
Abstract
Background and Purpose:
Extrinsic ureteral obstruction is caused frequently by pelvic malignancies or metastatic lymphadenopathy, necessitating renal drainage with ureteral stents to prevent renal failure and kidney damage. Understanding the nature of stent behavior under deformation and realistic external pressures may assist in evaluation of stent performance. Few published studies have investigated the flow and mechanical properties of stents within ureters, and none has considered the effects of deformation and compression on flow in realistic, in vitro, ureter-stent systems. The purpose of this work was to determine whether or not stent failure is due only to stent compression and deformation in the presence of extrinsic obstruction.
Methods:
We developed an in vitro ureter-stent experimental setup, using latex tubing to simulate a flexible ureter connecting a renal unit and a bladder side. We examined flow behavior in three stents (4.8F, 6F, 7F). The ureter-stent configuration was varied, simulating four levels of deformation (0°, 20°, 40°, 60°) and then simulating different external compressive forces on a stented ureter with 40° deformation. A constant, realistic fluid flow was applied through the ureter-stent configurations, and pressure fluctuations in the renal unit were monitored.
Results:
Deformation alone on four different levels (0°, 20°, 40°, 60°) has essentially no influence on fluid flow and renal pressure variation. Under increasing external compressive forces of 500, 1000, 2000, and up to 5000 g at 40° deformation, no effect on fluid flow and pressure within the renal unit was noted for the 6F and 7F stents. The only exception was for the 4.8F stent, which demonstrated complete failure at compressive forces near 4000 g.
Conclusions:
Neither realistic extrinsic ureteral compression forces nor ureteral deformation explain the high frequency of stent failure in extrinsic ureteral obstruction. Other factors such as urine composition may be a major contributor to stent failure.
Introduction
Extrinsic ureteral obstruction is a challenging situation in which compression and deformation of the ureter occur and lead to renal insufficiency and potentially irreversible damage to the kidney. In most cases, the etiology is malignant, that is, not only malignant pelvic tumors, metastases, or pelvic lymphadenopathy, but also benign causes have been reported such as ovarian cysts, retroperitoneal fibrosis, and benign pelvic masses. Under external ureteral obstruction, drainage of the kidney is imperative and frequently achieved by placement of ureteral stents. However, stent failure is not uncommon under such circumstances and can be as high as 45%, often occurring as early as 1 day to 1 month after placement. 1,2
The exact cause of stent failure is not clear, but it is frequently attributed to closure of the volume between the stent and ureteral wall, as well as closure of the stent lumen, 3 –6 especially over shorter periods (e.g., 1 month) before biofilm and encrustation processes might be expected to play a major role. Other factors that have been suggested include effects of malignant tumors, renal failure, use of chemotherapy, and bladder invasion as observed by cystoscope, 3 as well as the presence of debris in urine. 1 The purpose of this work focused on determining the extent to which stent failure is due only to stent compression and deformation in the presence of extrinsic obstruction.
Previous studies of in vitro experiments reported high and unrealistic external forces required to fully compress the stent lumen. 3 –6 Moreover, these experiments are limited as they employed two-point forces on opposing sides of the stent, or used inflexible ureter models. 7 The few available experimental studies employing in vitro and ex vivo stent/ureter flow models generally employ either glass or fixed geometry (straight) tubes. 7 –11 Such arrangements do not facilitate simultaneous in vitro investigation of deformation and compression in combined ureter-stent systems. Here, in contrast to the existing literature, we used an in vitro model of a stent within a ureter to investigate the influence of the flexible ureteral wall itself on stent compression and on the resulting combined (ureter-stent) flow dynamics, under ureteral deformation and realistic compressive forces.
Materials and Methods
We define here two terms used throughout this study: deformation and compression. Deformation refers to curvature of the ureter by natural variation (neither end is pinned perfectly straight), and by patient position or posture, as well as curvature induced by the presence of an extrinsic ureteral pressure (Fig. 1a). These features lead to variable positioning of a stent within the ureter, both temporally and along the length of the ureter. As a consequence, there is spatiotemporal variation in contact regions between stent and ureteral walls along the length of the ureter, which may be further mediated by peristalsis effects. Thus, the location of stent holes and their ability to improve fluid flow by pressure equalization between ureter lumen and stent lumen varies naturally over time and distance along the ureter.

