
Abstract
Purpose:
To conduct a randomized, controlled, multicenter study that could compare the efficacy and stent-related symptom scores between 5F and 6F ureteral stents after ureteroscopic lithotripsy (URS).
Materials and Methods:
From September 2017 to April 2018, 110 patients having a unilateral ureteral stent after URS were prospectively enrolled from three different tertiary medical centers. The patients were randomly assigned to a 5F or 6F ureteral stent group. A ureteral stent symptom questionnaire (USSQ) was administered to patients 2 or 3 weeks after stent placement. The USSQs were used to compare body pain and urinary symptom scores between the two groups.
Results:
There was no statistically significant difference in body pain between the 5F and 6F ureteral stent groups. There was also no difference in analgesic usage between the groups. However, patients with 5F ureteral stents expressed significantly fewer urinary symptoms. Postoperative hydronephrosis was not observed in either group.
Conclusions:
Ureteral stents are associated with various morbidities and impaired quality of life. This study demonstrated that 5F ureteral stents may cause fewer urinary symptoms when compared with 6F ureteral stents. Therefore, the placement of ureteral stents with smaller diameters may reduce stent-related urinary symptoms.
Introduction
Although ureteral stents are commonly used in endourology, especially after ureteroscopic procedures, stent-related symptoms are still a major concern. 1 –3 A ureteral stent can usually cause flank or bladder pain, lower urinary tract symptoms, and gross hematuria, resulting in deterioration of a patient's quality of life. Many initiatives and studies have been launched in an effort to reduce these stent-related symptoms. 1 –5 Recently, several studies have suggested that stent position and the material of the stent can influence the severity of stent-related symptoms. 1,3,6 This indicates that the circumstances under which the stent and bladder mucosa make contact can cause or aggravate bladder irritation. Therefore, we hypothesized that stents with larger diameters cause more pain than those with smaller diameters.
Researchers compared stent-related pain and urinary symptoms between 6F and 4.8F ureteral stents in the early 2000s, but they did not use a validated ureteral stent-related questionnaire, such as the ureteral stent symptom questionnaire (USSQ), in their studies. 7,8 More recently, Cubuk et al. performed a prospective, randomized, controlled trial to compare stent-related symptoms between 4.8F and 6F ureteral stents by using a USSQ. 9 However, these studies did not control other stent-related factors, which can influence stent-related symptoms such as stent length, material, and position. Therefore, we compared the stent-related symptoms between 6F and 5F ureteral stents while controlling other stent-related factors. We also evaluated the efficacy of the 5F ureteral stent in terms of urine drainage. This analysis relied on a multicenter-based, randomized, controlled trial that used a validated Korean version of the USSQ. Patients who underwent ureteroscopic lithotripsy (URS) were the focus of this evaluation.
Materials and Methods
Patient enrollment
This study was approved by the local Institutional Review Board (2017-05-005) and included 110 patients (37 patients from 2 hospitals, each, and 36 patients from 1 hospital) who underwent URS at 3 tertiary general hospitals. They were prospectively enrolled after randomization between September 2017 and April 2018. Written informed consent was received from all patients. The sample size of the enrolled patients was calculated based on a previous study investigating visual analog scale (VAS), since the primary endpoint was a ureteral stent-related pain score. 10 Assuming a similar treatment effect, a log-rank test with a two-sided significance level of 0.025 had an 80% power to detect differences between the two groups, with a sample size of 50 in each group. After considering a maximum dropout rate of 10%, 55 patients from each group were enrolled.
To meet the inclusion criteria, the participants had to be adults aged 18 years or older and had to have undergone unilateral semi-rigid URS or retrograde intrarenal surgery (RIRS) with planned ureteral stent insertion for urinary tract stones. Exclusion criteria included pregnancy or breastfeeding; involvement in bilateral procedures; concomitant use of alpha-blockers, anticholinergics, calcium channel blockers, and beta-3 agonists; history of preoperative urinary tract infection within 2 weeks before surgery; comorbid urologic malignancy; comorbid urologic anatomical abnormalities, such as ureteral stricture; and 12 or more points on the International Prostate Symptom Score (IPSS).
Study design
This study was a prospective, single-blind, randomized, multi-center trial. Eligible patients were randomly divided into 5F and 6F ureteral stent groups. Information on the randomization process was secured and managed by Keimyung University Dongsan Medical Center.
