
Abstract
Purpose:
To compare the efficacy of a newly developed hybrid pencil-type energy device (HD) generating simultaneously monopolar high-frequency electric energy and ultrasonic energy with that of a conventional device (CD) during laparoscopic partial nephrectomy (LPN).
Materials and Methods:
A total of 16 female pigs (32 kidneys) were divided into 4 groups of 4 animals (8 kidneys) each: nonischemic and ischemic HD-LPN groups, and nonischemic and ischemic CD-LPN groups. We performed bilateral LPN for each pig. HD alone was used in the HD-LPN group, whereas commercially available monopolar scissors and a soft coagulation system were used in the CD-LPN group. After observing the postoperative course for 14 days, we euthanized the animals and harvested the kidneys for histopathological observations.
Results:
We completed an LPN on a total of 32 kidneys. There were no cases of conversion to open surgery, nor were there any deaths or complications requiring treatment. For nonischemic LPN, LPN time was significantly shorter in the HD-LPN group than in the CD-LPN group (11.4 ± 4.8 vs 17.7 ± 5.3 minutes, p = 0.027). The decrease in postoperative hemoglobin was equally low in both groups. However, the frequency of TachoSil® use was significantly higher in the CD-LPN group than in the HD-LPN group (6/8 [75%] vs 0/8 [0%], p = 0.007). For ischemic LPN, we found no significant differences in parameters such as LPN time and using TachoSil between the two groups. The depth of thermal injury was the most superficial in the nonischemic HD-LPN group in comparison with the other three groups.
Conclusions:
The application of an HD allowed nonischemic LPN to be performed safely in a short time with less blood loss and less thermal injury to the kidney in the porcine model. Additional clinical investigations of human kidneys are required.
Introduction
Instead of radical nephrectomy, partial nephrectomy allowing the preservation of renal function has become the standard surgical technique for early-stage renal cancer without metastasis. 1 Laparoscopic partial nephrectomy (LPN) is gaining wide acceptance as a minimally invasive procedure, thus replacing open partial nephrectomy as the gold standard. However, laparoscopic surgery poses technical challenges, because it requires tumor excision, control of bleeding, and suturing as well as reconstruction of the opened urinary tract through small incisions within the abdominal cavity. In general, LPN is often performed under ischemia by clamping the renal vessels to secure a good surgical field. However, prolonged ischemia times can lead to irreversible renal dysfunction. Therefore, various procedures such as surgical techniques that do not include ischemia have been investigated by using animal experiments 2 –8 and patients with renal tumors in clinical settings. 9,10
In this study involving a porcine model, we used a newly developed hybrid pencil-type energy device (HD; Olympus Corporation, Tokyo, Japan) 11 to perform LPN. We compared the outcomes of LPN with an HD (HD-LPN) with those of LPN with a commercially available conventional device (CD-LPN) and assessed the usefulness of HD for nonischemic LPN without clamping the renal vessels.
Materials and Methods
The energy device used in this study was an HD that involved simultaneously generated monopolar high-frequency electric energy and ultrasonic energy for laparoscopic surgery developed by Olympus Corporation. The length of the device itself is 350 mm, and the diameter of the shaft is 5 mm, with a tip in the shape of a spatula (Fig. 1). High-frequency electric energy is generated with a power of 40 W in the coagulation mode and at a maximum voltage of 1600 Vp. Ultrasonic energy is generated at a frequency of 47 kHz and an amplitude of 70 μmpp. Switch-on generates high-frequency electric energy and ultrasonic energy simultaneously, allowing resection and coagulation/hemostasis.
