
Abstract
Introduction:
GreenLight laser vaporization of the prostate (photoselective vaporization of the prostate [PVP]) is a safe and effective procedure for Benign Prostatic Hyperplasia. Long-term results and advantages of PVP in patients with large and symptomatic prostate are still under evaluation.
Materials and Methods:
In a multicenter experience, patients who underwent standard or anatomical PVP were retrospectively reviewed. Patients with follow-up >12 months were divided into two groups based on prostate volume (<100 cc vs ≥100 cc). Pre- and perioperative data, as well as postoperative results and complications, were recorded after 3, 6, and 12 months and then annually.
Results:
One thousand and thirty-one patients were eligible, 916 of these had a prostate volume of <100 cc and 115 ≥ 100 cc. Median follow-up period was 25.0 months (interquartile range [IQR] 16.5–35.0) and 16.0 months (IQR 12.0–24.0) in ≥100 and <100 groups, respectively. No difference was found in terms of catheterization time, postoperative stay, and postoperative acute urine retention. Patients with prostate ≥100 required longer operative time (75 vs 55 minutes), lasing time (41.7 vs 24.9 minutes), and higher energy used but lower energy density. Patients with prostate ≥100 had a higher incidence of early (50.4% vs 35.7%) and late complications (21.7% vs 12.8%) and early urge/incontinence symptoms (40.9% vs 29.3%). No statistically significant differences were found for the maximum urinary flow (Qmax) and International Prostate Symptom Score (IPSS) results between the two groups. The reintervention rate in ≥100 group was 3.5% vs 2.3% in <100.
Conclusions:
In the midterm follow-up, GreenLight PVP guarantees the same results in different prostate volume groups. Early and late complications are more frequent in large prostates.
Introduction
Since 1997, when the prototype of a 60 W continuous-wave Very High Power (VHP)™ laser system was first used, two additional Green Laser devices have been introduced, the 80 W Potassium Titanyl Phosphate (KTP) and the 120 W high-performance system (HPS)™ Lithium Triborate (LBO). 1
These three laser systems differ in maximum power output and fiber design, and this evolution has been researched to allow higher and faster tissue ablation and lower fiber degradation. 1 Nowadays, GreenLight laser photoselective vaporization of the prostate (PVP) is a consolidated and safe technique for Benign Prostatic Obstruction (BPO). Several articles have reported long-term results with the 80 W KTP and the 120 W LBO, documenting absence of inferiority compared to Transurethral Resection of the Prostate (TURP) in terms of International Prostate Symptom Score (IPSS) and peak urinary flow rates, with lower transfusion requirements, shorter catheterization time, and hospital length of stay in favor of PVP, while reoperation rates and operation time are in favor of TURP. 1
The introduction of the 180 W LBO crystal GreenLight Xcelerated Performance System (XPS)™ (American Medical System-AMS, Minnetonka, MN) with a new 532 nm wavelength, metal-capped and liquid cooled irrigated fiber (Moxy TM fiber), and the development of different PVP techniques (standard photovaporization—PVP, anatomical PVP [aPVP], and GreenLight enucleation of prostate—GreenLEP) have permitted to vaporize more tissues in a shorter time with less fibers used, aiming to reduce re-treatment rates. 1 –3
The European Association of Urology (EAU) guidelines recommend GreenLight laser vaporization of the prostate to men with moderate-to-severe lower urinary tract symptoms (LUTS) as an alternative to TURP with a level of evidence (LE) of 1a (evidence obtained from meta-analyses of randomized trials) for short-term results with the 80 W KTP laser and for mid-term results with the 120 W and of LE-1b (evidence obtained from at least one randomized trial) with the 180 W LBO laser. 4 Conversely, for patients affected by large and symptomatic prostates, long-term functional results and reoperation rates after PVP performed with the 180 W LBO laser are mainly based on retrospective data. 1,5 –10
Based on these considerations, we decided to analyze a large multicenter cohort of 1031 patients to evaluate complication rates and functional outcomes in patients with BPO treated by 180 W LBO laser according to prostate volume.