Deformation and compression of the ureter-stent system:
Ureteral/stent deformation also occurs in the presence of an extrinsic ureteral pressure, which also causes compression (Fig. 1b). This is characterized as either partial closure of the stent by reduction in diameter and change in circular cross-section or, under sufficiently strong compression, complete closure of the stent cross-section.
Theory
It should be recognized that in terms of hydrodynamics, volumetric flow of urine from each kidney in the range of 25 to 50 mL/h, in a tube with 3-mm internal diameter (approximately that of a ureter), is very low, yielding essentially a laminar flow scenario. 12 This is supported by calculation of the Reynolds number, Re = ρud/η (where ρ and u are urine density and velocity, respectively, η is dynamic fluid viscosity, and d is ureter diameter).
Assuming a volumetric flow of 50 mL/h, with d = 0.3 cm, ρ ≈ 1.01 g/cm3, and urine viscosity 13 at 37°C of ≈8.4 × 10−4 Pa·s (η ≈ 8.4 × 10−3 g/cm·s), leads to the very small value of Re ≈ 7; this indicates that inertial forces are small compared with viscous forces, and that flow is laminar (the onset of turbulent flow is at Re >2000). In practical terms, such as in the experimental setup discussed next with saline water at 24°C (and Re ≈ 6.5), a flow rate of, for example, ∼30 mL/h translates to only about one drop of outlet fluid every 3 seconds.
To appraise urine flow in ureter-stent systems, laminar fluid flow is calculated easily for idealized systems via Poiseuille's law. For fluid flow in tubes with a circular cross-sectional area, the volumetric fluid flow rate, Q, for flow in a tube of length l, with circular cross-section of radius r, pressure difference across the tube inlet and outlet P, and dynamic fluid viscosity η, is given by Q = (πPr 4 )/(8η l).
In vitro stent-ureter-kidney model
We developed an in vitro ureter-stent experimental setup, using latex tubing to simulate a flexible ureter connecting a renal unit to the bladder side, and examined combined flow behavior in the ureter-stent system. The experimental setup is shown schematically and as a photograph in Figure 2a and b, respectively. Double-J stents (Boston Scientific® Percuflex Plus) with diameters 4.8F, 6F, and 7F were employed. The proximal pigtail end was inserted into a ∼40-mL glass vessel (“renal unit”). The bladder (distal) side curl was removed, and the stent/ureter opening was drained freely with the latex tubing extending beyond the stent.
