
Abstract
Objective:
To compare the efficacy and safety of a single-use digital flexible ureteroscope (f-URS) and a reusable digital f-URS (URF-V) for the treatment of renal stones in adults.
Patients and Methods:
In this randomized open-label noninferiority trial, we randomly selected patients with renal stones to receive ureteroscopy through a single-use digital f-URS (ZebraScope™; Happiness Workshop, Beijing, China) or a URF-V (Olympus, Tokyo, Japan). The primary endpoint was the 1-month postsurgical stone-free rate (SFR). The secondary efficacy endpoints assessed were the high-quality rate of images, the eligible rate of operability, the operative time, and the length of hospital stay. The safety outcomes assessed were the presence of postoperative complications, adverse events (AEs), and serious AEs (SAEs). The noninferiority margin was set at −10%.
Results:
In total, 126 patients completed the study (i.e., 63 patients in each group). The demographic and preoperative parameters were comparable between the two groups. The 1-month SFR was 77.78% for the ZebraScope group and 68.25% for the URF-V group (two-sided 95% confidence interval [CI]: −5.95 to 25.01). The high-quality rate of images and the eligible rate of operability were 100% in both groups (two-sided 95% CI: −5.27 to 5.35). There was no difference between the two groups in the operative time (p = 0.687), the length of hospital stay (p = 0.430), the presence of postoperative complications (p = 0.310), the presence of AEs (p = 0.709), and the presence of SAEs (p = 0.648). The most important and fatal SAE was acute urinary tract obstruction.
Conclusion:
The single-use digital f-URS (ZebraScope) appears to be at least noninferior to URF-V regarding the 1-month SFR, the high-quality rate of images, and the eligible rate of operability. Single-use digital f-URSs are an effective and safe alternative to URF-V.
Introduction
Nephrolithiasis is a highly prevalent disease worldwide, ranging from 7% to 13% in North America, 5% to 9% in Europe, and 1% to 5% in Asia. The management of stones is expensive because of the high rates of forming new and recurrent stones. 1 In some countries, flexible ureteroscopy (f-URS) is used as a first-line treatment modality for renal stones, and currently, it has exceeded other modalities by 30%. 2 –4 In the recent revision of the European guidelines on the management of urolithiasis, both endourology (percutaneous nephrolithotomy [PNL] and URS) and extracorporeal shock wave lithotripsy (SWL) were recommended as first-line management options, especially for stones measuring between 10 and 20 mm. However, for stones >1.5 cm in the lower pole, PNL or f-URS is recommended. 5
The existing constraints on reusable f-URS include a high initial purchase cost, vulnerabilities, high expenditures for repair, and a risk of cross-infection, resulting in the increased use of single-use f-URS. 6,7 Over the past few years, there have been encouraging reports on the improvement of single-use f-URS. Many results of in vitro experiments of single-use digital f-URS were comparable with those of current reusable f-URS in optics, deflection, and irrigation flow. 8,9 Clinical studies have indicated that single-use digital f-URS performed comparably with current reusable fiber-optic f-URS in terms of the stone-free rate (SFR), operative time, and complication rate. 10 –12
However, there has still not been a prospective clinical study for comparing the efficiency and safety of single-use digital f-URS with those of their reusable digital f-URS (URF-V) counterparts. Therefore, we designed and conducted a parallel randomized control trial (RCT) to evaluate the efficacy and safety of a single-use digital f-URS (ZebraScope™; Happiness Workshop) compared with a URF-V (Olympus, Tokyo, Japan).
Patients and Methods
Study design, ethics, and registration
A multicenter randomized open-label noninferiority trial with balanced randomization [1:1] was performed in four hospitals in China from September 2018 to February 2019. The sample size was calculated according to the noninferiority sample size calculation. Randomization was carried out using computerized random numbers. The allocated treatment for each patient was recorded in concealed envelopes. After achieving the patient's consent for participation in the trial, the concealed envelopes were opened, and the allocated treatment was performed. The clinical study was approved by the ethics committees of the four institutes (2018K032) and was registered in the Chinese Clinical Trial Registry (ChiCTR1900021615), and was conducted in accordance with the ethical standards of the Declaration of Helsinki. Sample size calculation is as follows:
The significance level (α) was 0.05 and the power (1–β) was 0.80. Δ refers to the noninferiority margin of −10%. PT and PC refer to the expected effective rate in the trial and control group. |D| is the absolute value of the expected effective rate between the two groups. Assuming a dropout rate of 15%, 61 participants will be needed in each group, yielding a total of 122 participants needed for this study.
