
Abstract
Introduction:
Urolithiasis in solitary kidney (SK) presents significant management dilemma as any insult to the kidney or its drainage can lead to significant morbidity. The treatment options include shock wave lithotripsy (SWL), percutaneous nephrolithotomy (PCNL), and ureteroscopy (URS). Our aim was to conduct a systematic review of literature on all available endourologic techniques reporting on the management of stones in an SK.
Materials and Methods:
We conducted a systematic review according to the Cochrane and PRISMA checklist for all English-language articles from inception to December 2018. All studies with a minimum of 10 patients that reported on endourologic management (SWL, PCNL, or URS) were included. Data were extracted for patient and stone demographics, outcomes including stone-free rate (SFR), adverse events, and renal function.
Results:
After an initial search of 553 articles, 27 were included for the final review (10 PCNL, 1 mini-PCNL, 9 URS, 1 SWL, and 6 comparative studies). The choice of treatment seemed to be based on stone size, with PCNL, URS, and SWL offered for mean stone sizes between 25–50, 10–28, and 12–15 mm, respectively. PCNL, URS, and SWL were reported in 1445, 792, and 186 patients, respectively, with a final SFR of 67%–97.7%, 43%–100%, and 73%–80% and a complication rate of 26.4%, 15%, and 16.7% across the three groups. The renal function deterioration was reported in 4/16 PCNL studies and in 1/15 URS studies, while it remained unaffected in the SWL study.
Conclusions:
Our review shows a rise of endourologic techniques in the management of stones in SK. Although PCNL was used for larger stones, it had a higher risk of major complications, including blood transfusion. While a good SFR was obtained for patients irrespective of the treatment modality, the selected intervention needs to be balanced with its safety profile and the need for ancillary procedures.
Introduction
Urolithiasis in solitary kidney (SK) presents significant management dilemma to the endourologist as any insult to the kidney or its drainage can lead to significant morbidity. The effect of any procedural complication is amplified due to lack of compensatory functional kidney. 1 –4 Treatment objectives should include preservation of renal function and good stone clearance with minimal postoperative complications. Repeated interventions and procedural complications could ultimately render the patient requiring renal replacement therapy. 4 Due to lack of contralateral functioning kidney, there is hypertrophy and dilatation of the effected kidney posing a higher risk of hemorrhagic complications. 1,2 The European Association of Urology guidelines consider these nonindex patients as high-risk stone formers as they have a higher risk of primary and recurrent stone formation and hence achieving a good stone-free rate (SFR) is paramount. 1
Management of stones in an SK is challenging and should be approached with a choice of full endourologic armamentarium depending on the patient demographics and stone characteristics as no modality is without its risks. 2 The choice of procedure needs to be balanced with the SFR and complications along with the need for further ancillary procedures. The treatment options are similar to those with normal kidneys and include shock wave lithotripsy (SWL), percutaneous nephrolithotomy (PCNL), and ureteroscopy (URS). 5,6 Optimal treatment needs to be tailored to the needs of an individual patient and although there are a few studies reporting on this, critical appraisal of these techniques remains underreported. The invasiveness of PCNL needs to be balanced with the ancillary procedures and success rates of URS and SWL, keeping in mind the stone size and renal function of these patients. 4,5 As no randomized trials exist in this complex group of patients, endourologists rely on clinical expertise and available resources to formulate the best management plan for individual patients.
With no recommended guidelines on the management of stones in SK, our aim was to conduct a systematic review of literature on all available endourologic techniques reporting on stones in an SK and to review and summarize the literature on surgical outcomes in these patients.
Method
Study population
Population: Adults with SK and surgical management.
Intervention: URS, PCNL, or SWL.
Comparator: None.
Outcome: Results (renal function, SFR, and complications) of management.
Study design: Systematic review.
Inclusion criteria
Studies in English language reporting on outcomes of surgical management (PCNL, URS, and SWL) of stones in an SK.
Studies that compared surgical treatments where data for individual option could be retrieved and analyzed. In these articles where data were present for more than one surgical option, the data and analysis were done separately and amalgamated with a similar type of procedure. Hence, these articles were counted in more than one surgical option(s).
Studies reporting on a minimum of 10 patients.
Exclusion criteria
Studies where data for individual treatment option could not be retrieved and analyzed separately.
Studies reporting on the treatment of nonurolithiasis conditions or when the procedure was performed in conjunction with another procedure.
Laboratory, animal data, or review articles.
Gray literature and decision analysis models that did not have real patient data.