URS or RIRS was performed under spinal or general anesthesia by using a semi-rigid or flexible ureteroscope. After lithotripsy, the same type of 5F or 6F ureteral stent (Polaris Ultra; Boston Scientific, Natick, MA) was inserted for all patients in their respective groups. The length of the stent used was determined according to the height of each patient (height <175 cm: length of stent, 22 cm; height >175 cm: length of stent, 24 cm), which followed the results of a previous Asian study. 11 The proximal curl of the ureteral stent was placed in the renal pelvis. If the placement of the distal curl crossed the midline of the bladder at postoperative kidney, ureter, and bladder radiograph (KUB), the patient was excluded from the study because the stent position could negatively affect stent-related bladder irritation symptoms. 3
The following discharge medications were prescribed for both groups: 3 days of oral antibiotics and on-demand analgesics (diclofenac 75 mg) for 7 days. Alpha-blockers or anticholinergics, which can affect stent-related symptoms, were not used in any patients. All patients were asked to record the amounts of analgesics they used. The indwelling time of the ureteral stent was 2–3 weeks in all patients. Follow-up examinations were performed on the day of stent removal. A kidney ultrasound was conducted to ensure the absence of hydronephrosis before stent removal for the purpose of evaluating the efficacy of the ureteral stent. Patients also completed the Korean version of the USSQ and reported the total amount of analgesic that they used.
The primary endpoints were urinary symptoms and body pain scores recorded by the USSQs. The secondary endpoints were the ratios between hydronephrosis, analgesics usage, general health, work performance, sexual function, and global quality of life scores recorded by the USSQs.
Statistical analysis
Continuous variables were compared with a paired t-test or a nonparametric Wilcoxon rank-sum test, and categorical variables between the 5F and 6F ureteral stent groups were assessed by using the chi-square test for comparisons. Continuous data are presented as the mean ± standard deviation. Statistical analyses were performed by using SPSS 22.0 (IBM Co., Armonk, NY), and p < 0.05 was considered significant.
Results
Of the 110 patients who were randomly assigned to the 5F and 6F groups, 4 patients in the 6F group were excluded from the final analysis because the distal curl of the ureteral stent crossed the midline of the bladder at postoperative KUB. Therefore, 55 patients in the 5F group and 51 patients in the 6F group completed the study (Fig. 1). Patient characteristics such as mean age, male to female ratio, body mass index, mean stone size and number, radio-opacity of stones, and operation types were not statistically different between the two groups (Table 1). Patients with stones on the left side were more common in the 5F group (p = 0.021).
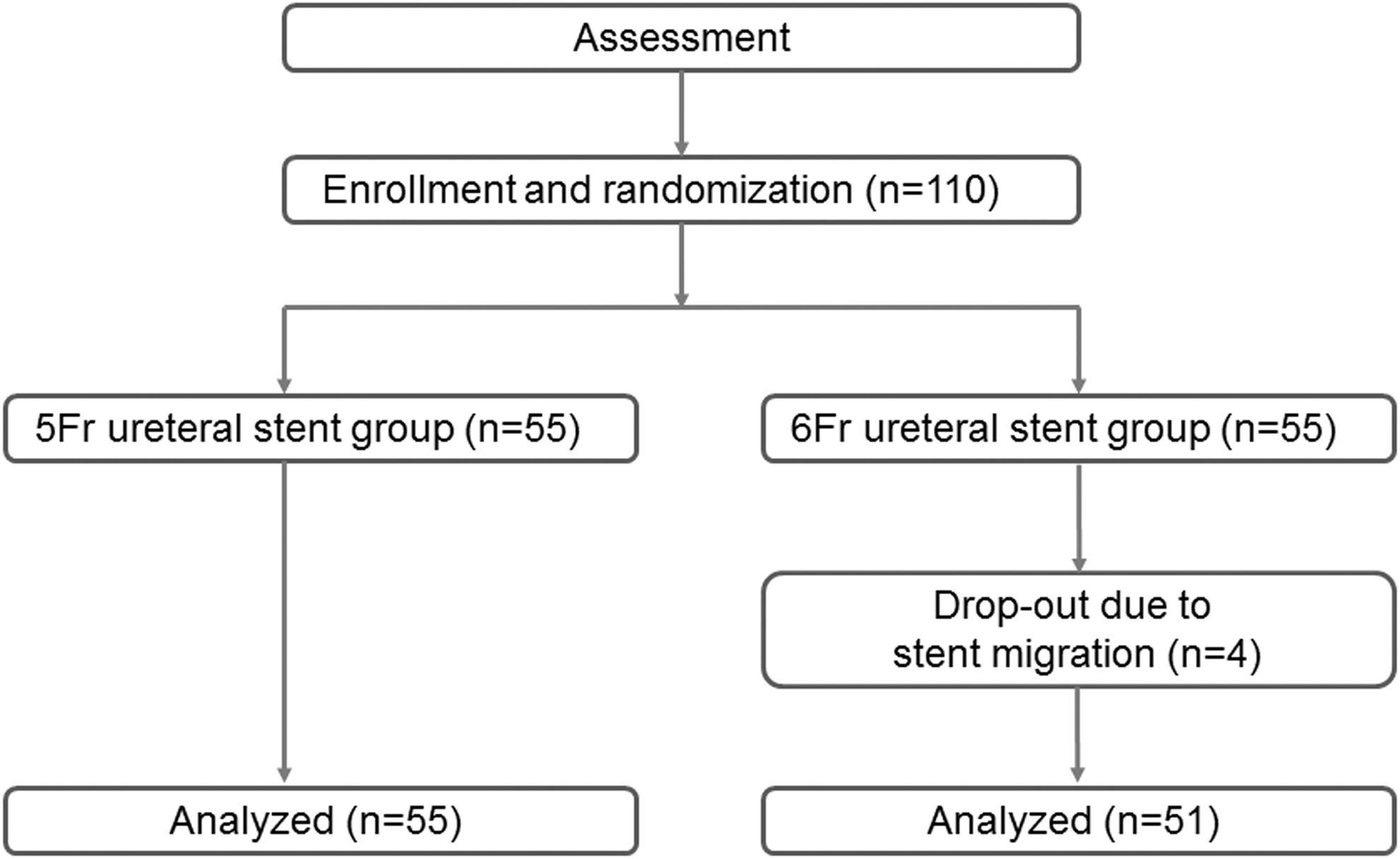
The algorithm used in this study.
Patients' Demographic Data and Stone Characteristics
BMI = body mass index; RIRS = retrograde intrarenal surgery; URS = semi-rigid ureteroscopic lithotripsy.