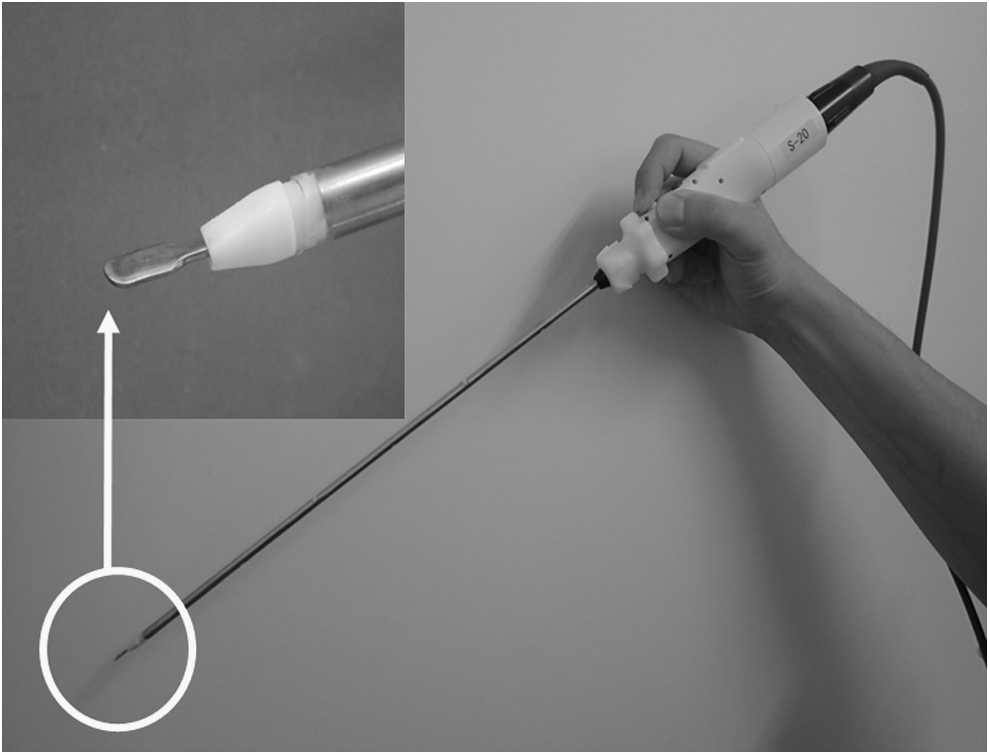
A hybrid pencil-type energy device developed by Olympus Corporation (Tokyo, Japan) generating simultaneous monopolar high-frequency electric energy and ultrasonic energy. The tip has a spatula shape.
Animal experiment and surgical methods
We used 16 female pigs (weight range: 45.2–52.6 kg; average weight: 48.5 kg) as experimental animals. They were divided into four groups: nonischemic HD-LPN, ischemic HD-LPN, nonischemic CD-LPN, and ischemic CD-LPN, with each group having four pigs (eight kidneys). This protocol for the animal experiment was approved by the animal experimentation ethics committee of Shin Nippon Biochemical Laboratory, Ltd. (Kagoshima, Japan; Approval No.: 149P-081/150P-081), which is certified by the Association for Assessment and Accreditation of Laboratory Animal Care International.
LPN was performed by four fully experienced urologists certified by the Laparoscopic Surgical Skill Qualification System of the Japanese Society of Endourology. LPN of both kidneys was performed for each pig in each group. The resection range of the renal parenchyma was set to a circle measuring ∼25 mm in diameter and ∼5 mm in thickness. In two LPN groups using an HD, the HD alone was used to resect the renal parenchyma and for coagulation/hemostasis. In two LPN groups using a CD, we used commercially available monopolar scissors (Epix® scissors, 40 W, Effect 2; Applied Medical, Rancho Santa Margarita, CA) to resect the renal parenchyma; a soft coagulation electrode (HiQ+ soft coagulation/suction/irrigation system, 65 W, Effect 3; Olympus) was used for coagulation/hemostasis. A fibrin sealant patch (TachoSil®; CSL Behring, Tokyo, Japan) was used if intraoperative bleeding was deemed difficult to control in any of the four groups.