Materials and Methods
We retrospectively reviewed cases undergoing standard or aPVP in a multi-institutional prospectively collected database between September 2011 and October 2017 using the 180-W XPS GL system for BPO. The study involved several surgeons with consolidated experience in GreenLight. Informed consent was obtained from all individual participants included in the study. This study and all related procedures have been performed in accordance with the Declaration of Helsinki. Patients with history of prostate cancer, neurogenic bladder disease, previous prostate surgery, as well as those who underwent GreenLEP or contemporary urethrotomy, treatment of bladder stones, and with incidental bladder tumors, were excluded. Surgical procedures were performed according to surgeon's preferences, as previously described. 1,3
All the procedures start with visualization of the striated sphincter, the ureteral orifices, and the exclusion of bladder tumors. In standard PVP (sPVP), after the creation of a working space at 5 and 7 o'clock, the prostate is vaporized in a centrifuge way from the prostatic urethra toward the prostatic capsule (inside out). Conversely, in aPVP after the localization of the capsule at the apex of the prostate, the surgeon performs a bilateral incision lateral to verumontanum, and the tip of the resectoscope is used to find the anatomical plane between the prostatic capsule and the adenoma. The dissection plane is followed toward the bladder neck at 6 o’ clock, and the dissection is accompanied by vaporization of the enucleated tissue, which is performed by firing the laser in direction of prostatic urethra (outside in). In both techniques, all the tissues were vaporized, and morcellation was not necessary. 3
All procedures were performed under general or spinal anesthesia. Antibiotic prophylaxis was administered to all patients according to local practice guidelines.
Examined pre-and postoperative factors and intra- and perioperative data include the following: age, American Society of Anesthesiology (ASA) score, prostate volume evaluated with transrectal ultrasound, use of antiplatelet and anticoagulant medications, LUTS therapy and history of catheterization or retention, prostate-specific antigen (PSA) level, IPSS, maximum urinary flow (Qmax), operative time, lasing time, energy used, catheterization time, hospital stay, and re-treatment rate. Energy density was coded as energy used divided by the prostate volume.
All the patients were recalled and underwent an outpatient clinic evaluation at least after 3, 6, and 12 months and then annually. Follow-up was calculated as time from surgery to last visit. During follow-up visit, symptoms score (IPSS), maximum urinary flow (Qmax), and PSA level were recorded. Patient Global Impression of Improvement (PGI-I) was evaluated with PGI-I scale. 11
Complications were collected as early (within 30 postoperative days) or late (after 90 days) and classified according to Clavien–Dindo classification. 12,13 We have considered postoperative frequency and urgency as complications when they prompted additional medical examination or bothered patients. Hematuria requiring application of bladder catheter and irrigation or reintervention or medical examination was also reported. Urinary incontinence was defined as reported incontinence of any degree and type (stress or urge incontinence) if bothersome and impairing patient's quality of life.
Statistical methods
Quantitative variables were summarized as median and interquartile range (IQR). Qualitative data were summarized as frequency and percentage. After stratification according to prostate volume (<100 cc vs ≥100 cc) the Chi-square and the Mann–Whitney U tests tested the statistical significance in proportions and median differences. We relied on a nonparametric model for repeated measurements 14 to test the effect of prostate volume and time on PSA, Qmax, and IPSS. Moreover, we tested the interaction between preoperative prostate volume and time. Box plots graphically depicted the distribution of PSA, Qmax, and IPSS values at each time point (baseline, 6 months, and 12 months). Furthermore, univariable and multivariable logistic regression models tested the effect of prostate size on acute urinary retention and early and late complication rates.