Search strategy and selection criteria
Our systematic review was performed as per the Cochrane guidelines and Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) checklist.
7
The databases searched included MEDLINE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Excerpta Medica Database (EMBASE), Scopus,
A cutoff of 10 patients was set to include studies from centers with minimum relevant endourologic experience in managing stones in SKs. All original studies were included and where more than one article was available, the study with the longest follow-up was included. Two experienced reviewers (A.P. and T.R.) not involved in the original work independently identified all the studies that appeared to fit the inclusion criteria, which were then included for a full review. Each reviewer independently selected studies for inclusion in the review and all discrepancies were resolved with mutual agreement and consensus with the senior author (B.K.S.).
Data extraction and analysis
The following variables were extracted from each study: year of publication, journal published, country of study, treatment modality, body mass index, etiology of SK, pre- and postprocedural renal function, operative time, SFR, complications, hospital stay, and retreatment rate. Adverse events were graded according to the Clavien–Dindo system. Renal function data were analyzed and graded as stable if there was a variation of up to 10% postprocedure, and better or worse if the variation was more than 10%. Data were collected using Microsoft Excel 2016 (version 16.0). Due to the heterogeneity of the included studies, the authors decided that meta-analysis of effect sizes was not suitable, and hence, either pooled analysis was performed to calculate mean values, or outcomes were summarized in a narrative manner. Each study was assigned a level of evidence in accordance with the guidelines published by the Centre for Evidence Based Medicine (CEBM). 8
Results
Study selection and characteristics
The literature search yielded 553 publications (Fig. 1). After having screened them for eligibility, 27 articles met the inclusion criteria and were included in the final review. These included 10 studies on standard PCNL, 1 on mini-PCNL (MPCNL), 9 studies on URS, 1 study on SWL, 3 comparative studies on standard PCNL and URS, 2 comparative studies on MPCNL and URS, and 1 comparative study on URS and SWL. As five studies had data for both URS and PCNL and one study had data for both URS and SWL, these articles were therefore divided into the respective treatment arms and amalgamated and calculated with a similar type of procedure. Hence, in the results, these six articles appear in two treatment arms.
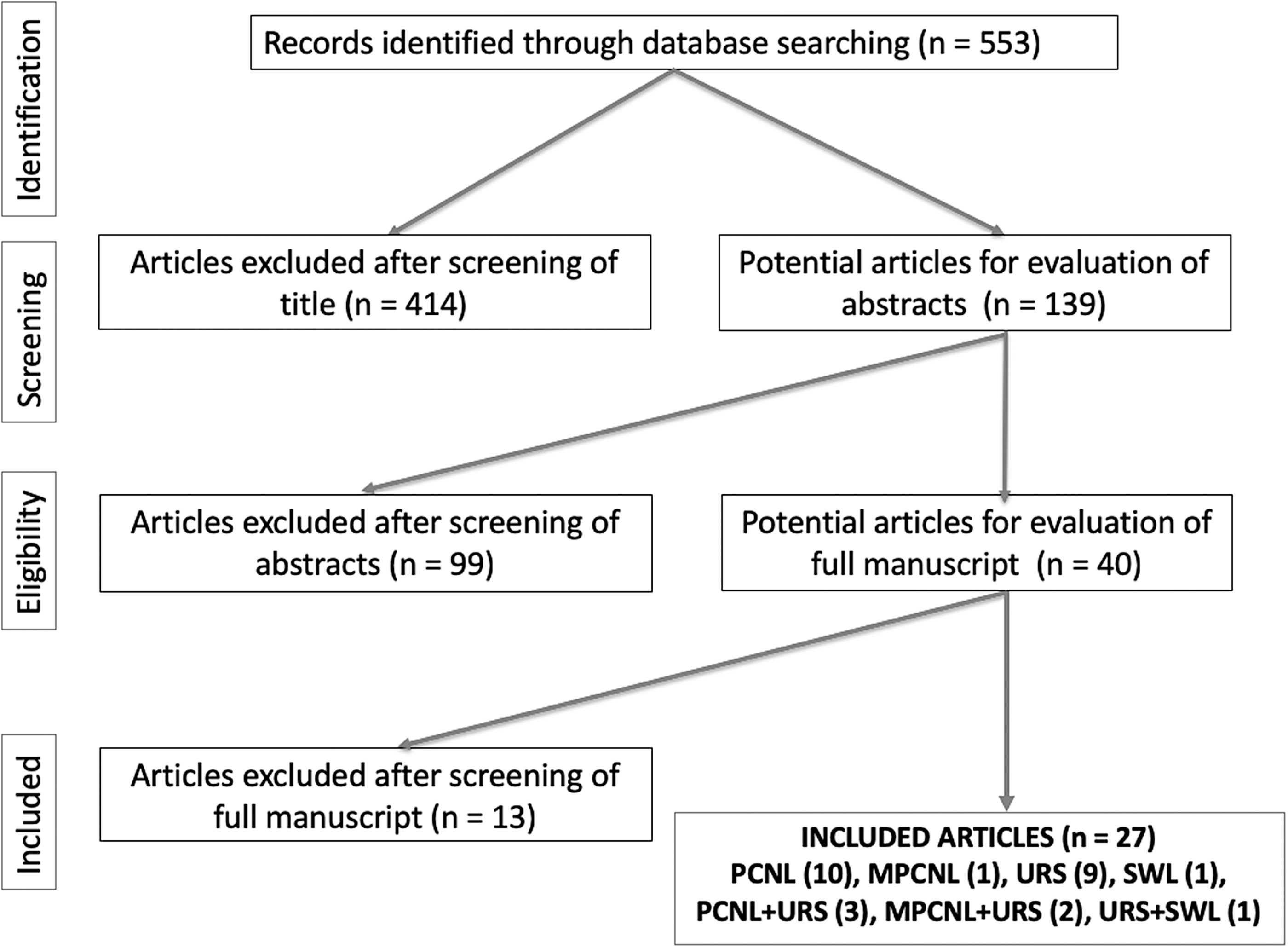
PRISMA flowchart of the included studies.
Percutaneous nephrolithotomy
