
Abstract
Introduction:
High-power laser settings are commonly employed for stone dusting techniques. Previous in vitro and in vivo studies have demonstrated that a toxic thermal dose can result from treatment within a renal calix without adequate irrigation. Hence, both laser power and irrigation rate must be considered together to determine safe laser lithotripsy parameters. The objective of this in vitro study was to map parameter safety boundaries and create guidelines for selection of safe laser and irrigation settings.
Methods:
The experimental system consisted of in vitro models simulating ureter, renal calix, and renal pelvis placed in a water bath maintained at 37°C. Temperature was recorded during ureteroscopy with laser activation for 60 seconds. Trials were conducted at strategically selected power levels and irrigation rates. Thermal dose for each trial was calculated based on Sapareto and Dewey t43 methodology with thermal dose >120 equivalent minutes considered to result in thermal tissue injury. A parameter safety boundary was established by plotting the maximal safe power level for each irrigation rate.
Results:
The parameter safety boundary was found to be linear for each scenario with the renal pelvis able to tolerate the highest laser power and the renal calix the least power without injury.
Conclusion:
This study describes the methodology to determine parameter safety boundaries that can be used to guide proper selection of thermally safe laser settings and irrigation rates during ureteroscopy with laser lithotripsy. This work provides a framework to assess the effectiveness of various strategies to control and mitigate thermal dose.
Introduction
The introduction of high-power (100–120 W) holmium laser systems capable of 60 to 80 Hz pulse frequency has dramatically expanded the available settings for laser lithotripsy. 1 In addition to the conventional fragmentation strategy, “dusting” 2 –4 and “pop-dusting” 4 –7 are also possible. With dusting, a stone is eroded to submillimeter particles by translating the laser fiber across the surface of a large stone. With pop-dusting, the laser is activated on a collection of stone fragments in noncontact mode to create a cloud of fragments that randomly pass through the laser focus to produce sand-like particles.
These new lithotripsy modes are effective adjuncts to fragmentation laser lithotripsy and have been shown to shorten operative time. 2 However, the higher powers utilized with these modes present a risk of overheating the caliceal fluid as demonstrated in in vitro and in vivo studies as well as computer simulations. 8 –17 Temperatures in one in vitro study reached 60°C after only 10 seconds of laser activation at 40 W power settings. 8 Even short (<1 second) exposure to this temperature produces cell death and tissue injury. Pathologic thermal injury of the renal parenchyma was grossly apparent in an in vivo porcine study following 60 seconds of laser activation within the collecting system at 40 W power. 9 Moreover, fluid temperature data from previous in vitro studies using the same methods described in this article showed strong agreement with in vivo porcine studies, suggesting that the in vitro system is a good surrogate for in vivo assessment of thermal safety. 8,9
Surprisingly, the assessment of thermal safety in laser lithotripsy has lagged behind the clinical introduction of new high-power laser systems, which do not have automated safety features nor real-time sensing of temperature. Additionally, there is no guidance from industry, professional groups, or regulatory bodies on selection of thermally safe laser settings. Despite the lack of safety features and guidance, a survey in 2015 revealed that 67% of urologists commonly used some form of stone “dusting” technique. 18 Bench studies suggest that increasing irrigation rate can partially control temperature elevation. 8 –12 However, this can only be achieved in certain scenarios, since intrarenal pressures should not exceed 40 cm H2O to minimize risk of infection, sepsis, and hemorrhagic complications from pyelovenous and pyelosinus backflow. 19 –21 Hence, both laser power and irrigation rate must be considered together to determine safe laser lithotripsy parameters. The objective of this study was to demonstrate methods to map the parameter safety boundary and create guidelines for selection of safe laser lithotripsy settings and irrigation rates during ureteroscopy with laser lithotripsy.