All the multivariate logistic regression models were adjusted for age, baseline PSA, BPO/LUTS therapy, antiplatelet/anticoagulant therapy, surgery type, and history of catheter indwelling prior surgery. All tests were two sided, and the level of statistical significance was set at p < 0.05. Analyses were performed using the R software environment for statistical computing and graphics (version 3.5.1;
Results
A total of 1031 patients were eligible for the study analysis. Nine hundred and sixteen of these had a prostate volume <100 cc, and 115 patients had a prostate volume ≥100 cc. The median prostate volume in <100 group was 55.0 cc (43.0–70.0) vs 112.0 cc (100.0–130.0) in ≥100 group (p < 0.001). Patients with large prostate volume had more frequently a history of indwelling catheter (27% vs 15%, p < 0.001). Patients with prostate ≥100 cc required longer operative times (75 vs 55 minutes, p < 0.001), longer lasing times (41.7 vs 24.9 minutes, p < 0.001), and higher energy used (390 vs 205 kJ, p < 0.001) but lower energy density (3.3 vs 4.1 kJ/mL, p < 0.001). Age, catheterization time, and postoperative hospital stay were similar between the two groups (Table 1).
Patients' Preoperative and Intraoperative Characteristics Stratified According to Prostate Volume
Values are n (%) or median (IQR).
Mann–Whitney U test prostate volume ≤100 vs ≥100 cc.
Chi-squared test.
5-ARI = 5-alpha reductase inhibitors; ASA = American Society of Anesthesiology; BPH = Benign Prostatic Hyperplasia; IPSS = International Prostate Symptom Score; IQR = interquartile range; LUTS = lower urinary tract symptoms; PVP = photoselective vaporization of the prostate; TRUS = transrectal ultrasound.
According to Clavien–Dindo classification, the most common early complications were Grade I in both groups (93.1% in ≥100 cc and 87.8% in <100 cc), and similar rates between groups were recorded (Table 2). The most frequent early complication was burning urination (13.2%), while the most frequent late complication was storage symptoms with de novo urgency (Table 3). Patients in ≥100 group had a higher risk of developing early (OR: 1.8, 95% CI: 1.2–2.9, p = 0.009) and late complications (OR: 2.2, 95% CI: 1.3–3.9, p = 0.004) (Table 4).
Main Outcomes After Photoselective Vaporization of the Prostate Stratified According to Prostate Volume
Values are n (%) or median (IQR).
Mann–Whitney U test prostate volume <100 vs ≥100 cc.
Chi-squared test.
Percentage refers only to the group of patients who experienced early complications.
Early and Late Complications Stratified According to Prostate Volume
MACE = Major Acute Cardiovascular Event.
Multivariable Logistic Regression Models Predicting Acute Urinary Retention And Overall Early and Late Complication Rates in Patients with Prostate Volume <100 cc vs ≥100 cc (Reference: Prostate Volume <100 cc)
All the models were adjusted for age, baseline PSA, BPH/LUTS therapy, antiplatelet/anticoagulant therapy, surgery type, and history of catheter indwelling prior surgery.
PSA = prostate-specific antigen.
When analyzing functional results after surgery, no statistically significant differences were found for the Qmax and IPSS between the two groups (Table 5). All three parameters (PSA, Qmax, and IPSS) improved overtime (Figs. 1 –3). However, despite PSA being higher in patients with large prostate, the magnitude of decrease overtime was similar in the two groups (p-value for interaction = 0.089). Conversely, even if Qmax and IPSS improved overtime in both groups, the Qmax increase and IPSS decrease were larger in patients with large prostates (p-values for interaction = 0.022 and 0.013, respectively) (see Table 5).
