = robot-assisted fluoroscopy-guided; USG = ultrasound-guided.
The Characteristics of the Surgeons Who Performed Phantom Renal Accesses
Median [25%, 75% interquartile range].
For the USG puncture, we utilized a US machine (ARIETTA 70; Hitachi, Ltd., Tokyo, Japan) to view the target balls and perform needle access. The US machine was activated beforehand to avoid the potential bias for device preparation between the US and robotic device. Given that the participants had their own preference for using a needle guide attachment, each participant performed the USG puncture both with (Fig. 3A) and without (Fig. 3B) a needle guide attachment to standardize the US puncture skills. After examining the phantom skin using a US probe with a gel (device setup), the needle was inserted into the phantom model toward the target ball (needle puncture). The puncture location was confirmed by fluoroscopy.
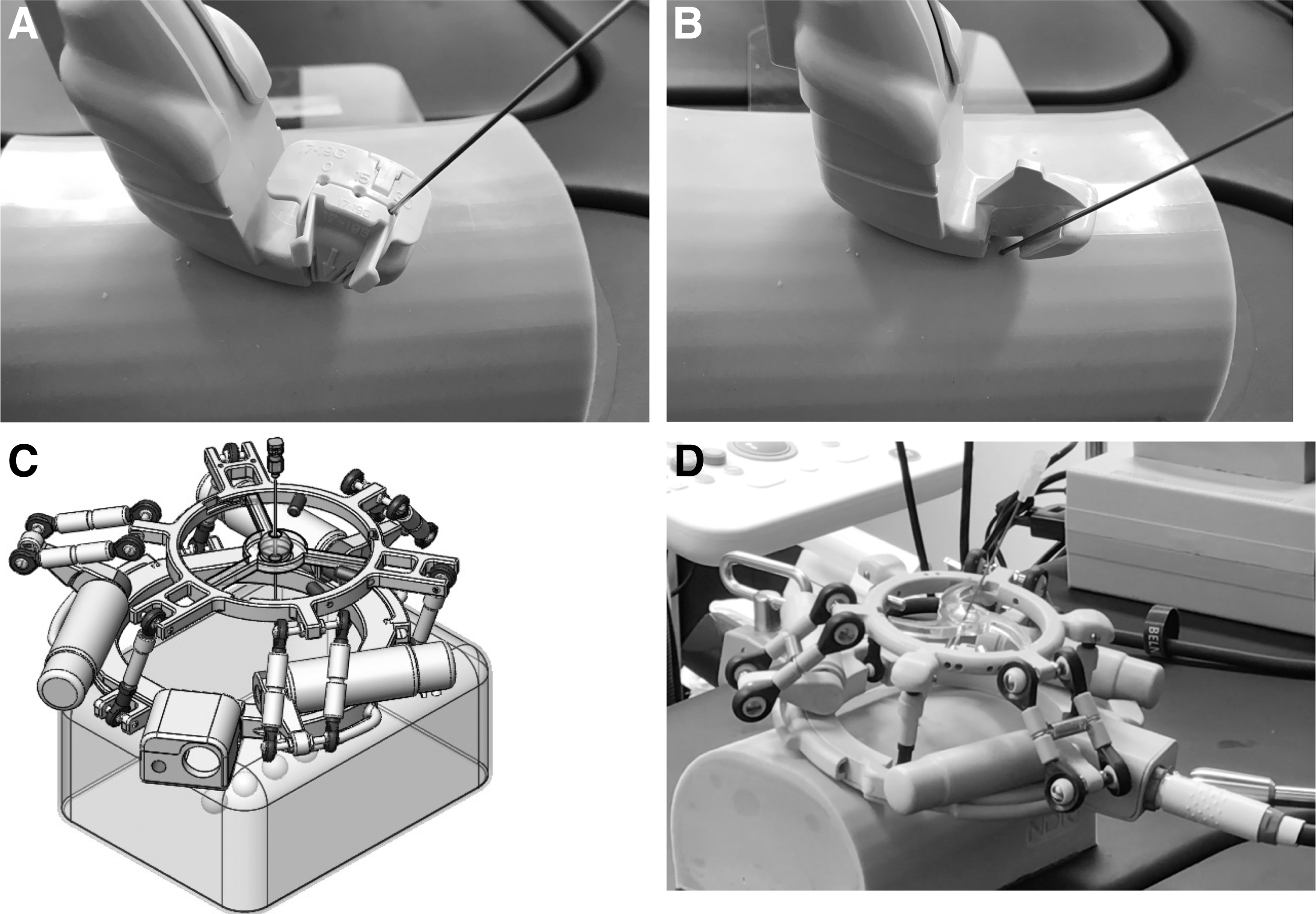
Representative photographs and images show the needle punctures into the phantoms with an ultrasound probe and a needle guide attachment
For RAG puncture, we utilized the ANT-X, 14 which integrated both an articulated reusable arm mounted on the operating table and a computer system connected to a standard C-arm for automated needle positioning to access the target balls mimicking renal stones (Fig. 3C, D). The ANT-X system is used for prone fluoroscopy-guided PCNL with bull's eye technique, 15 and its principles were described previously. 14 The software activation and robotic arm attachment to the operation table were completed beforehand. After the initial marking (Fig. 4A, B) on the phantom skin, computerized calibration (Fig. 4C) and alignment (Fig. 4D, E) were carried out to decide the needle insertion angle to the target (device setup). Then, the participant advanced the needle deep into the phantom model toward the target ball (Fig. 4F, G) (needle puncture). The puncture location was confirmed under fluoroscopic guidance by tilting the C-arm (Fig. 4H).