Methods
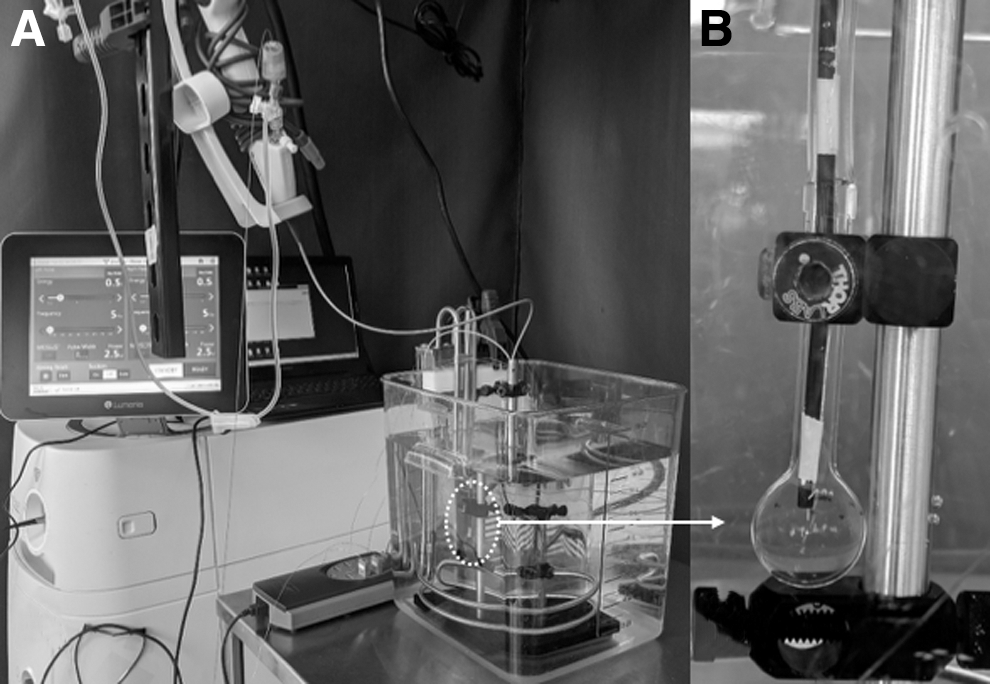
Glass cylindrical tubes (inner diameter 6 mm/length 130 mm/wall thickness 1 mm) terminating in a spherical bulb of 11 or 19 mm inner diameter were used to simulate renal calix and pelvis, respectively. A ureteroscope (LithoVue; Boston Scientific, Boston, MA) was inserted through the model and placed at the middle of the spherical bulbs. The ureter was simulated by placing the ureteroscope within the glass tube 50 mm away from the 19 mm spherical bulb. Experiments were conducted individually for each scenario (renal calix, renal pelvis, and ureter). A 242 μm core laser fiber (Flexiva; Boston Scientific) was introduced through the ureteroscope with the laser fiber tip advanced 5 mm beyond the end of the ureteroscope. Each model was placed in a water bath maintained at 37°C using an immersion heater (Ulanet, Bristol, CT) with 10 mm extending above the water surface (Fig. 1). A wire thermocouple (Omega, Norwalk, CT) was positioned with the measuring portion adjacent to the end of the ureteroscope (Fig. 2).
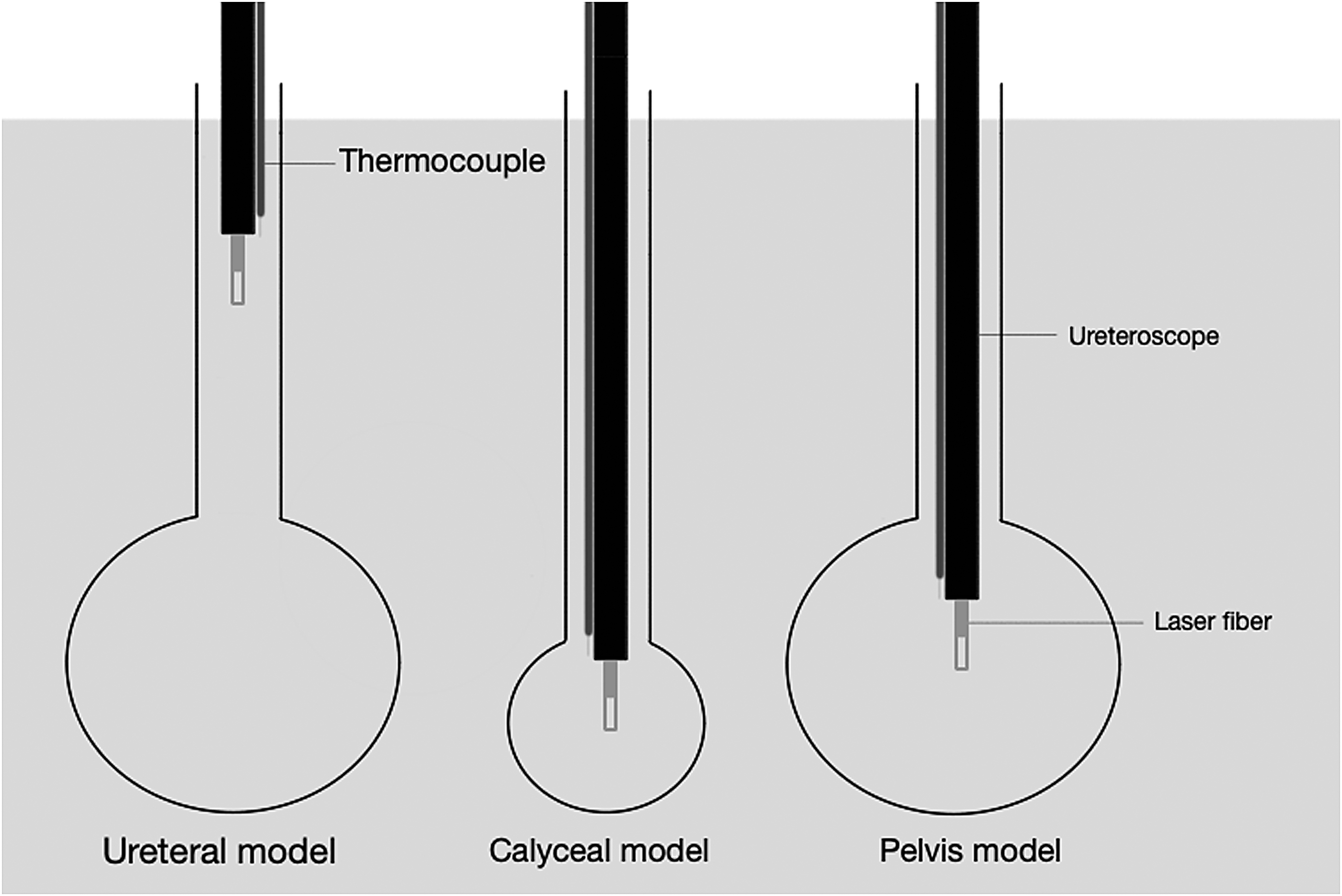
Representation of the ureteral, renal calix, and renal pelvis models and positioning of the ureteroscope, laser fiber, and thermocouple in each model.
Irrigation with room temperature (23°C) deionized water was provided through the working channel of the ureteroscope. The height of the irrigation bag was adjusted to 0, 35, 70, 100, 135, 170, and 200 cm to provide irrigation rates of 0, 5, 10, 15, 20, 25, and 30 mL/min, respectively. Laser energy (range 2.5–50 W) was delivered from a 120 W holmium laser (Pulse 120; Lumenis, San Jose, CA) at