A total of 16 studies (1445 patients) reported on the outcomes of PCNL in SKs, of which three were on MPCNL 9 –24 (Table 1). The etiology of the SK was mentioned in 11 studies and it varied between studies, with nonfunctioning contralateral kidney as the most common etiology followed by contralateral nephrectomy and congenital agenesis. Across studies, the mean stone size ranged from 25 to 50 mm with a mean operative time of 44–138 minutes and a mean hospital stay of 2–8 days (Tables 2 and 3). The mean and final SFR ranged from 36–85.7% to 67%–97.7%, respectively, and the mean number of procedures to achieve the final SFR was 1.13. Twelve studies (1045 patients) mention ancillary procedures (139 procedures), of which a completion PCNL, URS, and SWL were done in 68 (49%), 28 (20%), and 43 (31%) patients, respectively. Renal function pre- and postprocedure was unchanged in seven studies, 9,13,14,19 –21,24 better in two studies, 11,12 worse in four studies, 10,16,17,22 and was not mentioned in three studies (Table 3). The follow-up time duration is shown in the table and there were insufficient data to include pre- and postprocedure hemoglobin in our analysis.
Baseline Characteristics of Included Studies
Comparative study listed twice.
NS = not specified.
Stone Characteristics of Included Studies
Comparative study listed twice.
CaOX = calcium oxalate-based stones; UA = uric acid stones; Str = struvite stones; Cys = cystine stones; CaPh = calcium phosphate stones.
Summary of Results
Comparative study listed twice.
↑ = renal function got better, ↓ = renal function got worse, ↔ = renal function unchanged.
The overall complication rate for PCNL was 26.4% (382/1445) (Table 4). Clavien I/II complications in standard and MPCNL were seen in 18.1% and 36.4%, respectively, of which blood transfusion was seen in 69/1264 (5.5%) and 12/158 (7.6%), respectively. Clavien ≥III complication in standard and MPCNL was seen in 6.6% and 1.1%, respectively (p < 0.05). Although 13 (1%) Clavien IV complications were seen in the standard PCNL group, only 1 such complication was seen in the MPCNL group, and no postoperative deaths were reported.
Complications of Different Endourologic Management
Ureteroscopy
A total of 15 studies (792 patients) reported on the outcomes of URS in SKs 17 –19,22,24 –34 (Table 1). The etiology of SK was nonfunctioning contralateral kidney or contralateral nephrectomy in most studies. Across studies, the mean stone size ranged from 10 to 28 mm with a mean operative time of 25–117 minutes and a mean hospital stay of 0–5 days (Tables 2 and 3). The mean initial and final SFR ranged from 20%–100% to 43%–100%, respectively. An ancillary procedure was mentioned in nine studies, of which URS was done in 114 (80%) patients, SWL in 26 (18.5%) patients, and PCNL in 2 (1.5%) patients, and the mean number of procedures to achieve a stone-free status across studies was 1.23. Ancillary procedure was not mentioned in two studies, not required in one study (SFR of 100% after the first procedure), and in three other studies the patients who were not stone free were followed up with surveillance scans. Renal function pre- and postprocedure was unchanged in eight studies, 19,22,24,25 –29 better in two studies, 30,31 worse in one study, 17 and unreported in four studies (Table 3).