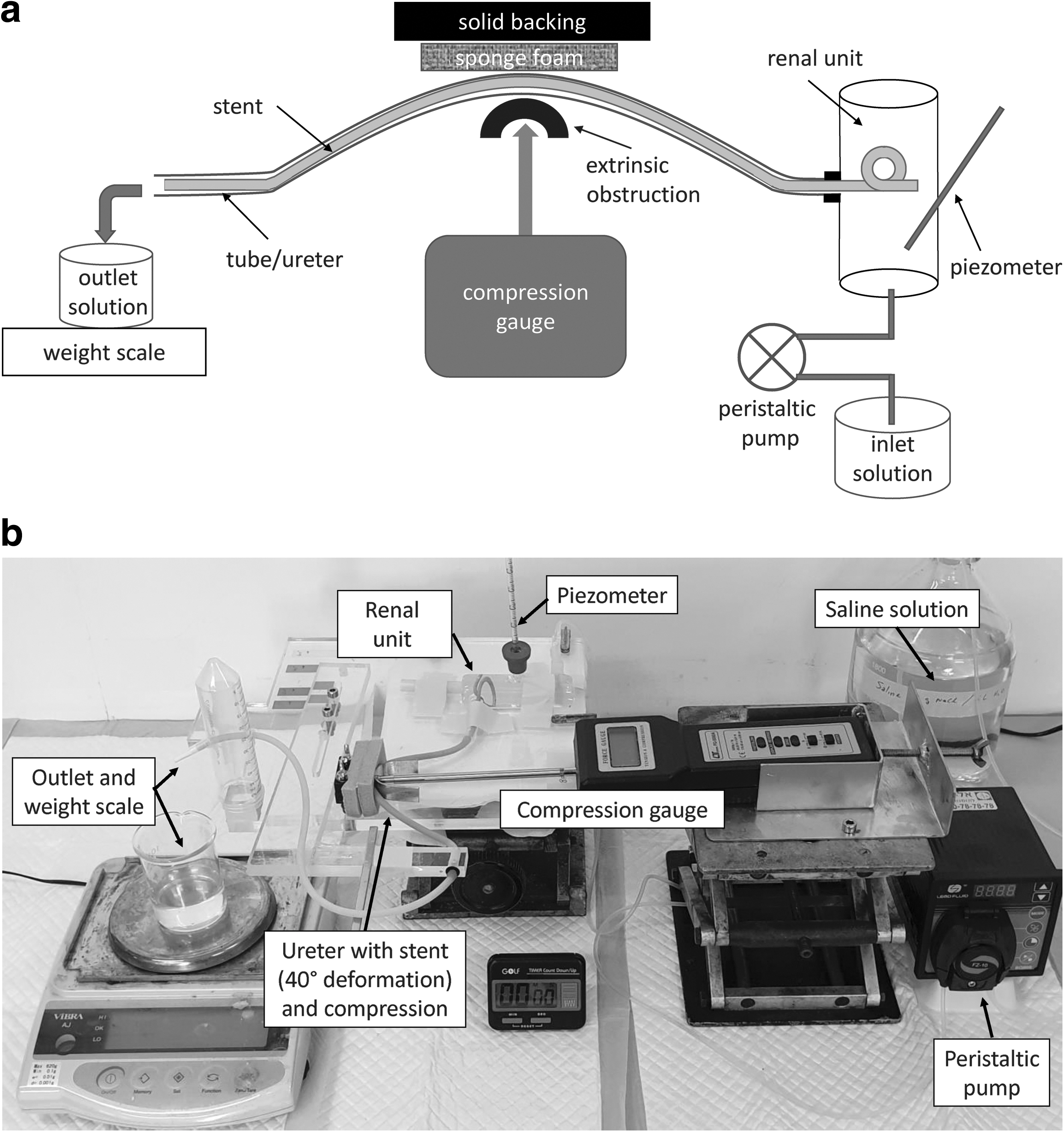
A peristaltic pump controlled fluid input at a constant flow rate for all experiments, and the flow rate at the outlet (bladder) side was measured over time for each ureter-stent configuration by recording fluid weight at various times. In parallel, fluid pressure in the renal unit was monitored via a piezometer. All experiments employed saline solution (9 g NaCl/L), to allow investigation of pure fluid and mechanical effects. The fluid volume in the renal unit acted to damp the small pressure fluctuations induced by the pump.
The ureter was simulated by a natural latex rubber tubing (NEWTEX; NewAge® Industries, Inc.), with inner diameter 3.175 mm (1/8 inch) and wall thickness 0.79 mm (1/32 inch). Several types of tubing were tested by different senior urologists and the one that felt most similar to ureter consistency was selected. The choice of latex tubing to mimic a ureter, without peristalsis, is further justified because stenting usually results in a pronounced reduction of ureteric peristalsis. 14 Moreover, increased accumulation of extracellular collagen can occur in dilated ureters, causing increased wall stiffness and reduced distensibility. 15
Experiment description
Using a constant flow rate of 32.5 mL/h to simulate normal urine production of a single kidney, fluid flow through the ureter model without stent was initially tested for all deformation chosen angles from 0° to 60°. No rise in renal unit pressure was noted. The ureter-stent configuration was then tested, first allowing for deformation from straight (pipe, θ = 0°) geometry deformation over three angles (θ = 20°, 40°, 60°, the latter being an extreme case), as shown in Figure 3. Pressure in the renal unit was measured as height in the renal unit piezometer for the different ureteral deformations. Repeated measurements for each stent were done, and two 7F stents were tested to confirm reproducibility. Then, external compressive force was applied over the ureter-stent configuration while on 40° deformation for each ureteral stent to simulate an extrinsic pressure.