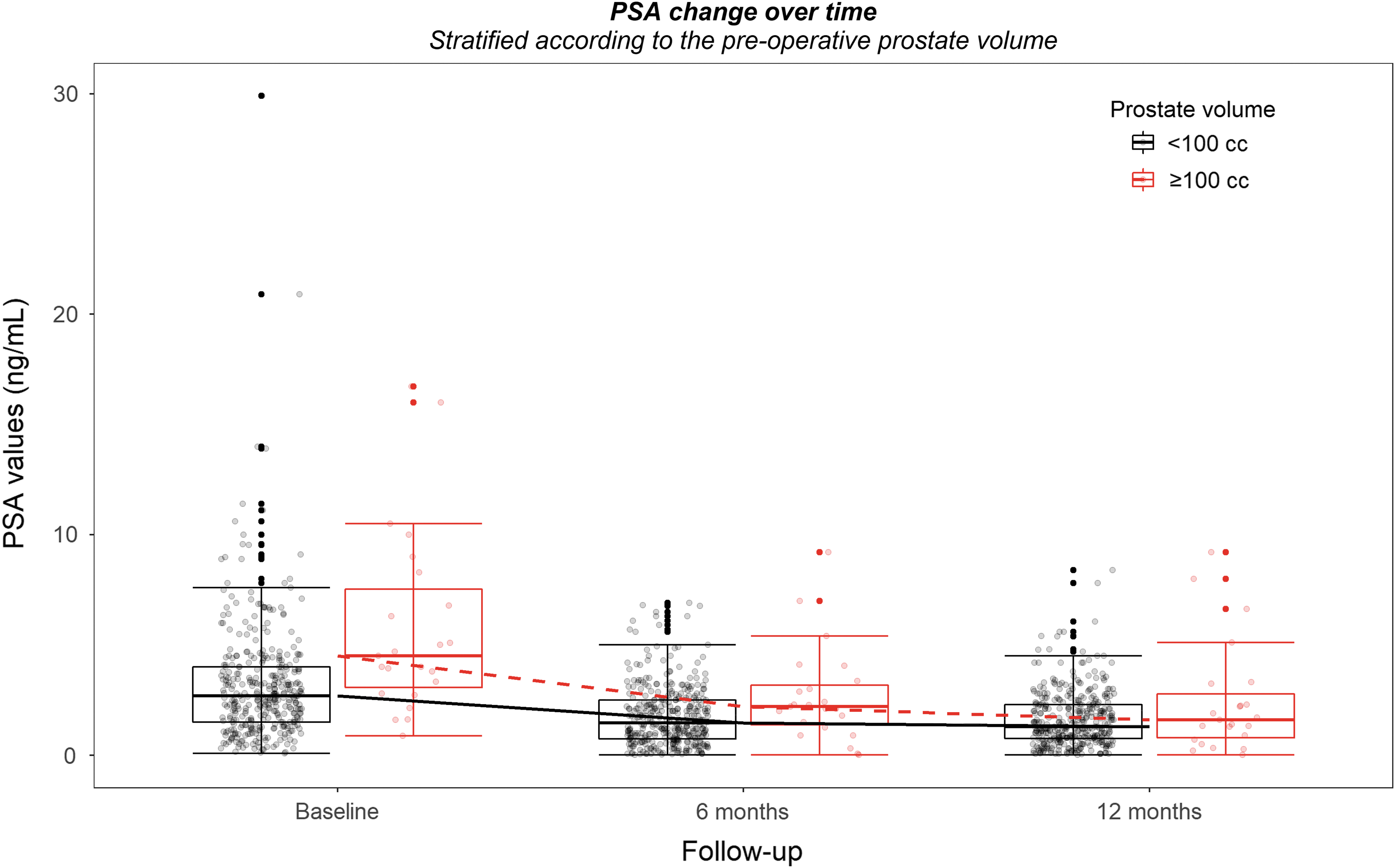
Box-whiskers graphs of baseline, 6 months, and 12 months of PSA in large and small prostate groups. Box-whiskers plots show the 25th and 75th percentile range (box) with 95% confidence intervals (whiskers) and median values (transverse lines in the box). PSA = prostate-specific antigen.
