
Abstract
Introduction and Objectives:
Ureteroscopic management of impacted ureteral stones poses multiple challenges. We examined whether ureteral thickness measured on preoperative noncontrast computed tomography (CT) is predictive of stone impaction at the time of ureteroscopy (URS).
Methods:
Thirty-eight patients with preoperative CT scan and undergoing URS for ureteral stones were prospectively studied. Ureteral thickness directly above, around (peri-calculus ureteral thickness [P-CUT]), and below the calculus were determined on CT scan. The cross-sectional surface area around the stone (P-CUT) was also calculated. Stones were considered impacted at surgery if contrast had difficulty passing, a guidewire could not pass, and the stone was visually impacted >5 on a Likert scale. The surgeon determining intraoperative impaction and the individual measuring the ureteral thickness on CT were blinded.
Results:
Fourteen of the 38 patients were found to have an impacted ureteral stone at the time of surgery. Patients with an intraoperative finding of an impacted stone had significantly higher ureteral thickness above, around (P-CUT), below the calculus, and P-CUT surface area with all four p-values <0.001. P-CUT surface area was independently predictive of impaction at the time of surgery on multivariate analysis. A mean P-CUT of 6.1 and 1.6 mm and P-CUT surface area of 92.6 and 15.4 mm2 were noted for the impacted and nonimpacted stones, respectively.
Conclusion:
Ureteral thicknesses above, around (P-CUT), and below the calculus are readily measurable on CT scan. P-CUT surface area can also be calculated for a stronger representation of ureteral thickness. These four parameters are predictive of ureteral stone impaction and useful for surgical planning and patient counseling.
Introduction
Impacted ureteral stones can be associated with edema and hypertrophy of the ureteral mucosa making endoscopic retrograde ureteral surgery more challenging. 1,2 Potential complications of ureteroscopy (URS) for impacted ureteral stones include greater adherence of stone fragments to the adjacent ureteral mucosa that can lead to subsequent bleeding, possible ureteral perforation, and future ureteral stricture. 3,4
The ability to predict ureteral stone impaction from preoperative imaging could be advantageous in several ways. First, a urologist would be able to counsel a patient about realistic expectations of stone clearance, increased possibility for initial stenting with future definitive stone treatment, or the increased likelihood for stenting following URS. Second, a general urologist may refer these patients to a stone specialist given the higher complexity of successful stone treatment. Third, a urologist could optimize preoperative variables such as the use of preoperative alpha-blockade and withholding anticoagulation to allow for easier access and visualization of the stone during the case. Fourth, for large proximal ureteral impacted stones, an endourologist may have a lower threshold to perform percutaneous assisted antegrade URS instead of retrograde URS. 5,6 Also, retrospective studies have shown that an impacted stone has less of chance spontaneous passage compared to a nonimpacted stone, which would make medical expulsive therapy a less appealing option. 7
Due to the value this information may provide to a urologist's practice, many researchers have attempted to delineate predictive factors that would preoperatively indicate ureteral stone impaction. Several retrospective investigations have reported factors including, increased peri-ureteral density, increased ureteral lumen density distal to the stone, increased serum creatinine, increased severity of hydronephrosis, and increased ureteral wall-thickness to be associated with stone impaction. 8 –13 However, no such studies have utilized a prospective study paradigm to identify the predictive value of each parameter.
In this prospective study, we compared ureteral thickness parameters, as measured on computed tomography (CT) imaging of patients with and without impacted ureteral stones to identify factors that may predict ureteral impaction.
Materials and Methods
We obtained institutional board approval for this double-blind, prospective study for patients undergoing URS for ureteral stones who had preoperative noncontrast CT imaging. Patients were recruited and followed up between August 2017 and January 2019. A single surgeon was responsible for the surgical treatment of study participants. Before surgery, a separate surgeon blinded to future intraoperative findings evaluated the preoperative noncontrast CT. Measurements of stone size, ureteral thickness on a coronal series directly above, around, and below the calculus were made. The measurement of ureteral thickness around the stone was termed the peri-calculus ureteral thickness (P-CUT).