The overall complication rate was 15.0% (n = 119), of which most were Clavien I (9.6%) and Clavien II (3.4%) complications (Table 4). Majority of these comprised fever (n = 47, 39.5%), transient rise in creatinine (n = 21, 17.5%), and UTI (n = 23, 19%). The Clavien III and IV complications were seen in 1.5% and 0.5%, respectively, and comprised Steinstrasse (n = 10, 8%) and septic shock (n = 4, 3%).
Shock wave lithotripsy
Two studies (186 patients) reported on the outcomes of SWL in SKs 27,35 (Table 1). The mean stone size was 12.5 and 14.9 mm in the two studies with a final SFR of 73% and 80% across both studies although ancillary procedures were needed and the mean number of procedures to achieve the stone-free status was 1.25. Of the ancillary procedures (n = 47), 21 (45%) had URS, 20 (42.5%) had SWL, and 6 (12.5%) had PCNL, 35 although one study used only URS as the ancillary procedure. 27 The renal function remained unchanged in both these studies.
The overall complication rate was 16.7% (n = 31). These included Clavien I complications (n = 17), of which the majority was postprocedure pain. Clavien III complication was Steinstrasse (n = 14), and there were no other complications recorded.
Discussion
Meaning of the study
The main aim of the endourologic procedure in patients with SK should be to preserve renal function and obtain the maximal stone clearance with minimal morbidity. Several studies have been identified on this topic with 12/27 studies published between 2017 and 2018 confirming the increasing intervention rates and interest toward this topic.
The choice of treatment across the included studies seemed to be based on the stone size with larger stones undergoing PCNL (mean stone sizes between 25 and 50 mm). URS was offered for mean stone sizes between 10 and 28 mm, and SWL for stones between 12 and 15 mm. The renal function deterioration was reported in 4 of the 16 PCNL studies and in 1 of the 15 URS studies, while it remained unaffected in the SWL study. Given the compensatory renal hypertrophy, relatively high blood transfusion rates were seen with both standard and MPCNL, despite the smaller tract in the latter.
Importance of this review
Although more invasive, a previous systematic review on PCNL for patients with chronic kidney disease (CKD), of which a sizable proportion also had an SK, showed the feasibility and safety in these patients with an overall improvement of renal function in nearly 10% of patients, although this was not seen in patients with CKD 5 disease. 36 Known to be the more invasive of different endourologic procedures, PCNL is still one of the more effective techniques available for large stones in patients with SK. El-Nahas et al. already demonstrated that due to compensatory hypertrophy and dilatation of the remaining renal parenchyma, SKs have higher risk for hemorrhage. 37
The use of MPCNL for SK with staghorn stones opens a new dimension in the minimization of PCNL. 23 Liu et al., in their retrospective series of 105 patients, looked at the outcomes of MPCNL (16–18F) for partial or complete staghorn stones in SKs and divided the patients into a single-tract or multitract group. 23 Their results confirmed similar SFR but with lesser complication rates for single-tract MPCNL, with a final SFR between 80% and 83% although auxiliary procedures were needed in up to 44% of patients, with a third of them having a repeat MPCNL procedure.
The safety of URS as a treatment option for stones in SK has been previously shown, with a substantial rise in the volume of URS performed for these patients. 38,39 Our results on 15 studies confirm an initial and final SFR of 74% and 85% with a complication rate of 15%, of which the majority were Clavien I/II complications. However, care must be taken in these patients with SK due to risks associated with high intrarenal pressure during URS, which can cause extravasation, perirenal hematoma, and renal injury. 40 Measurement of intrarenal pressure and newer techniques with the use of ureteral access sheath could help reduce the pressure. 40,41 A reduction of operative time with the use of high-power laser, and newer techniques such as dusting and pop-dusting would also improve the SFR for larger stones. 42
There exist limited data on the use of SWL for stones in SK. The main disadvantage seems to be the potential for renal impairment and emergency intervention in the event of obstructing ureteral stone. 27,35 In the article by El-Assmy and colleagues, 35 of the 108 patients who underwent SWL, a pre-SWL drainage (27% ureteral stent, 3% ureteral catheter, and 0.6% nephrostomy) was present in 31% of patients. Post-SWL, a high proportion of patients developed Steinstrasse (9%) with 13% needing a secondary procedure (4% PCNL, 8% URS, and 1% emergency nephrostomy). They do conclude that on a long-term follow-up of 4 years, the renal function and blood pressure were not affected significantly. Although SWL has a low rate of intra- and postprocedural complications, this can require repeat sessions to achieve a stone-free status. 43
Effect on renal function
With only one functioning kidney, preservation of renal function is paramount and treatment objective and surgical option have to balance this aspect. In patients with previous nephrectomy, there seems to be an initial decline in the renal function although this stabilizes over a period of time in most patients. 44 Patients with kidney stone disease carry twice the risk of CKD or end-stage renal disease and this risk is even higher for females and overweight patients. 45 The etiology seems to be a combination of stone-related obstruction, interventions, and infections. 45 To preserve good renal function, it is therefore important to achieve stone-free status and to avoid repeated procedures.