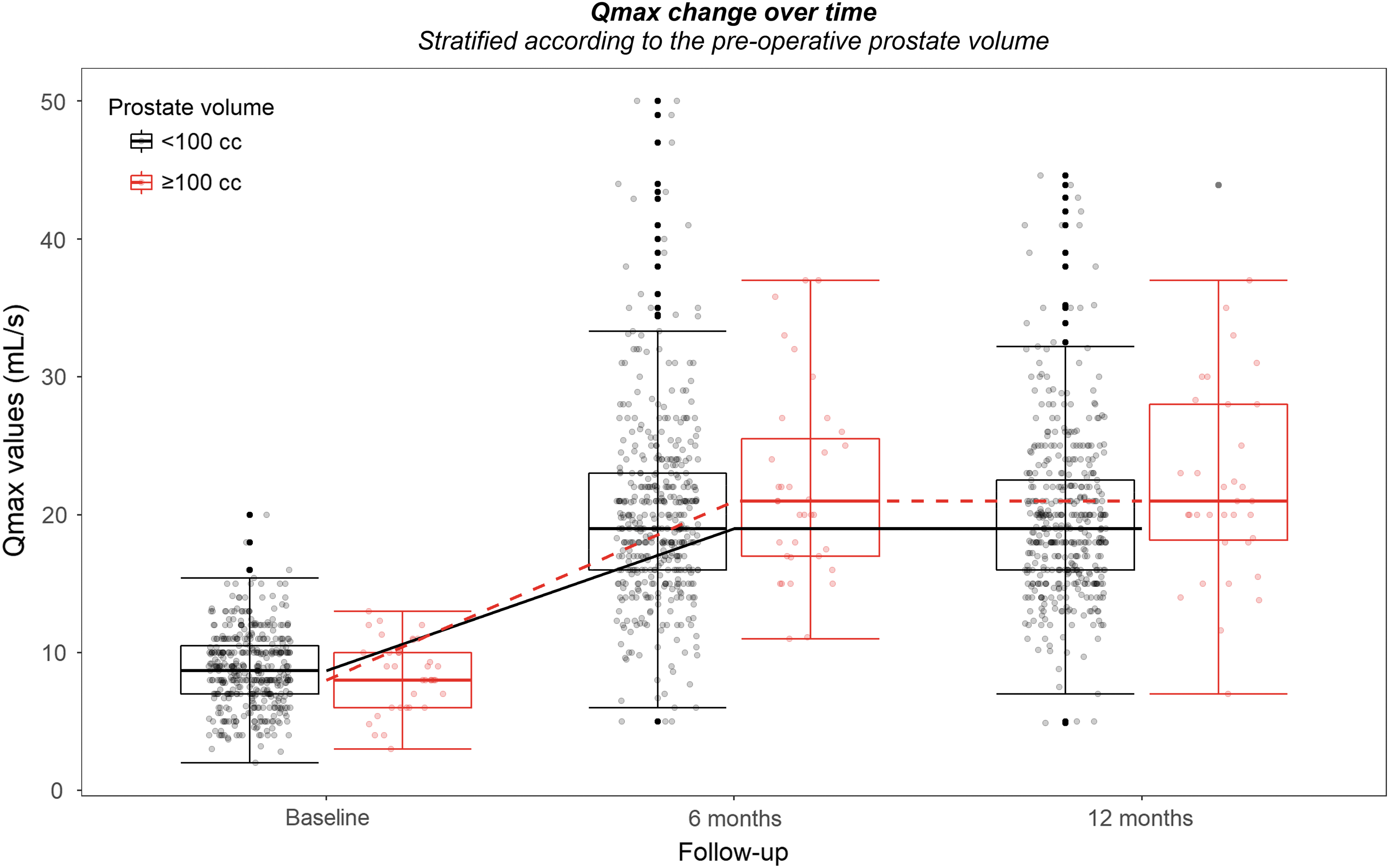
Box-whiskers graphs of baseline, 6 months, and 12 months of Qmax in large and small prostate groups. Box-whiskers plots show the 25th and 75th percentile range (box) with 95% confidence intervals (whiskers) and median values (transverse lines in the box). Qmax = maximum urinary flow.