To reliably measure these ureteral thickness parameters, the CT coronal images at 4 × magnification were used. Coronal images were used because the entire stone is visible on a coronal longitudinal profile, allowing the physician to visualize and accurately measure P-CUT at the widest part of the stone. The ureteral thickness above and below the stone was taken just superior and inferior to the terminal edges of the stone, respectively. To measure P-CUT, the widest transverse dimension of the ureter involving the stone and corresponding transverse dimension of the stone at this level were measured. P-CUT was then calculated by subtracting the stone width from the overall stone and ureteral width (Figs. 1 and 2). The rationale for using this measurement technique for P-CUT was because the ureteral thickness was often asymmetrical around the stone. This measurement was then converted to surface area to have a better three-dimensional representation of the stone and the adjacent ureteral wall. For simplicity of measurement, ureteral and stone diameters were used to calculate cross-sectional surface area (Appendix A1). To calculate the P-CUT surface area, the cross-sectional surface area of the stone was subtracted from the cross-sectional surface area of the ureter and stone combined, outlined in the following formula: P-CUT surface area = π/4 (d 1 2 − d2 2) (Appendix A1).
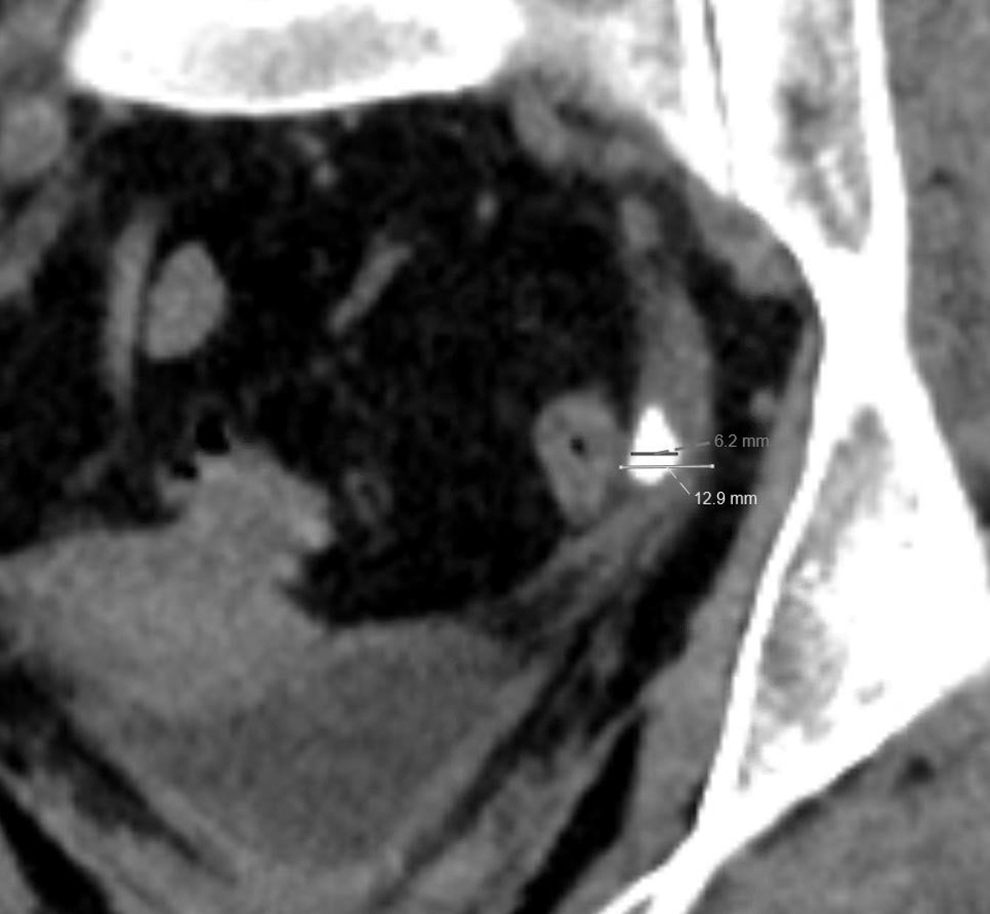
Coronal image of an impacted distal ureteral calculus. The stone width (6.2 mm) is subtracted from the overall ureteral width (12.9 mm) at this same level to get the P-CUT (6.7 mm). Note the asymmetry of edema, which is mostly observed lateral to the ureteral calculus. P-CUT = peri-calculus ureteral thickness.