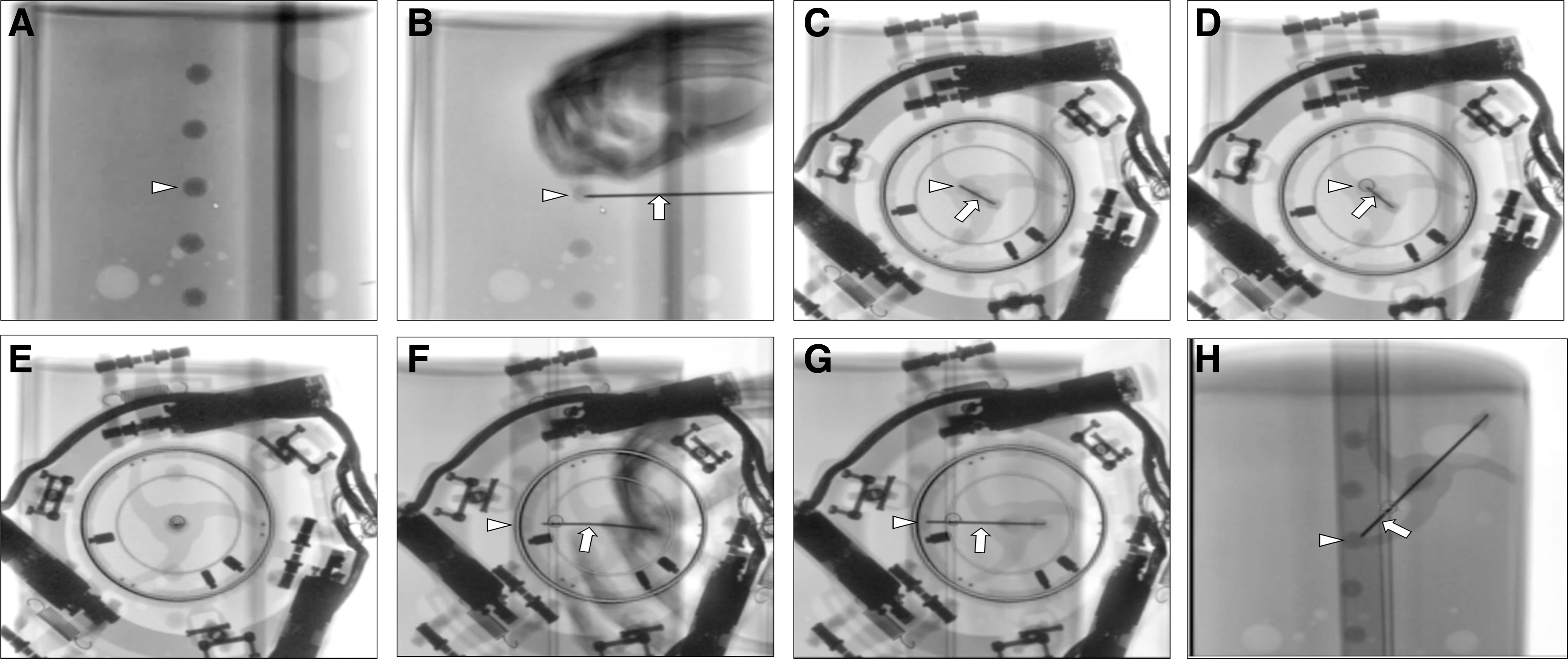
RAG puncture.