Schematic diagram showing definition of “angle of deformation,” θ, prescribed in the experiments at θ = 0° (straight tube), 20°, 40°, 60°.
External compression force was induced by the presence of a semi-circular metal plate of diameter 3.5 cm. The metal plate was located in the region of maximum deformation and was countered by two layers of foam (2 × 9.5 mm thick, Contour Foam; Sammons Preston Rolyan) backed by a metal brace to simulate resistance offered within the abdominal cavity (Fig. 2a, b). The length of the resulting compression along the ureter-stent system is generally longer than those previously considered. 3 –7 Although previous studies examined pressure between two opposite points, directly on stents, we suggest that external pressure over a 3.5-cm ureteral segment is more realistic, as frequently seen with either pelvic tumor or lymphadenopathy. The extrinsic pressure was pressed against the ureter/stent configuration by a force meter (Lutron, Model FG-5000A).
Recognizing that the true in vivo forces exerted by extrinsic ureteral obstruction are currently unknown, we assessed different external compressive forces of 500, 1000, and 2000 g (1000 g force ≈9.8 N). Higher forces of up to 5000 g were also tested, although the likelihood of generating such compression in abdominal tissue appears low. Each stent was removed after completion of the experiments. It is noted, too, that the actual compressive force exerted on the stent is expected to be lower given the dissipative effects of both the additional ureter (latex tubing) wall and the extent of the compressed ureteral segment.
Results
Experimental measurements of fluid flow with deformation in ureter-stent configurations
As a control for the experimental system, measurements were first made with the ureter (latex tube) in the absence of a stent. Each stent within the ureter was then tested. Under all four deformation conditions (0°, 20°, 40°, 60°), as well as in the ureter-only case, the volumetric flow was confirmed constant (32.5 mL/h) via weighing fluid at the outlet over time. In all cases, the maximum deviation from this flow rate at the system outlet was 1%. Moreover, the fluid height in the renal unit piezometer in all cases (ureter only and the 4.8F, 6F, 7F stents, at all four deformation angles) remained constant, displaying only ∼1 mm (∼0.1 cmH2O) height variation due to the action of the peristaltic pump.
Experimental measurements of fluid flow in ureter-stent configurations under external compression pressure
The effect of compressive force was tested for the 40° configuration. In all of the experiments cited next, the volumetric flow was confirmed to be constant (32.5 mL/h) via weighing fluid at the outlet over time. In all cases, the maximum deviation from this flow rate at the system outlet was 1%. As summarized in Table 1, renal unit pressure changes were detected in only some cases. With increasing compressive force, no additional pressure increases were detected, within an error of 0.1 cmH2O. We defined stent failure as an increase of 10 cmH2O in the renal unit pressure. There was no visible sign of compression or damage to the stent even after reaching 5000 g compressive force within the ureter/latex tubing.
Effect of Compression (at 40° Deformation) on Fluid Flow/Pressure Changes

Table entries show pressure increase in renal unit.
Rise of 3.7 cmH2O within 60 seconds, 5 cmH2O within 12 minutes, and 10 cmH2O within 30 minutes.
Discussion
Failure of ureteral stents under extrinsic ureteral obstruction is a common phenomenon that is usually believed to be secondary to elevated compression pressure, leading to compressed ureteral walls and closure of stent lumen. In this experiment, we examined the impact of ureteral deformation and external compression forces over a stented ureter to evaluate stent failure. We developed a unique in vitro experimental setup of a stented ureter. Our model consists of a ureteral stent placed within a simulated ureter, with external pressure applied on the stented ureter and over a ureteral segment, rather than point pressure applied directly on a stent.