Inclusion and exclusion criteria
The inclusion criteria were as follows: Maximum stone diameter of 6 to 20 mm confirmed by a computed tomography (CT) scan. Stones located in the renal or upper ureter. Adults aged 18 to 75 years.
The exclusion criteria were as follows: Coagulopathy or currently on anticoagulation therapy. Anatomic abnormalities, such as horseshoe kidneys, caliceal diverticula, ureteral strictures, ureteropelvic junction obstructions, infundibular stenoses, and impassable urethral strictures. Comorbidities that interfere with the participation in or the completion of the study, for example, myocardial infarction, stroke, congestive heart failure, severe chronic respiratory lung disease, cancer, uncontrolled diabetes mellitus, pregnancy, mental illness, and severe systemic diseases or psychosis. Severe deformity of the hip joint, which cannot meet the requirement of the operation position. Patients who participated in other clinical trials within 3 months.
Study population
In total, 134 patients were recruited and allocated to the trial group (n = 68) or the control group (n = 66) from October 2018 to January 2019. All the patients were enrolled in the study after a routine preoperative evaluation including urinalysis, urine culture, complete blood count, renal function, electrolyte determination, and nonenhanced CT.
Investigational device
Single-use digital f-URS ZebraScope (Fig. 1) was utilized in the trial group. The structures of ZebraScope are shown in Figure 2. The major parameters of the device are as follows: it weighs 185 g with a 670-mm working length, and can deflect 275° in the upward and downward directions. The outer diameter is 8.7F, the tip diameter is 7.4F, and the working channel for irrigation and insertion of instruments is 3.6F.

Main part of Chinese single-use digital f-URS ZebraScope™ (Happiness Workshop). f-URS = flexible ureteroscope.
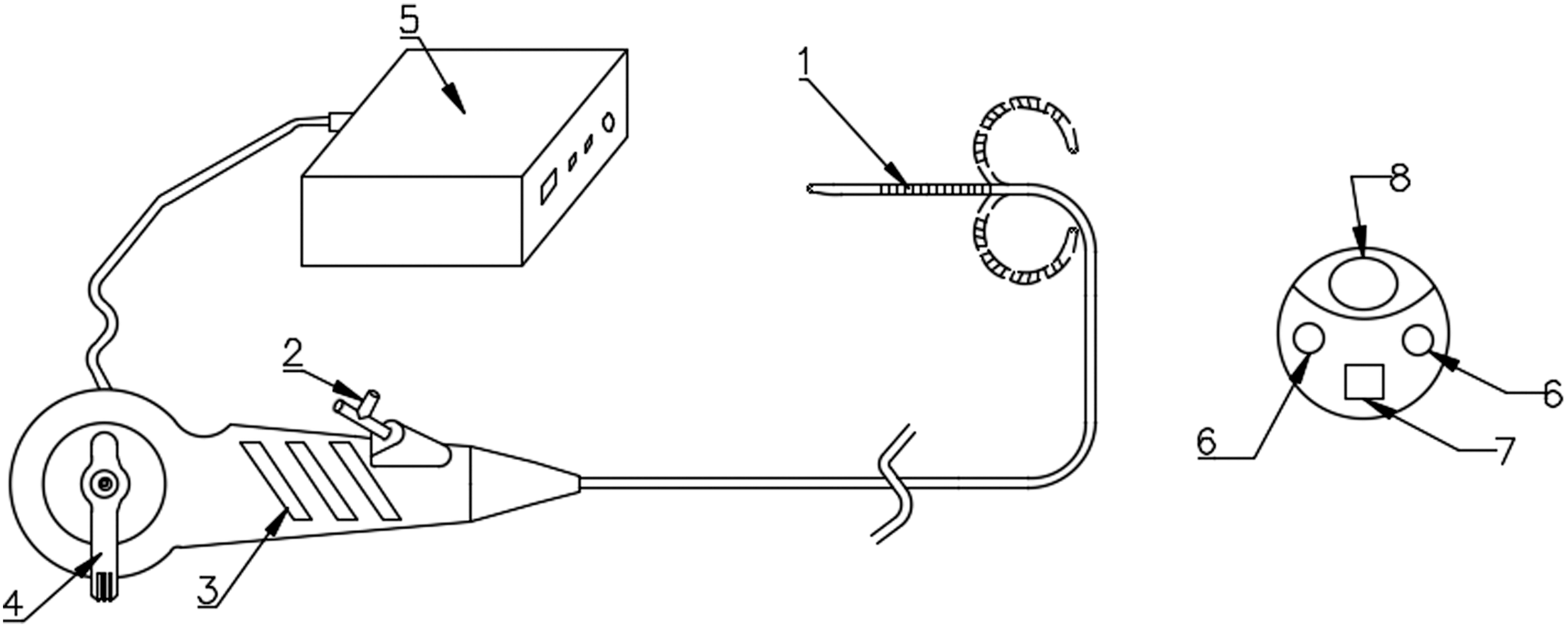
The structures of the single-use digital f-URS ZebraScope. (1) Flexible tip of 275°, (2) entrance of working channel, (3) Handle, (4) control lever of direction, (5) host system of imagining, (6) light sources, (7) image module, (8) exit of working channel.
Surgical technique