Statistical analysis
Continuous normally distributed variables were expressed as means (standard deviation), whereas non-normally distributed variables were expressed as medians (25%, 75% interquartile range). Categorical variables were presented as frequency (percentage). Two-sample t tests and Mann–Whitney U test were used to identify differences between groups. Categorical variables were compared using Fisher's exact test. Differences were considered statistically significant at α < 0.05. All statistical analyses were performed using EZR for R (R project) 16 by two authors (K.T. and R.A.), and then validated by the other authors.
Results
Among the participating doctors, 90% of the residents had <50 renal access experiences, such as PCNL and nephrostomy tube insertion, whereas all of the attending surgeons had an experience of >50 renal access cases. The median years of experience in urologic practice were 4.0 and 17.0 years for the residents and attending surgeons, respectively (Table 1).
A total of 34 US and 17 RAG punctures were performed during the study. Table 2 summarizes the comparison of the data between the access methods. The single puncture success rate of the RAG group was 100%, which was significantly higher than that of the USG group (p = 0.021). In the RAG group, the device setup time was 60 seconds longer, and the needle puncture time was 11 seconds shorter than that of the USG group (both p < 0.001); however, there was no significant difference in the total procedural time between the two groups. In addition, the duration of fluoroscopic exposure was much longer in the RAG group than in the USG group (6.5 and 38.0 seconds for US and RAG groups, respectively; p < 0.001). No significant differences in the other parameters were seen between the groups.
The Comparison of Feasibility of Renal Access on Phantom Models Between Ultrasound- and Robot-Assisted Fluoroscopy-Guided Punctures Performed by All Surgeons
It includes punctures performed both with and without a needle attachment guide.
Median [25%, 75% interquartile range].
Total procedural time includes both device setup time and needle puncture time.
The comparison of surgeon's self-assessment results between the two procedures is shown in Table 3. In the RAG group, the participating surgeons marked statistically higher scores for visibility (p = 0.002), safety (p = 0.013), and satisfaction (p = 0.001). In the RAG group, 41% of the participants reported excellent visibility, 60% completed the procedure without any trouble, and 82% were satisfied with the procedure. In the USG group, only 3% of the participants had excellent visibility, 15% completed the procedure without any trouble, and 26% were satisfied with the procedures and rated them as “never been better.”
The Comparison of Surgeon's Self-Assessment After Each Procedure Performed by All Surgeons
Details of each score are described as follows: visibility—5, excellent; 4, good; 3, reasonable; 2, poor; 1, hardly detectable.
Maneuverability—5, very smooth; 4, smooth; 3, fine; 2, somehow difficult; 1, very difficult.
Safety—5, without any trouble; 4, with a few confirmations; 3, fine; 2, with some troubles; 1, almost failed to complete because of troubles.
Satisfaction—5, excellent; 4, better than average; 3, average; 2, poor but no need to retry; 1, may need to retry
It includes punctures performed both with and without a needle attachment guide.
The subgroup analysis, comparing residents and attending surgeons in both RAG and USG groups, demonstrated that the only significant difference found between the groups was the median total procedural time, which showed that RAG puncture was performed within 131 and 104 seconds for the residents and attending surgeons, respectively (p = 0.045). The device setup time of RAG puncture was ∼30 seconds shorter in the attending surgeons than in the residents, but the difference was not statistically significant (p = 0.073). In addition, the median needle puncture time and total procedural time of USG puncture by the attending surgeons were 21 and 23 seconds shorter than those by the residents, but the differences were not statistically significant (Table 4).
The Comparison of Procedure Performance of Robot-Assisted Fluoroscopy- and Ultrasound-Guided Puncture Between Residents and Attending Surgeons
Median [25%, 75% interquartile range].
NA = not applicable.
Discussion
Our findings revealed that this latest robotic technique showed efficiency as an access method to the renal collecting system, comparable with the current USG puncture technique.
Robot-assisted procedures, represented by the Da Vinci® system, was first developed for prostatectomy and has made substantial revolution in clinical practice. 17 This technology has been adapted for kidney stone surgeries, such as robotic pyelolithotomy, nephrolithotomy, and anatrophic nephrolithotomy. There is also an interesting development of a robotic tool for ureteroscopy. 18 Roboflex™ has improved ergonomics for surgeon's maneuver. 19 Although these procedures utilize sophisticated technological tools, their outcomes are still based on the operator's experience and manual dexterity, which require long-term training.