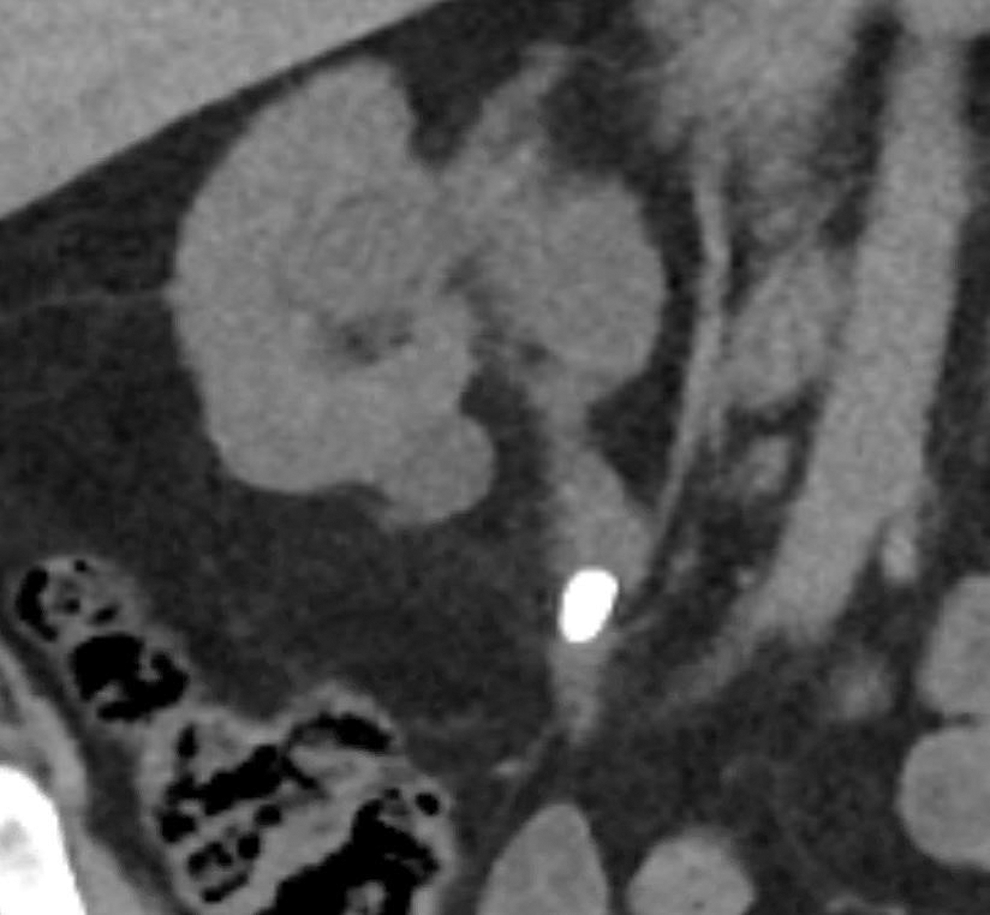
Coronal image of a nonimpacted proximal ureteral calculus with a ureteral stone width of 7.1 mm, stone width of 8 mm, and a P-CUT of 0.9 mm.