All the procedures were performed by doctors experienced with the use of f-URS. Prophylactic antibiotics were given to all patients according to the local antimicrobial guidelines. The patients were given general anesthesia and placed into the lithotomy position. An F8/9.8 rigid URS was placed into the ureter to observe whether the ureter has stenosis or deformity and to dilate the ureter to facilitate the placement of a ureteral access sheath (UAS).
Then, a 0.038-inch Zebra guidewire was inserted through a rigid URS. After positioning the guidewire into the ureter, the rigid URS was removed, and a 12/14-Fr Flexor UAS (Cook Urology) was placed in the ureter. The 8.7-Fr ZebraScope or the 9.9F URF-V f-URS was placed into the pelvis through the UAS. Holmium laser lithotripsy was performed by a 200-μm laser fiber with a power setting of 0.8 to 1.5 J at a frequency of 10 to 20 Hz. A manual irrigation system (syringe technique) was used to maintain an appropriate low intrarenal pressure to guarantee enough space to break the stones and to avoid intrarenal backward flow. A 1.7F or 2.4F Nitinol basket was used for lower caliceal stone extraction or relocation from the lower calix. A 6F Double-J stent was indwelled for 4 weeks, and a Foley catheter was placed in the site.
Outcome assessment
The primary endpoint was the 1-month postsurgical SFR. The secondary efficacy endpoints assessed were the high-quality rate of images, eligible rate of operability, operative time, and length of hospital stay. The safety outcomes assessed were the presence of adverse events (AEs), serious AEs (SAEs), and postoperative complications, including pain, fever, renal hematoma, hematuria, pelvicaliceal system injury, urinary sepsis, and steinstrasse formation.
At the end of surgery, the surgeon would measure performance of the URS. If the image was bright enough and the capillaries and mucosa were clearly visible, the surgeon would consider it a high-quality image. The operability of f-URS was considered eligible by meeting the following criteria: (1) the tip could bend up and down under handle control and (2) various endoscopic instruments, such as laser fibers, baskets, and different kinds of graspers, could be used in the working channel. The operative time was defined as the time from URS insertion until the end of Foley catherization. “Stone-free” status was defined as no residual stone or stones ≤4 mm by plain abdominal radiograph of the kidneys, ureters, and bladder (KUB) and by CT scan at 1 month after stent removal. The radiologists who performed the CT scan and the KUB radiograph were totally blinded to the study objectives and protocols.