LPN of the right kidney was first performed in the left lateral position with tracheal intubation under general anesthesia. Laparoscopic surgery began with four trocars. In the groups using an HD, the posterior peritoneum and renal fascia were resected and detached by using an HD to expose the anterior surface of the kidney. Markings were made around the fabric marker by using an HD at a point close to the center of the anterior surface of the kidney to determine the resection range of the renal parenchyma (i.e., the round area ∼25 mm in diameter; Fig. 2A). Resection of the renal parenchyma began without clamping the renal vessels in the nonischemic HD-LPN group. The resection depth of the renal parenchyma was set to ∼5 mm to avoid damaging and opening of the urinary collecting system (∼5 mm in the shaft diameter of each forceps was considered for the targeted resection depth of the renal parenchyma; Fig. 2B). We resected the renal parenchyma along the marker while slightly lifting up the resected renal tissue by using a blunt-tip suction/irrigation tube held with the left hand, to confirm the resection surface (Fig. 2C). After freeing the resected tissue completely, we used an HD to control bleeding from the resected bed and surgical margin of the kidney (Fig. 2D). After confirming hemostasis, we removed the four trocars and closed the wounds. We then repositioned the body in the right lateral position and performed LPN of the left kidney in a manner similar to that for the right kidney. In the ischemic HD-LPN group, we dissected the renal vessels and clamped them with Bulldog forceps. Then, we performed LPN in a manner similar to the procedure for the nonischemic HD-LPN group. After hemostasis, the clamp was removed to induce renal reperfusion.
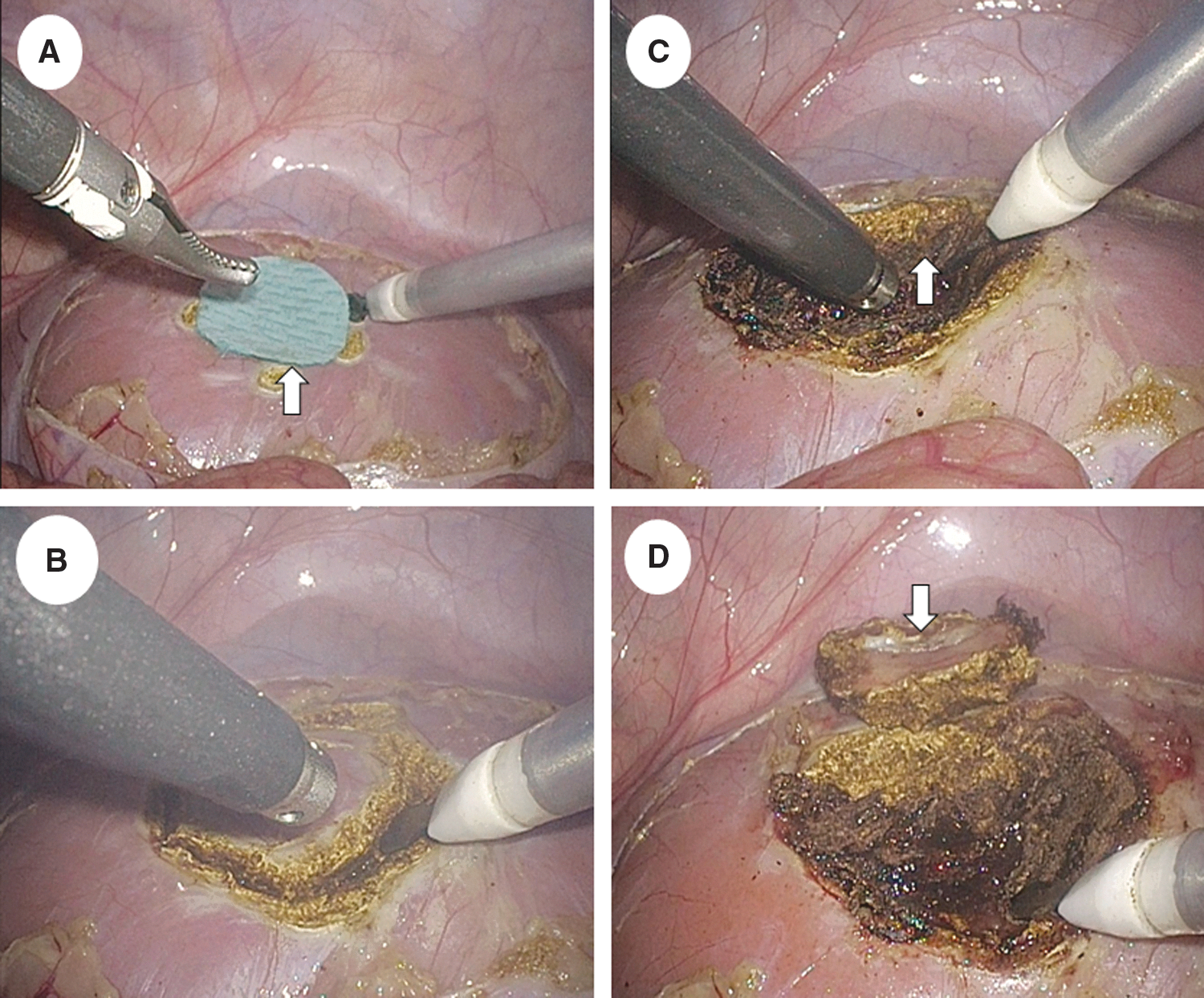
Nonischemic laparoscopic partial nephrectomy with an HD.
In the CD-LPN group, we used monopolar scissors to resect the renal parenchyma and a soft coagulation electrode for hemostasis of the resected bed and surgical margin after finishing renal parenchyma resection. In addition, we used a bipolar coagulation forceps (HiQ + Bipolar, 40 W; Olympus) as a secondary device. Other surgical techniques used for the CD-LPN group were similar to those used for the HD-LPN group.
Outcome measures