To overcome these concerns, percutaneous access to the kidney (PAKY) and PAKY-remote control of motion were first introduced as an automated remote control access for the renal collecting system integrated with fluoroscopic vision, by the Johns Hopkins URobotics laboratory. 20 They further invented the AcuBot system, mounted on the computed tomography (CT) scan, to provide accurate puncture by monitoring scanned images with a remote needle driver as PAKY. 21 In addition, there is a development of other robot devices that are integrated with the magnetic resonance imaging (MRI) system for transperineal prostate percutaneous access, which is called MrBot robot. 22 The clinical application of MrBot has already been approved by the Food and Drug Administration because of its accuracy and safety for patients. Although these CT- and MRI-integrated navigation systems promote safe and accurate procedures, the renal access during PCNL is mainly performed under either fluoroscopic or US guidance rather than under CT or MRI guidance. Therefore, a more pragmatic methodology, using more accessible imaging modalities, for robot-assisted renal access is important to improve the technique for renal access for urinary stone disease. The present robotic system, ANT-X, is a feasible and effective tool owing to its ingenious features, such as compact size, ease of use, and completely automated navigation system. 14 Furthermore, it can tag onto existing low-cost C-arm fluoroscopic devices, which are found in most operating theaters.
Surprisingly, although all of the participating surgeons had not performed fluoroscopy-guided renal access, they were able to perform RAG puncture effectively, with an accuracy rate for reaching a target ball of 100% in a single puncture. The median needle puncture time, including the confirmation of location by fluoroscopy, was 24% faster in the RAG puncture, compared with the USG puncture. Most importantly, the surgeon's self-assessment for both procedures revealed that the RAG puncture had better visibility and increased safety than the USG puncture. They also reported that they are more satisfied with the RAG puncture. These are the advantages of RAG over USG punctures, which could lead to a safe and effective renal access during PCNL.
In addition, there was an interesting finding that the medial total procedural time of RAG puncture by the attending surgeons was nearly 30 seconds, ∼20% shorter than that by the residents. Even though both participants had no previous experience in fluoroscopy-guided renal access, surgeons with more experience and greater familiarity with the steps during puncture had shorter and smoother procedures with the ANT-X system. Despite these positive features, the RAG puncture had some disadvantages over the USG puncture. For instance, although the direct comparison was difficult because of the different device settings, the median device setup and fluoroscopic exposure times of RAG puncture were ∼1 minute and 60 seconds, respectively, longer than those of USG puncture. One reason for these results could be the fact that device setup was needed for fluoroscopic observation with ANT-X integration; thus, the fluoroscopic time was increased during the procedure. Furthermore, even though some useful techniques for fluoroscopy-guided PCNL have been reported in the literature, 15 the radiation time was quite high in our study, which may be because of the fact that the participating surgeons in this study were beginners of fluoroscopy-guided renal puncture and had little knowledge on the basic principles of as low as reasonably achievable (ALARA). 23 Training the surgeons for RAG puncture utilizing the ALARA protocol will reduce the procedural time and mitigate the radiation exposure time.
The main limitation of this study is that we utilized a phantom model mimicking the renal collecting system with some discrepancies in anatomy with an actual kidney. Given that this research is a benchtop ex vitro study, findings should be validated in stone patients and its economic impact should be evaluated in a clinical trial for future evaluations. In addition, the methodology for capturing the procedural time for both RAG and USG punctures may not be accurate and may be challenging for direct comparison. Similarly, the direct comparison between RAG and manual fluoroscopy-guided punctures might be useful to simply evaluate the differences between them. Lastly, although we utilized the surgeon's self-assessment for subjective evaluation of the procedures, a validated assessment questionnaire will be more reliable for the evaluation.
Conclusions
Our benchtop study comparing the efficacy between RAG and USG phantom punctures revealed comparable results for mimicked renal access during PCNL. The single puncture success rate for RAG is also significant. The fluoroscopy-guided access under the ANT-X system allowed for safer and more accurate target puncture even for beginners. Although the basic principles to mitigate radiation exposure such as the ALARA protocol are needed, for fluoroscopy-guided procedures, we believe that the RAG puncture technique with the ANT-X system could improve the procedural success rate and duration to facilitate surgeons' work on PCNL, affecting the clinical practice.
Footnotes
Acknowledgments
We thank the radiology staff and the following participating doctors of NCU Hospital: Masahiko Isogai, Kenichi Hasebe, Tomoki Okada, Kengo Kawase, Yuya Ota, Tomoki Takeda, Satoshi Nozaki, and Yasuhiro Fujii. NDR Medical Technology provided the ANT-X device and phantom models used in this study without any further financial support.
Author Disclosure Statement
Y.-K.T. serves as a medical adviser to NDR Medical Technology.
Funding Information
No funding was received for this article.