Statistical analysis
We analyzed the primary outcome data obtained from the patients who had an effective surgery and completed the 1-month follow-up. To assess whether ZebraScope could be considered noninferior to URF-V in terms of the 1-month SFR, high-quality rate of images, and eligible rate of operability, the Newcombe–Wilson confidence interval (CI) was computed using the URF-V group as the control. 13 This method involves constructing a two-sided 95% CI of the difference in the SFR, high-quality rate of images, and eligible rate of operability of the two f-URS groups and determining whether the lower limit of CI was greater than the noninferiority margin of −10%.
The data were analyzed by using Statistical Package for the Social Sciences, V. 22.0 (SPSS; SPSS, Inc., Chicago, IL). Continuous variables were compared by independent samples t-tests. Categorical variables were compared by chi-square or Fisher exact tests, as appropriate. All analyses were planned by intention to treat.
Results
Patients and stone characteristics
Of the 134 patients identified, 126 patients completed the study, including 63 patients in the ZebraScope group and 63 patients in the URF-V group. The flow chart of the trial is shown in Figure 3. The patient and stone characteristics are given in Table 1. The mean age of the patients in the trial group was 51.84 years, with a mean body mass index (BMI) of 26.07 kg/m2. The mean age of the patients in the control group was 53.25 years, with a mean BMI of 25.84 kg/m2. The mean stone sizes were 11.09 and 11.08 mm in the trial and control groups. No significant differences were observed between the groups in terms of age, gender, stone size, stone location, or preoperative condition.
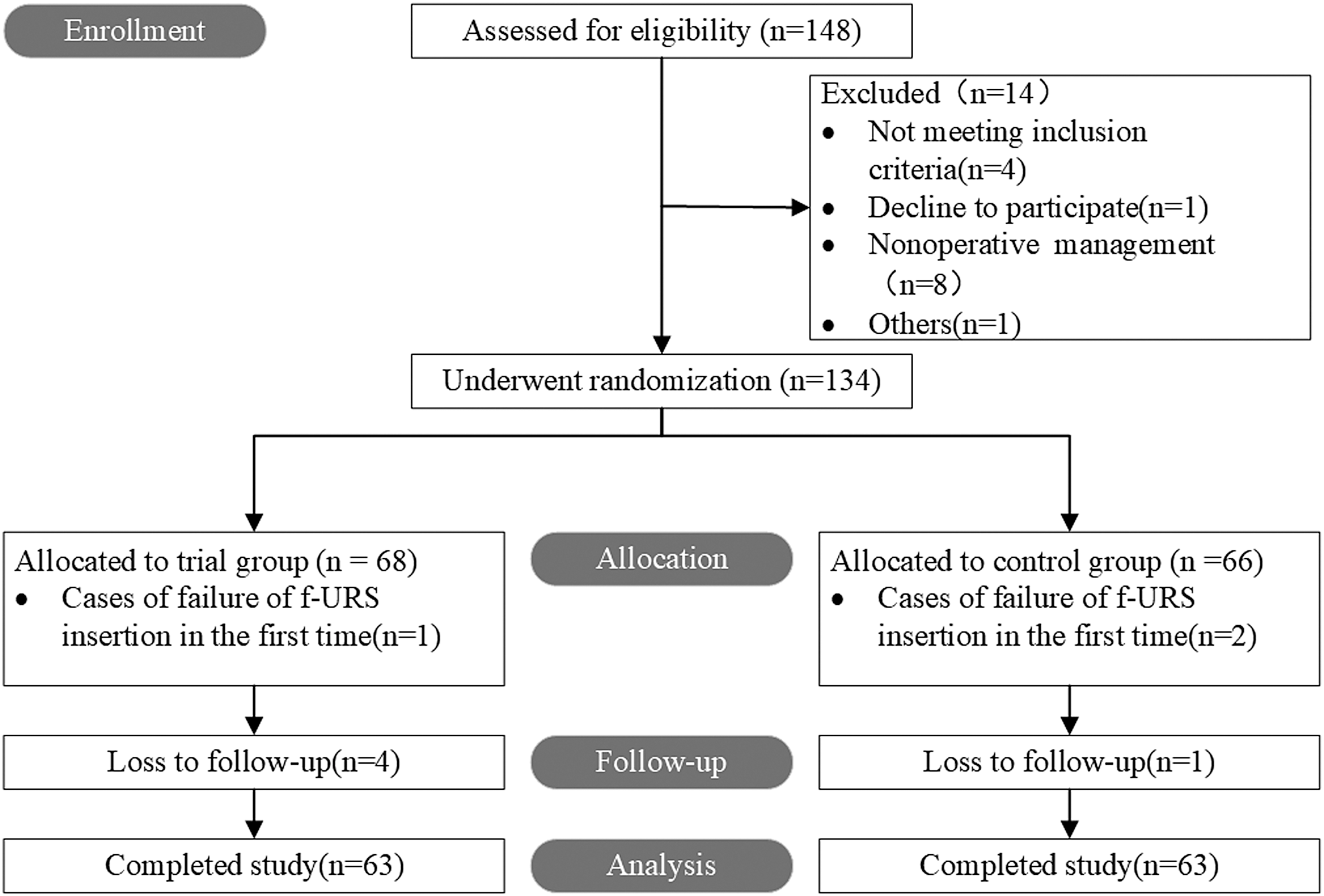
Flow diagram showing study recruitment.