Outcome measures included total surgical time (from the start of resection of the posterior peritoneum to completion of LPN) and LPN time (from the start of resection of the renal parenchyma to completion of hemostasis at the resected site). Other outcome measures were intraoperative blood loss, frequency of TachoSil use, number of conversions to open surgery, and number and severity of perioperative complications. We performed blood tests at six time points (immediately before and after surgery and on postoperative days 1, 3, 7, and 14). We performed contrast-enhanced CT (CECT) during the 1 week leading up to surgery and at 3 and 14 days after surgery.
The pigs were euthanized at 14 days after surgery, and both kidneys were harvested. The tissue was formalin-fixed after macroscopic observations of kidney specimens. Next, we divided the center of the partially resected site in the transverse direction and prepared specimens stained with hematoxylin and eosin (H&E) to histopathologically examine the effects of thermal injury on renal tissue. A veterinarian pathologist observed H&E-stained specimens by using a light microscope to determine the range of thermal injury in the renal tissue and measured the depth from the surface vertically in the necrotic area of the renal tissue at 10 sites at near-equal intervals for each kidney specimen. The average of 10 depth measurements was established as the depth of thermal injury.
Statistical analysis
For statistical analyses, we used IBM SPSS version 21 software package (IBM Corp., Armonk, NY) and performed a normality test, an F-test, Fisher's exact test, Student's t-test, Aspin–Welch's t-test, and Mann–Whitney's U-test; p < 0.05 was considered statistically significant.
Results
Table 1 shows perioperative outcomes of the four experimental groups. We completed LPN for a total of 32 kidneys in all four groups. There were no cases of conversion to open surgery. There were no major complications, including deaths, urine leakage, hematoma, and intra-abdominal abscess, during surgery or during the observation period.
Perioperative Outcomes of the Four Experimental Groups
Data displayed as mean ± standard deviation or n (%).
CD = conventional device; Cr = creatinine; Hb = hemoglobin; HD = hybrid pencil-type energy device; LPN = laparoscopic partial nephrectomy.