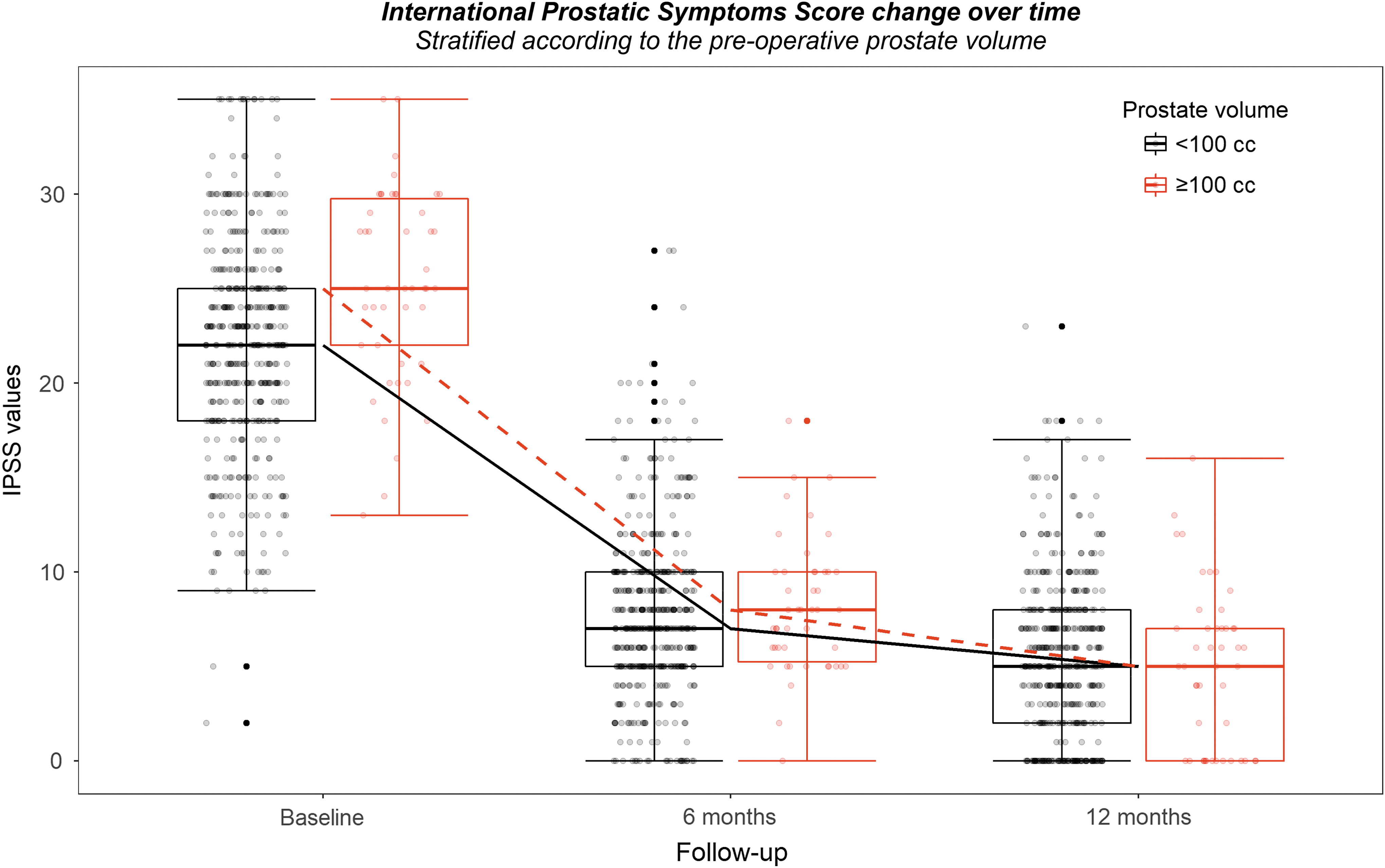
Box-whiskers graphs of baseline, 6 months, and 12 months of IPSS in large and small prostate groups. Box-whiskers plots show the 25th and 75th percentile range (box) with 95% confidence intervals (whiskers) and median values (transverse lines in the box). IPSS = International Prostate Symptom Score.