Baseline Demographics and Clinical Characteristics of 126 Patients with Renal Stones Who Received Ureteroscopy Through a Single-Use Digital Flexible Ureteroscope (ZebraScope) in Trial Group or a Reusable Digital Flexible Ureteroscope in Control Group
BMI = body mass index; CT = computed tomography; LUTS = lower urinary tract symptoms; PNL = percutaneous nephrolithotomy; SD = standard deviation; SWL = extracorporeal shock wave lithotripsy.
Outcomes
The surgical outcomes are shown in Table 2. The 1-month SFR was 77.78% for the ZebraScope group and 68.25% for the URF-V group (p = 0.229). We assessed the noninferiority of ZebraScope in terms of the 1-month SFR, high-quality rate of images, and eligible rate of operability using URF-V as the control. If the lower limit of the 95% CI was greater than the noninferiority margin of −10%, we would consider ZebraScope noninferior to URF-V. The 95% CI of the 1-month SFR difference between the two groups was −5.95% to 25.01%, meeting the criteria for noninferiority of ZebraScope to URF-V. During surgery, the ureteroscopic basket was used in 92.06% of patients in the trial group and 82.54% of patients in the control group, and the difference was not significant. The high-quality rate of images and eligible rate of operability of f-URS were 100% in both groups (95% CI: −5.27 to 5.35). The lower limit of the CI (−5.27) was greater than the noninferiority margin of −10%, meeting the criteria for noninferiority of ZebraScope to URF-V.
Surgical Outcomes Comparison of the Efficacy and Safety Between a Single-Use Digital Flexible Ureteroscope (Trial Group) and a Reusable Digital Flexible Ureteroscope (Control Group)
AE, adverse event; ARDS = acute respiratory distress syndrome.
The mean operative times were 42.97 and 41.63 minutes in the trial and control groups (p = 0.687). The mean hemoglobin drops were 7.61 and 7.08 g/L in the trial and control groups (p = 0.760). The mean lengths of hospital stay were 7.71 and 8.19 days in the trial and control groups, respectively (p = 0.430). The mean lengths of postoperative hospital stay were 2.03 and 2.06 days in the trial and control groups (p = 0.878).
Safety
Postoperative complications occurred in three (4.76%) patients in the trial group and in one (1.59%) patient in the control group (p = 0.310). The AE rates were 38.57% and 39.71% in the trial and control groups, respectively (p = 0.709). The SAE rates were 3.17% and 4.76% in the trial and control groups, respectively (p = 0.648). AEs included hematuria, lower urinary tract symptoms (LUTS), fever, lung infection, blood electrolyte disorder, and nausea. SAEs included ureteral stent migration, acute renal failure caused by obstruction, and acute respiratory distress syndrome.