Nonischemic LPN
For nonischemic LPN, total surgical time was significantly shorter in the HD-LPN group than in the CD-LPN group (15.4 ± 5.4 vs 23.7 ± 4.6 minutes, p = 0.005). LPN time was also significantly shorter in the HD-LPN group than in the CD-LPN group (11.4 ± 4.8 vs 17.7 ± 5.3 minutes, p = 0.027). The decrease in immediate postoperative hemoglobin (Hb) levels was slight in both groups, indicating no significant differences (0.30 ± 0.22 vs 0.33 ± 0.25 g/dL, p = 0.885). However, the frequency of TachoSil use was significantly higher in the CD-LPN group than in the HD-LPN group (6/8 [75%] vs 0/8 [0%], p = 0.007), suggesting that bleeding control was better in the HD-LPN group than in the CD-LPN group. Changes in serum creatinine (Cr) levels on postoperative day 14 were slight in these groups (−0.06 ± 0.1 vs −0.01 ± 0.1 mg/dL, p = 0.426). Other blood test findings on postoperative day 14 were unremarkable.
Figure 3A and B, respectively, show typical CECT findings obtained on postoperative day 14 from the HD-LPN and the CD-LPN groups. In the HD-LPN group, although a small low-density area corresponding to the partially resected site was observed, no sites measuring 20 mm or larger in maximum diameter were detected. In contrast, in the CD-LPN group, we observed cyst-like low-density areas measuring 20 mm or larger in maximum diameter in four kidneys. Neither urinoma nor hematoma was detected in either group.

CECT findings at 14 days after surgery and hematoxylin and eosin-stained histopathological specimen of the resected kidney.
Ischemic LPN
For ischemic LPN, total surgical time, LPN time, decrease in Hb levels immediately after surgery, frequency of TachoSil use, and changes in serum Cr levels on postoperative day 14 did not differ significantly between the HD-LPN and CD-LPN groups. We observed no abnormalities in other blood tests of the two groups on postoperative day 14. Based on the CECT findings on postoperative day 14, the number of kidneys with a cystic lesion was one and six in the HD-LPN and CD-LPN groups, respectively. Neither urinoma nor hematoma was detected in either group.
Depth of thermal injury
Figure 3C and D, respectively, show typical histopathological findings for the nonischemic HD-LPN group and ischemic CD-LPN group. The depth of thermal injury was shallow in the nonischemic HD-LPN group, but it was deep in the ischemic CD-LPN group.
The mean depths of thermal injury were 2.09 ± 0.29, 2.82 ± 1.34, 3.86 ± 0.87, and 6.99 ± 1.54 mm in the nonischemic HD-LPN, nonischemic CD-LPN, ischemic HD-LPN, and ischemic CD-LPN groups, respectively (Fig. 4). The nonischemic HD-LPN group showed a significantly more shallow depth of thermal injury compared with the ischemic HD-LPN and ischemic CD-LPN groups (p < 0.001 vs ischemic HD-LPN and p < 0.001 vs ischemic CD-LPN). The depth of thermal injury was also more shallow in the nonischemic HD-LPN group than in the nonischemic CD-LPN group, although this did not reach statistical significance (p = 0.173). Moreover, the depth of thermal injury was significantly more shallow in the ischemic HD-LPN group than in the ischemic CD-LPN group (p = 0.000).