The urinary symptom score captured by the USSQs was significantly lower in the 5F group when compared with the 6F group (p = 0.014). Meanwhile, other sub-scores recorded by the USSQs, such as body pain, general health, work performance, and stent-related additional problems, were not statistically different between the two groups. Also, the overall pain score, number of pain sites, use of analgesics, and satisfaction with the ureteral stent were not significantly different between the two groups (Table 2). To confirm the efficacy of each ureteral stent, an ultrasound of the kidney was performed on each patient before stent removal, and postoperative hydronephrosis was not observed in any patients.
Comparison of Ureteral Stent-Related Symptoms Between 5F and 6F Stent Groups
Range of score: 1–7, 1-very satisfactory, 7-terrible.
USSQ = ureteral stent symptom questionnaire; VAS = visual analogue scale.
Discussion
Since ureteral stents can cause stent-related symptoms and deteriorate the quality of life of patients even with a short indwelling time, many researchers have tried to find and reduce the causative factors of stent-related symptoms. Although the exact mechanism(s) of stent-related symptoms is still not well known, several factors such as ureteral spasms, urinary reflux attributable to a ureteral stent, and irritation of the trigon have been proposed as causes of stent-related discomfort. 12
Most studies examining ureteral stent-related morbidity have focused on stent design, materials, position, presence of string, or administration of medicine to reduce stent-related symptoms. 1 –3,5,6,12 –18 These studies have shown that specially designed stents 1 ; correct placement of the stent 3 ; pharmacologic agents such as alpha-adrenergic blockers, 14,16 anticholinergic agents, 14,16,17 phosphodiesterase-5 inhibitors, 13 and beta-3 agonists 12 ; and absence of string 18 can relieve urinary symptoms and body pain after stent indwelling.
However, these strategies did not fully improve all stent-related symptoms, and some studies did not confirm the positive effects expected from some pharmacologic agents. 2,15 Therefore, other strategies to reduce stent-related discomfort should be considered. Based on proposed mechanisms of stent-related symptoms, reducing areas of contact between the bladder mucosa and the distal curl of the stent may be helpful. Also, reducing the stiffness and decreasing the chance of urinary reflux caused by the stent may be effective at reducing stent-related symptoms. Recently, a novel thermo-expandable ureteral metal stent was developed and used in patients with ureteral strictures. 19 Because this type of metal stent does not have a distal curl, it was expected to decrease bladder irritation and urinary reflux. These positive effects were proven in a comparative study between conventional Double-J stents and thermo-expandable metal stents. 20 However, the use of this metal stent is not recommended in patients with urolithiasis due to its high cost and difficulty of retrieval. Thus, we applied a conventional ureteral stent under the assumption that a ureteral stent with a smaller diameter may reduce stent-related urinary symptoms and/or body pain.