At the time of the surgery, a surgeon blinded to the CT measurements of ureteral thickness determined whether or not a stone was impacted based on intraoperative findings. The operating surgeon was able to review the CT images before surgery, but did not measure the ureteral wall. Stone impaction was determined by the surgeon using a 10-point Likert scale. Our 10-point Likert scale assesses stone impaction based on four categories: (1) Stone mobility, (2) Level of edema, (3) Guidewire passage, and (4) Contrast passage. Calculi were considered as nonimpacted if rated between 1 (mobile/rolling stone, no edema, guidewire and contrast pass freely) and 5 (stone stuck in ureter, requires mild pressure with ureteroscope or irrigation to dislodge, mild to moderate edema in contact with stone, guidewire passage requires mild to moderate pressure, 60% of contrast able to pass). Calculi rated between 6 (stone stuck in ureter, requires moderate pressure with ureteroscope or irrigation to dislodge stone, moderate edema in contact with stone, guidewire passage requires moderate pressure, 50% of contrast able to pass) and 10 (stone embedded within ureteral tissue and tissue stuck to stone and requires in situ treatment, severe edema, guidewire unable to pass, <10% of contrast able to pass) were considered impacted.
Demographic data, CT imaging parameters, and intraoperative factors were used for comparison between the impacted and nonimpacted stone groups. Statistical analysis was performed using t-tests and logistic regression with SPSS statistical software v.25 (IBM Analytics, Armonk, NY). Any univariate result with a p-value ≤0.05 was included within a multivariate regression model to investigate independent predictors of stone impaction. This includes ureteral thickness above the stone, P-CUT, P-CUT surface area, and ureteral thickness below the stone.
Results
A total of 38 patients were included in the study. Patients with ureteropelvic junction and ureterovesical junction stones were excluded from the study because of the inability to reliably measure ureteral width immediately above and below the stone, respectively. The mean time between initial presentation and day of surgery was 14.5 days for the control group and 24 days for impacted group. The mean duration between CT scan and extraction procedure was 25 and 25.6 days for the control and impacted groups, respectively. No significant difference between groups was noted for either temporal measure. No differences in age, height, weight, body mass index, or American Society of Anesthesiologists (ASA) score status were observed between the two groups (Table 1). Additionally, no differences in preoperative hydronephrosis, stone location, and stone size were observed between groups (Table 2).
Clinical Characteristics of Study Patients
Standard deviation of mean values in parentheses.
ANOVA.
Chi-square.
ANOVA = analysis of variance; ASA = American Society of Anesthesiologists score; BMI = body mass index.
Stone Characteristics and Degree of Hydronephrosis of Study Patients
Standard deviation of mean values in parentheses.
Chi-square.
ANOVA.
Of the 38 patients, 14 were found to have an impacted ureteral stone at the time of surgery based on Likert scale criteria. Patients with an intraoperative finding of an impacted stone had statistically significant higher ureteral thickness above, around (P-CUT), below the calculus, and P-CUT surface area with all four p-values <0.001 (Table 3). Multivariate analysis revealed that P-CUT surface area was independently predictive of impaction at the time of surgery (p-value 0.025, Table 3). A mean P-CUT of 6.1 and 1.6 mm and P-CUT surface area of 92.6 and 15.4 mm2 were determined for the impacted and nonimpacted stone groups, respectively. The differences in the mean stone volumes of 221.8 and 99.2 mm3 for impacted and nonimpacted stone groups, respectively, were not found to be statistically significant (p-value 0.86, Table 3).
Ureteral Thickness Parameters of Study Patients
Standard deviation of mean values in parentheses.
ANOVA.
Multivariate analysis.
Denotes significance.
P-CUT = peri-calculus ureteral thickness.