Discussion
Treatment recommendations for urolithiasis have shifted to endourologic procedures such as URS and PNL. 5 The SFR of f-URS is equal to that of PNL for stones ≤2 cm 14,15 and superior to that of SWL. 16,17 The initial purchase cost, maintenance cost, performance degradation, and poor durability remain significant issues associated with both fiber optic and URF-V use. 18 –20 Thus, several single-use f-URS devices have been introduced in the past several years (e.g., Polyscope™, SemiflexM, FlexorVue™, Neoflex™, LithoVue™, and UscopePU3022). 21,22 Since the first single-use digital f-URS, LithoVue (Boston Scientific, Marlborough, MA) was introduced to the European market in October 2015 23 and launched in the United States in January 2016, 12 urologists have paid increasing attention to the applications of single-use f-URS because of its similar SFR compared with reusable f-URS. 10 –12
However, there are still a lack of clinical data comparing the efficacy and safety between single-use and URF-V. We designed and conducted a parallel RCT comparing the single-use digital f-URS (ZebraScope, Happiness Workshop) with a URF-V (Olympus). The main reasons why we selected the Olympus digital f-URS URF-V as the control to assess noninferiority are as follows: (1) URF-V can offer better observation, maneuverability, and deflection ability than reusable fiber optic f-URS 24,25 and (2) URF-V is widely used in clinical practice.
Our study showed that single-use digital f-URS is comparable with URF-V. A Nitinol basket was used in 92.06% of patients in the trial group and 82.54% of patients in the control group, which indicated that, in this study, single-use digital f-URS was superior enough in terms of the bidirectional maximal deflection with the laser fiber and Nitinol basket in the working channel. Once the UAS was inserted effectively, all the target stones could be found and handled.
A high operative rate is closely linked with the experience of the surgeon. Similarly, the high-definition images and the superior operability of digital f-URS play important roles. The 1-month SFR was higher in the trial group than in the control group (77.78% vs. 68.25%). Usawachintachit et al. 12 evaluated clinical outcomes of single-use f-URS (LithoVue) compared with those of reusable fiber-optic ureteroscopy in 78 patients, and the results showed that the 3-month SFR of LithoVue was 60%, which is lower than the present study. Mager et al. 26 reported a higher SFR for single-use f-URS than the present study. However, in Mager's study, the SFR was assessed intraoperatively by the surgeon's endoscopic and fluoroscopic views. The error of this method to evaluate SFR is unavoidable. In our study, the SFR of single-use f-URS is high, which is related to the high-definition images and the superior operability.
Inferred by former research, 4 the use of single-use f-URS is considerably less expensive. Hennessey et al. 4 conducted an analysis of 234 procedures with 7 new Olympus URF-V URSs and revealed that 15 URSs were damaged. The total repair costs were 115,224 United States dollar (USD), and the mean cost per case was 492 USD. Including the purchase cost and the cleaning and repair costs, the total cost of 28 procedures using a reusable f-URS was 35,425 USD. A cost analysis 4 showed that if a single-use f-URS device is priced at 850 USD, considerable costs would be saved; therefore, this study suggested that switching to a single-use URS would make sense from an economic point of view. However, an economic evaluation was not performed in our study because all the patients recruited in the study received free f-URS. A health economic evaluation will be performed in our future research.
Furthermore, use of single-use f-URS may improve work efficiency and reduce the risk of cross-infection because it does not need to be sterilized. Sterilization of reusable f-URS requires personnel, time, and specialized equipment, and there is a risk of cross-infection in the case of failed sterilization.
This study has several limitations. First, an economic evaluation was not performed in our study, but it will be assessed in our future research. Second, the efficiency of ZebraScope should be assessed in a larger cohort. In addition, this study focuses only on ordinary patients and does not address other special situations, such as pregnant women, infants, and horseshoe kidney patients.
Conclusion
Our study demonstrates that both single-use digital f-URS (ZebraScope) and URF-V are safe and feasible surgical options in the treatment of stones <20 mm. ZebraScope appears to be at least noninferior to URF-V. We recommend single-use digital f-URS as an alternative to URF-V.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study is supported by the National Natural Science Foundation of China (NSFC: 81874088), the Fundamental Research Funds for the Central Universities (lzujbky-2018-kb14), Science and Technology Project of Tianjin (17ZXMFSY00060), the Education Commission Research Project of Tianjin (2017KJ208), and the Key Laboratory Fund Project of the Second Hospital of Tianjin Medical University (2017ZDSYS14).