A ureteral stent consists of three parts: proximal curl, shaft, and distal curl. Six French ureteral stents are commonly used in adult patients. The diametric size of the ureteral stent represents the outer diameter of the shaft. Thus, a ureteral stent with a smaller diameter corresponds to a stent with a smaller diametric shaft. Although it was not precisely validated, a ureteral stent with a smaller diameter can be less stiff and may create less pressure inside the lumen of the ureter. In addition, a ureteral stent with a smaller diameter may reduce the degree of vesicoureteral reflux. Therefore, we hypothesized that the 5F ureteral stent would decrease flank or back pain; however, the USSQ body pain score, VAS, and analgesics usage were not statistically different between the 5F and 6F ureteral stent groups in this study. Most commercially available ureteral stents with a smaller size have smaller proximal and distal curl diameter. A stent with a smaller size and a smaller distal curl diameter may result in less contact between the bladder mucosa and stent surface. Therefore, stent-related bladder irritation symptoms may be reduced with a smaller diameter stent. The results of our study also showed that the USSQ urinary symptom score was significantly lower in the 5F ureteral stent group when compared with the 6F stent group. However, several previous studies did not show any differences between 4.8F and 6F ureteral stents in terms of pain and urinary symptoms. 7,8 These studies did not use USSQs to assess patients' stent-related symptoms and other stent-related factors, such as stent length, material, and position, were not controlled. In contrast, a more recent study, which used USSQs, showed that smaller diameter ureteral stents caused less stent-related symptoms and decreased the USSQ score compared with 6F ureteral stents. 9
Even though the 5F ureteral stent should reduce stent-related symptoms, and our study confirmed its beneficial effects, it cannot be used routinely if the stent does not accomplish proper urinary drainage. Also, there is a concern that stents with smaller diameters can migrate more easily. However, stent migration and postoperative hydronephrosis were not observed in any patients from the 5F stent group in this study. This indicates that the 5F ureteral stent can be maintained well during the indwelling time, and it effectively achieved urinary drainage. Also, 5F ureteral stents were slightly tighter during insertion when compared with 6F stents, but it was feasible to place 5F ureteral stents by using 0.035″ guidewire without any problems.
Ureteral stents can also reduce the quality of general health, work performance, and sexual activity. These impairments may be caused by stent-related symptoms, such as body pain and urinary symptoms, as well as by anxiety and decreased self-confidence. Interestingly, Deliveliotis et al. reported that the mean general health index and mean sexual performance score, captured by USSQs, were significantly lower in patients who received alfuzosin during stent indwelling when compared with patients who received a placebo. 21 These results may be due to decreased body pain and urinary symptoms in patients who received alfuzosin. However, stent-related sexual abstinence, general health, and work performance scores were not significantly different between the 5F and 6F ureteral stent groups in our study. This may be due to similarities in body pain between the two groups, although urinary symptoms were less severe in the 5F ureteral stent group.
This study had several limitations. First, most of the cases in this study were not complicated. Thus, we could not confirm the efficacy of 5F ureteral stents in cases of complicated URS such as impacted stones or ureteral stricture. Second, although short-term outcomes of 5F ureteral stents were comparable to 6F ureteral stents in terms of the presence of hydronephrosis during stent indwelling, a lack of long-term follow-up data such as incidence of ureteral stricture is another limitation of this study. Finally, we collected preoperative IPSSs to exclude patients with underlying lower urinary tract symptoms. However, preoperative USSQs were not evaluated in all patients. Measurements from the preoperative USSQs and a comparison of the changes between pre- and postoperative USSQs may be more helpful in identifying the effects of a ureteral stent.
Despite these limitations, this study, to the best of our knowledge, was the first trial to evaluate the impact of 5F Polaris Ultra ureteral stents. It provides the first clinically derived data that identify factors of stent-related symptoms. In future studies involving ureteral stent-induced symptoms, the diameter of the stent as a causative factor as well as medicines, stent design, and materials should be considered.
Conclusions
Ureteral stents are associated with various morbidities and impaired quality of life. This study indicated that 5F ureteral stents may cause fewer urinary symptoms compared with 6F ureteral stents. Therefore, the placement of a smaller diameter ureteral stent can be used to reduce stent-related urinary symptoms. In the future, larger population-based, prospective, double-blind, randomized, controlled trials or a combination study with medicines such as alpha-adrenergic antagonists and/or anticholinergics should be performed to evaluate the effects of 5F ureteral stents and to identify better strategies for treating ureteral stent-related symptoms.
Author Disclosure Statement
No competing financial interests exist.
Footnotes
Funding Information
This research was supported by the Keimyung University Research Grant of 2017.