Median Values (Interquartile Range) of Prostate-Specific Antigen (ng/mL), Maximum Urinary Flow (mL/second), International Prostate Symptom Score Stratified According to the Prostate Volume with the p-Values Derived from Ranked Based Model for Differences Between the Prostate Volume, Follow-Up Time Points, and Interaction Prostate Volume and Follow-Up Time
Boldface indicates statistically significant values.
Qmax = maximum urinary flow.
Discussion
In general, patients with prostate volumes higher than 100 cc undergo either simple prostatectomy (open laparoscopic or robotic) or endoscopic enucleation procedures. 4 Simple prostatectomy is the most invasive procedure to treat BPO but it has longer functional results and it does not require dedicated instruments. Management of large prostate volumes with laser offers the major advantages of this technology (shorter catheterization and hospitalization time and fewer blood transfusion rates). 4,7
However, the approach to large prostate volumes requires experience and relevant endoscopic skills. The long learning curve of the enucleation technique and the requirement of further materials for morcellation are some of the arguments to explain the slow dissemination of this procedure in urologic practice. In contrast with other laser techniques (Holmium and Thulium), the GreenLight Laser allows to adapt the surgical strategy (pure enucleation vs standard or anatomical vaporization) during a single procedure without modifying the functional outcomes and the complication rates. 3,15,16
In this study no difference was made between patients who underwent sPVP or aPVP based on our previous multicenter experience in which we did not find any difference in terms of functional results and complication rates between the two techniques. 15 In the last years several retrospective studies evaluated the safety and outcomes of Green Laser in large prostate volumes. 7,17 –26 The commonest criticisms against the use of XPS in this clinical scenario are the absence of long-term follow-up, the retrospective nature of the available literature data, and the reportedly higher re-treatment rates compared to Holmium laser enucleation of the prostate (HoLEP). Our series, with a mean follow-up of 25.0 months (IQR 16.5–35.0) for prostate with a volume ≥100 cc, is one of the longest so far reported in the literature. The reintervention rate in the ≥100 group was 3.5% vs 2.3% in prostate <100 cc. These data are slightly better than those reported by the Goliath study with a 24-month re-treatment rate of 9% 27 and worse than those reported by Ajib and colleagues 10 with a re-treatment rate of 1.1% in a series of 370 patients with a mean follow-up of 59.4 months and a mean prostate volume of 48.6 and 78.8 cc, respectively.
If we consider only large prostate series, re-treatment rates range from the no re-treatment at 12 months reported by Altay and colleagues, 18 1.2% at 24 months by Hueber, 19 and 2.9% by Stone 20 up to 13.2% by Meskawi and colleagues 22 and 6% for 200 cc prostate and 9% for 100 to 200 cc (mean follow-up: 15.9 months) of the same reviewed multi-institutional series. 24 Only five studies compared the results of photoselective vaporization in large prostate cases: <80 vs ≥80 cc, 19 ≥200 cc vs 100 to 200 cc, 24 PVP vs en bloc enucleation (GreenLEP), 21 sPVP vs aPVP, 25 and simple prostatectomy vs PVP. 26
Despite the different results of re-treatment rates reported in these articles, all the authors (including us) agree with the greater operative and lasing time in large prostate undergoing PVP. Similarly, there are no differences in hospital stay and midterm functional results.