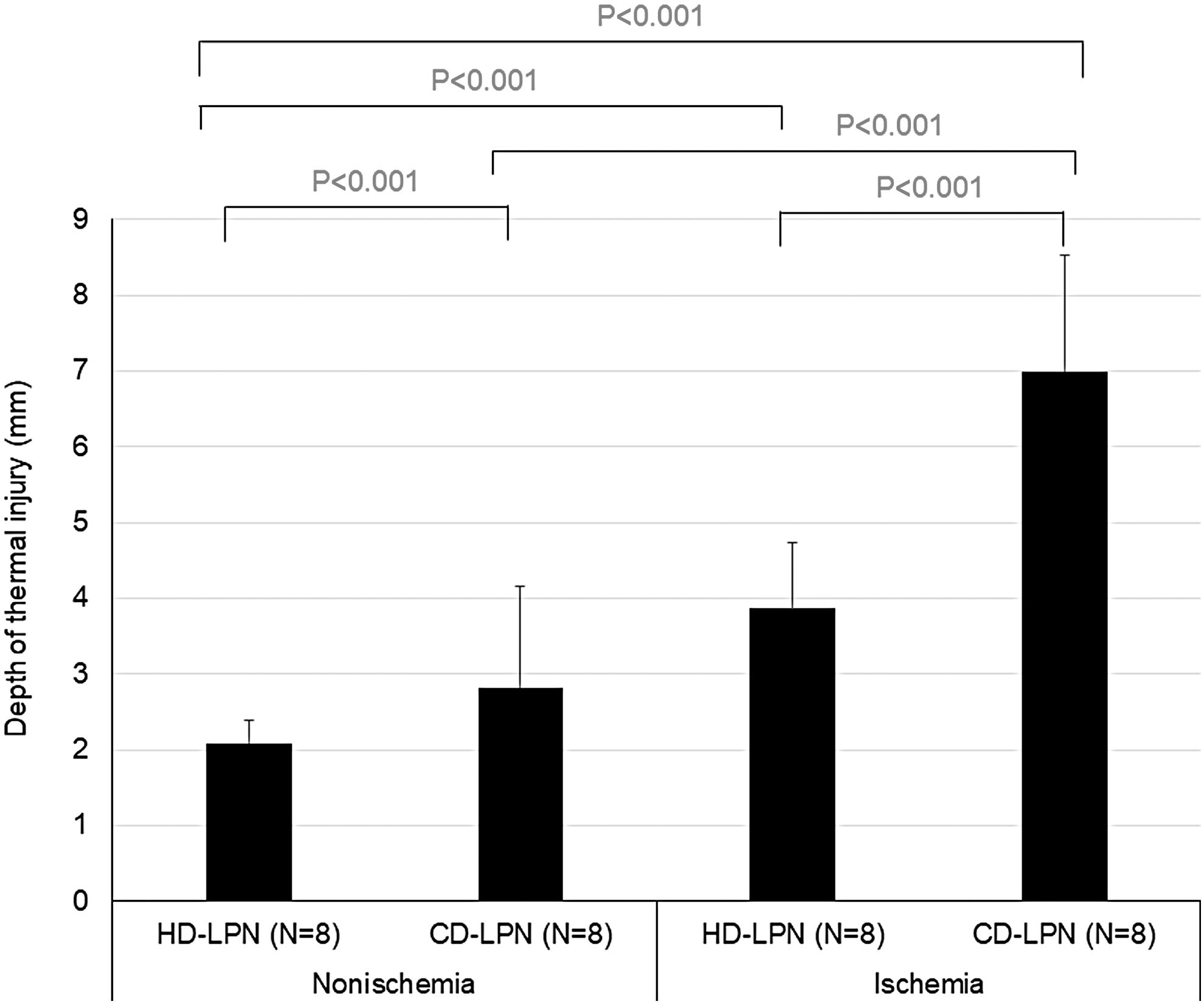
Comparison of the thermal injury depth among eight kidneys of four groups (four animals each). The depth of thermal injury was more shallow with HD-LPN than with CD-LPN, whether ischemia was present or absent. The thermal injury was significantly more shallow with nonischemic LPN than with ischemic LPN, regardless of device type. Data are mean ± standard deviation.
Discussion
An ideal energy device for LPN would allow simultaneous resection of the renal parenchyma and coagulation/hemostasis. In addition, tissue necrosis associated with thermal injury must be minimized at deep-seated sites and across a wide range of the remnant kidney. Various devices such as a thulium laser, 2 radiofrequency, 3,4 potassium-titanyl-phosphate laser, 5,7 bipolar cautery (LigaSure), 5 ultrasonic cutting and coagulation device (SonoSurg), 5 hydrodissection, and holmium:YAG laser 8 have been investigated in an animal kidney model to evaluate nonischemic LPN. The potential use of these devices has also been assessed in actual clinical settings.