Discussion
Treatment of impacted ureteral calculi can be challenging because of ureteral edema and hypertrophy. 1,2 This may result in greater adherence of stone fragments to the adjacent ureteral mucosa that can lead to subsequent bleeding, possible ureteral perforation, and future ureteral stricture. 3,4 A Clinical Research Office of the Endourological Society (CROES) database report of 2650 patients undergoing ureteroscopic treatment of impacted stones demonstrated lower stone-free rates and higher rates of bleeding, ureteral avulsion, and ureteral perforation. 8
In our study, patients with an intraoperative finding of an impacted stone had significantly higher ureteral thickness above, around (P-CUT), below the calculus, and P-CUT surface area with all four p-values <0.001 (Table 3) on univariate analysis. Additionally, P-CUT surface area was independently predictive of impaction at the time of surgery on multivariate analysis (Table 3). A mean P-CUT of 6.1 and 1.6 mm and P-CUT surface area of 92.6 and 15.4 mm2 were noted for the impacted and nonimpacted stone groups, respectively. As such, a urologist should have a high degree of suspicion for an impacted ureteral stone with a P-CUT and P-CUT surface area of 6 mm and 90 mm2, respectively. While there was an observed difference in stone volume, there was high standard deviation within the cohort. If there were more patients included in the study, we may eventually see significance. P-CUT is a better measure to predict stone impaction because we see significance at such a low number of patients.
Although P-CUT, also referred to as ureteral wall thickness in previous retrospective studies, 8,10,11 is a promising technique to predict stone impaction, several additional preoperative indicators should be mentioned. In a study conducted by Tran et al., the researchers found that on a noncontrast CT scan, patients in the impacted stone group had significantly higher ureteral lumen density below the stone. 12 Also, severity of hydronephrosis, and increased serum creatinine were also found to be characteristic of patients with impacted ureteral stones. 9,11 While these studies followed a retrospective paradigm and should be validated among a larger patient sample they illustrate a promising trend toward preoperatively predicting whether a ureteral stone is impacted.
In accordance with previous work on this topic, our study suggests that a urologist has the ability to predict ureteral stone impaction from the measurement of ureteral thickness parameters on a noncontrast CT before surgery. This gives the urologist the opportunity to counsel a patient with an impacted ureteral stone appropriately for expected outcomes of URS. These include a much higher likelihood of a staged procedure with prestenting and subsequent definitive stone treatment. Additionally, patients can expect a higher likelihood of postoperative stenting. A urologist may utilize other strategies such as the use of preoperative alpha-blockers to facilitate retrograde URS and withholding anticoagulation to reduce risk of bleeding and a better chance of successful stone treatment. An endourologist may also have a lower threshold to perform percutaneous antegrade URS for larger, proximal ureteral calculi rather than retrograde URS. Finally, a urologist would be less likely to recommend a trial of medical expulsive therapy for impacted ureteral stones given the less likelihood of spontaneous passage. 7
Our study is the first prospective, double blind study evaluating ureteral thickness, as measured on preoperative CT scan, to predict intraoperative ureteral stone impaction. Calculating P-CUT is fairly simple, and it can be easily implemented to guide both the provider and patient in making clinical decisions. A limitation of our study is the exclusion of patients with either ureteropelvic junction or ureterovesical junction calculi because of the inability to measure ureteral thickness parameters reliably at these anatomical locations. An additional limitation to this study is the limited size of our study cohort. Further investigations regarding this topic should aim to first validate previous findings using larger samples, and second, combining known predictive factors into a comprehensive nomogram that will provide urologists with an accurate estimation of whether a patient's ureteral stone is impacted.
Conclusion
A urologist with the ability to measure stone size on CT coronal imaging can readily determine ureteral thicknesses above, around (P-CUT), and below the calculus. P-CUT surface area may also be calculated for a stronger representation of ureteral thickness. These four parameters, especially P-CUT surface area, accurately predict impacted ureteral stones before surgery, which is advantageous for preoperative patient counseling and surgical planning.
Footnotes
Funding Information
No funding was received for this article.
Abbreviations Used
Appendix A1.
Equation to calculate surface area of a circle using its diameter.
P-CUT surface area equation where d1 is ureteral diameter including stone, d2 is stone diameter.