Valdivieso and coworkers 24 and Hueber and coworkers 19 reported a higher conversion rate to TURP. Hueber 19 also reported a longer catheterization time in prostate larger than 80 mL, conversely Misraï and colleagues 23 described, for large prostate, shorter catheterization time in PVP than in GreenLEP. Interestingly, Lanchon and colleagues reported a higher rate of recatheterization and rehospitalization after PVP compared to open simple prostatectomy. Our results highlight the higher risk to develop early and late complications of large prostate, as well as early urge incontinence symptoms, similar to Hibon and coworkers. 25
In our series early and late storage symptoms/De novo urgency are 22.2% and 4.8%, respectively. These data are in line with the results reported in the literature. The groups of Zorn and Misrai 10 reported irritative voiding symptoms of 18.8% at 3 months. This incidence dropped to 8.46% at 1 year. In a series of large prostate treated with GreenLaser irritative symptoms are described in 10.2% patients. 22 In agreement with previous series, we confirm no differences in catheterization time.
In our series, the PSA drop, used as a proxy of removed tissue, is 51.1% and 64.5% in ≥100 vs 44.4% and 51.8% in <100 group at 6 and 12 months, respectively. The decrease is statistically significant. This reduction is greater in ≥100 (p = 0.013) and continues overtime (p < 0.001), but the interaction between prostate volume and follow-up time is not statistically significant (p = 0.089), implying that despite the larger amount of tissue removed the magnitude of change is not different between large and small prostate volume: the effectiveness is similar in the two groups.
In the literature the cutoff of 50% of PSA reduction is established as the surgical goal to reduce re-treatment risk. 28 Probably the PSA drop recorded in our centers (64.5%) at 12 months might explain our low re-treatment rate (3.5%). Qmax and IPSS improve after surgery, with no difference between the two groups (p = 0.097 and p = 0.207, respectively), and with improvement overtime (p < 0.001). At 12 months Qmax increased by 118.3% in <100 and 162.3% in ≥100. This result might correlate with the major volume of tissue vaporized in large prostate, which is linked to an efficient vaporization and an improvement of urodynamic performances.
Even if Valdivieso and coworkers reported a 5 kJ/cc energy density to achieve 80% of PSA reduction at 24 months in prostate <100 cc (this target in larger prostate might be time- and fiber consuming), a 3 to 4 kJ/cc cutoff has been proposed as the minimum threshold to obtain adequate adenoma vaporization. 28 In the ≥100 group the mean energy density was 3.3 KJ/cc (IQR 2.3–4.2), less than in <100 group, where it was 4.1 kJ/cc (IQR 2.7–5.4) (p < 0.001). The lower energy density in the ≥100 group might be explained by the greatest use of aPVP (63%), as already described. 15
There are some limitations in this study: the retrospective design, the involvement of several surgeons with different level of expertise, the heterogeneity between centers to report and manage pre- and postoperative events, and the absence of number of fibers used per procedure. Another confounding factor might be the multicenter nature of this study involving different surgeons with variable surgical experience. Although all these aspects might represent limitations, from our perspective they strengthen the general perception that laser is a safe and reliable procedure which can be adopted also by young surgeons. 29,30
Conclusions
In the midterm follow-up, GreenLight PVP using the XPS-180 W is safe and effective in treating patients with prostate volumes ≥100 cc compared to prostate volumes <100 cc. Even if early and late complications are more frequent in large prostate, the improvement overtime in terms of Qmax and IPSS is greater than in small prostate. This study confirms the flexibility and reliability of GreenLight Laser technique. Nevertheless, a longer follow-up period is necessary to better clarify the re-treatment rate and effectiveness of GreenLight in large prostates.
Footnotes
Author Disclosure Statement
P.D., L.R., C.D., G.F., and L.C. do surgical tutorship for AMS and received honoraria for their tutorship. All other authors have no competing financial interests that exist.
Funding Information
No funding was received for this article.