We considered stent failure as rising pressure of more than 10 cmH2O within the renal unit. Although this pressure is lower than the accepted pressure for obstruction as defined, for example, by the Whitaker test (20 cmH2O), we suggest that the gradual rise in pressure will ultimately lead to stent failure. 16
Our results show that for any level of deformation of the ureter up to 60°, no rise in renal unit pressure occurs. Considering the low fluid flow within the ureter, laminar flow is inevitable also for a deformed ureter, even accounting for any dilation and changes in peristalsis due to the presence of an indwelling stent. Based on Poiseuille's law, for urine, 13 η ≈ 8.4 × 10−3 Pa·s at 37°C, with ureter radius and length of r = 0.15 cm and l = 24 cm, respectively, and a pressure of 1 cmH2O ( = 98.0665 Pa), we find that Q = 0.0955 cm3/s, or 348 mL/h. Thus, given that urine production is usually only in the range of 25 to 50 mL/h in a single kidney, pressures 7 of up to 20 cmH2O within the renal unit are certainly not relevant, unless the ureter is obstructed.
Further, considering slow, laminar flow rates of urine through the ureter, the effect of ureter-stent curvature, for example, even in the range of up to an extreme angle of 60°, is associated with negligible friction losses. 17 Thus, deformation alone, as may be seen in natural variation, abdominal “geometry,” and by patient position/posture, has little influence on the volumetric flow rate of urine or renal pressure.
At external compression of 1000 g, we noted complete obstruction of the nonstented ureter, leading to an increase in renal unit pressure. Therefore, we might expect that for external ureteral force equal or higher than 1000 g on a ureter-stent system, all of the fluid flow is likely to flow through the stent itself, in the region of compression. If the extrinsic obstruction completely encapsulates the ureter, then this is certainly the case (the entire cross-section of the ureteral wall can be compressed against the stent); if compression is only two-dimensional (lateral to the ureter/stent), then the ureter cross-section can become more elliptical, enabling some fluid flow outside the stent even in the region of compression. In any case, holes along the length of the stent can be expected to facilitate urine communication and flow between the stent and the ureter lumina, on either side of the compression region.
A recent analysis 6 focused on measuring luminal reduction (% cross-sectional area) as a function of compression for 4.8F, 6F, and 7F ureteral stents. Pressure was applied directly over the stent, at two opposing points. The study found that the luminal area of the 4.8F stent was reduced by 57% and 91% at compressive forces of 1065 g (10.44 N) and 1771 g (17.37 N), respectively. For the 6F stent, luminal areas were reduced by 62% and 95% at compressive forces of 2868 g (28.13 N) and 3775 g (37.02 N); for the 7F stent, luminal areas were reduced by 50% and 100% at compressive forces of 2589 g (25.39 N) and 3587 g (35.18 N).
In contrast, we found in our experiments—which involve the stents inserted within a ureter, a more realistic length of external ureteral compression, and measurement of the actual fluid flow—that up to 3000 g compression, there is essentially no change in fluid flow or pressure (∼3 mm H2O height) in the 4.8F, 6F, and 7F stents. Two key observations can be made: (i) particularly for the 4.8F stent, the effect of compression on the stent within a ureter is less significant than compression directly on the stent, 6 at least when considered in terms of fluid flow; and (ii) even relatively high degrees of reduction in luminal area (stent and/or ureter)—which we expect occurred in the experimental setup—have little to no effect on fluid flow, at least at typical flow rates.