In the PCNL group, renal function pre- and postprocedure was unchanged in seven studies, 9,13,14,19 –21,24 better in two studies, 11,12 worse in four studies, 10,16,17,22 and unreported in three studies. In the URS group, it was unchanged in eight studies, 19,22,24,25 –29 better in two studies, 30,31 worse in one study, 17 and unreported in four studies. In the lithotripsy group, it was unchanged in both studies. 27,35
Outcomes of comparative studies
There were three comparative studies on standard PCNL and URS, 17 –19 two comparative studies on MPCNL and URS, 22,24 and one comparative study on URS and SWL. 27 In the study by Bai et al., the mean stone size, initial/final SFR was 29.6 and 27.7 mm, 36/88% and 20/82% for PCNL and URS groups, respectively, with a reduction in renal function seen across both groups. 17 Another comparative study had an initial and final SFR of 85.7/92.9% and 58.8/85.3% for PCNL and URS, respectively, concluding that the former had a higher one-session stone-free rate for 2–3-cm lower caliceal calculi although URS had lower bleeding and hospitalization stay as a promising alternative to PCNL. 18 The results of MPCNL vs PCNL in the studies were contradictory for SFR, with one suggesting higher SFR and comparable complications 22 and the other showing a lower SFR and more blood loss with MPCNL. 24 When comparing URS with SWL, although both were found to be safe and effective, all patients undergoing SWL were prestented and needed more sessions for stone clearance. 27
Strengths, limitations, and areas of future research
This is the first systematic review to look at all endourologic options together (PCNL, URS, and SWL) for patients with stones in SK. The review is done according to the Cochrane guidelines and PRISMA checklist summarizing the role of endoscopic management for stones in SK. It gives an overview of the SFR, renal function, and complications with all available surgical options, although 20 studies were retrospective case series and hence prone to bias. Furthermore, the heterogeneity in the reported studies and the lack of standardized outcomes made it challenging to do a formal meta-analysis. Given that data collection and reporting were not standardized either, it was difficult to compare or combine outcomes.
There were no randomized comparative trials with seven prospective studies of level three evidence. 11,24,28,31 –34 As with all systematic reviews, we acknowledge the publication bias and that there are limitations to the conclusions drawn, which are only as robust as the included articles. Although the complications were reported according to Clavien–Dindo, a known difficulty in analyzing outcomes was a lack of consensus or information in the measurement of stone size, renal function, and definition of SFR along with the postoperative timing of measuring these parameters. 46,47 A less invasive option such as URS for larger stones could lead to higher recurrence rates due to residual fragments from initial surgery. 48 Another option that has been looked at is a PCNL procedure followed by a planned URS procedure 2–4 days as a part of the SK stone treatment. 49
The review highlights the paucity of high-quality evidence in this area, and hence, it is difficult to draw robust conclusions. An individualized tailored approach would balance the invasiveness of the procedure with complications associated and SFR achieved. Surgical expertise and available resources must also be considered. Although treatment of stones in SK is not common, more evidence ideally through randomized control trials needs to address the best treatment option that is likely to need recruitment from multiple centers. This should also include the cost of treatment and consider patients' quality of life with standardized clinical outcomes and a long-term follow-up.
Conclusion
The outcomes from our review show that there has been a rise of endourologic techniques in the management of stones in SK. While standard PCNL was used for larger stones with a higher risk of major complications, URS and SWL were used for slightly smaller stones. While a good SFR was obtained for patients irrespective of the treatment modality, the selected intervention needs to be balanced with the safety profile and the need for ancillary procedures.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.