The advantages of the HD used in this study are as follows: The addition of ultrasonic vibration (frequency, 47 kHz; amplitude, 70 μmpp) to a monopolar device reduces tissue sticking compared with conventional monopolar high-frequency electric energy devices, thereby shortening the resection time; because this allows coagulation at low temperatures (electric power, 40 W, coagulation mode), the generation of Joule heat is inhibited and damage due to thermal injury is minimized.
The results of this study showed that LPN with an HD, regardless of the presence or absence of ischemia, can be performed safely and quickly with minimal blood loss. Notably, when nonischemic LPN was performed, total surgical time and LPN time were significantly shorter in the HD-LPN group than in the CD-LPN group used as a control. A possible explanation for the significantly short LPN time in the HD-LPN group is that HD is better for resecting the renal parenchyma and blood coagulation. The nonischemic HD-LPN group had no bleeding cases that were difficult to control. Moreover, because single-device HD is capable of resecting the renal parenchyma and coagulation, there is no need to replace it with another surgical instrument through the trocar port, allowing completion of LPN in less time. In the nonischemic CD-LPN group, although monopolar scissors promoted the resection of the renal parenchyma in a relatively short time, bleeding was difficult to control with soft coagulation used for coagulation/hemostasis and required prolonged hemostasis. TachoSil was required in 75% of the bleeding cases that were difficult to control. Separate surgical instruments for the resection of the renal parenchyma and coagulation/hemostasis and time-consuming changes of instruments through the trocar port were used for the CD-LPN group.
Nonischemic LPN was significantly associated with more shallow depths compared with ischemic LPN in the HD-LPN and CD-LPN groups. Such shallow depths obtained with nonischemia LPN were consistent with those reported by Mues et al., who used a new wet monopolar device in a porcine kidney model. 12 Therefore, it was concluded that more shallow thermal injuries were obtained in the absence of ischemia compared with those obtained in the presence of ischemia for LPN, regardless of device type. The thermal injury depth in nonischemic or ischemic LPN was lesser in the HD group than in the CD group. We believe that the reason for the more shallow thermal injury in the HD group was the shorter coagulation time due to good hemostatic ability of HD. Moreover, we suspect that tissue injury by HD is more shallow than that by soft coagulation of CD even if the coagulation time is similar, because the ischemic LPN-HD group showed significantly more shallow thermal injury than the ischemic LPN-CD group, regardless of almost the same time needed for LPN in both groups. Another report indicated that thermal injury of liver tissue associated with HD use was equivalent to that associated with the use of a monopolar device and ultrasonic device in a porcine model. 13
This study had several limitations. First, the number of animals (four in each group) was small. However, we performed LPN for both kidneys in each pig. Therefore, LPN was performed eight times in each group. Second, although the porcine model closely matches to humans, the porcine kidney is smaller than and not as well vascularized as the human kidney. 12 Therefore, the results obtained in the present porcine model cannot be translated to those for the human kidney. Third, due to the shallow resected depth of the renal parenchyma when using an HD in this study, we were unable to assess the ability to respond to bleeding from a large vessel and the renal calix damage anticipated to occur if renal dissection reaches the renal medulla. If bleeding from a large vessel or renal calix damage occurs, then a suturing procedure or other subsidiary materials such as TachoSil may be required. Another limitation was that it was not determined whether it was easy to close the caliceal wall injured by HD.
Conclusions
The application of an HD allowed nonischemic LPN to be performed safely in a short time with less blood loss and less thermal injury to the kidney in the porcine model. Additional clinical investigations of human kidneys are required.
Footnotes
Acknowledgment
The authors thank the veterinary pathologist (Olympus Corporation, Tokyo, Japan) for performing the histopathological assessments.
Author Disclosure Statement
This study was funded by Olympus Corporation.
Funding Information
This study was funded by the device manufacturer (Olympus Corporation, Tokyo, Japan), and the investigating surgeons received an honorarium for their time. The company did not contribute to the writing of the article.