Indeed, we emphasize that measurement of reduction in luminal stent area 3,6 does not provide information on the resulting flow dynamics, particularly for laminar flow regimes and relatively low flow rates. In similar two-point compression tests on stents, Hendlin and colleagues 4 (fig. 4 of that paper) reported a linear decrease in flow of normal saline solution, at a rate of 5 mL/s/mm of compression for a 10.2F stent. Two critical points should be recognized. First, the initial flow rate was ∼20 mL/s (i.e., ∼1200 mL/h), far greater than real urine flow rates of 25 to 50 mL/h, and therefore expected to be more sensitive to changes in stent cross-sectional area. Second, even at a final compression of ∼3.4 mm (which might be expected to represent “complete closure” of a 10.2F stent lumen), the measured flow rate was ∼5 mL/s (∼300 mL/h). This result clearly supports our point (ii). With regard to (i), we note that the ureteral wall and the length of the external ureteral compression dissipate some of the compressive force applied on the stent.
Particularly in the context of these findings, we note that stent sizes (4.8F–7F) indicate the outer wall diameter of the stents. Wall thicknesses of different stents (4.8F–7F) can vary, even among the same manufacturer as well as among different manufacturers. 3 For example, the wall thickness of the 4.8F stent examined here was 0.22 mm, notably smaller than the 0.40-mm thickness measured for the 6F and 7F stents. This, of course, affects both stent resistance to compression and the inner stent diameter that determines volumetric flow rates.
In this context, Davis and colleagues 6 discussed inconsistencies in the use of traditional French sizing, and they concluded that the stent “material area” relative to cross-sectional area is a critical control on stent behavior subject to compression. An earlier study 18 also found that stent wall hardness can be more critical than stent diameter. We demonstrate that, in addition, two other key factors are the presence of the ureteral wall and the actual length of the external ureteral compression, which dissipate some of the compressive force applied on the stent.
Thus, we demonstrate here that compression induced by the presence of an extrinsic ureteral pressure has little influence on fluid flow output, regardless of any possible reduction in stent diameter or change in circular cross-section, at least under realistic abdominal compressive forces of up to 2000 g. It should also be noted that the stent pigtails residing within the kidney and bladder enable stent motion along the ureter; this motion might mitigate stent compression under (at least initial) deformation and/or application of compression.
Based on the results of these experiments, deformation and compression forces on the ureter do not appear to play a major role in stent failure. The question that then remains to be answered is: What is the reason for stent failure under extrinsic ureteral obstruction? We speculate that urine viscosity combined with aggregation of debris and large molecules are a common actual cause of stent failure, leading to occlusion of both the stent and ureter lumina, as has been previously suggested 1,4 ; whereas stent encrustation and incrustation, biofilm development, and impaired peristaltic action may lead to failure over longer periods. This has yet to be clarified and further experiments using artificial and/or real urine, at body temperature, are currently under investigation.
There are several limitations to our study. The latex tube used to simulate a ureter may have physical characteristics different than a real ureteral wall, and it lacks the peristaltic motion of a real ureter, which may potentially have affected our results regarding the flow dynamics. We note that indwelling stents cause dynamic ureter responses, including dilation and changes in peristalsis, which will further affect the flow dynamics over time. Such dynamics may include reflux or retrograde pressure transmission through and/or around the stent, although clear specification of the dynamic changes remains uncertain. Finally, the use of saline solution, with viscosity different from urine, may also affect the deformation and compression measurements to some degree.
Conclusions
Stent failure under extrinsic ureteral obstruction is a common situation and the mechanism for it has yet to be clarified. One of the major parameters believed to be responsible for stent failure is extrinsic pressure placed on the ureter and stent.
We found that to impair fluid flow through a stented (4.8F) ureter, unrealistic pressure of more than 4000 g is required; compressive forces up to 5000 g had essentially no effect on the 6F and 7F stents. Moreover, deformation of the ureter in addition to compression will not result in failure under realistic external compression forces.
Future experiments using urine and ex vivo models may assist in a better understanding of the mechanism for stent failure under external ureteral pressure and may direct the most appropriate drainage device.
Footnotes
Acknowledgments
B.B. appreciates the support of a research grant from the Estate of Emile Mimran. B.B. holds the Sam Zuckerberg Professorial Chair in Hydrology. The authors thank Prof. Jacob Karni for useful discussions on fluid dynamics.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.