different laser settings (Table 1). During each experiment, temperature was recorded for 120 seconds: starting with 20 seconds of baseline temperature, 20 seconds of irrigation only, 60 seconds of continuous laser activation with irrigation, and last 20 seconds of irrigation only.
Laser Settings Used in This Study
Thermal dose (t43) for each trial was calculated using the Sapareto and Dewey formula 22 :
where t is time, T is temperature in °C, and R is a constant; 0.5 when T > 43 and 0.25 when T < 43. A t43 value >120 minutes is associated with a high probability for thermal tissue injury 22,23 so each trial was categorized based on whether t43 exceeded 120 minutes.
Parameter pairs (power and irrigation) were selected to span the thermal threshold. Five trials were performed at each parameter pair beginning with the lowest flow rate and laser power level (0 mL/min and 2.5 W). If all five trials did not exceed thermal threshold, the power was increased by the smallest increment (2.5 W for frequency <50 Hz and 5 W for frequency >50 Hz) while maintaining irrigation rate. This process was repeated until 5/5 trials for any parameter pair exceeded the thermal threshold. The next parameter pair selected was at the same power with irrigation increased by 5 mL/min. Parameter pairs were tested in this staircase manner until reaching the maximum laser power in this study (50 W). The number of trials exceeding t43 of 120 equivalent minutes is displayed at each data point on the parameter plots. Supplementary Figure S1 further depicts this methodology step by step.
Results
The number of trials at each parameter pair (power and irrigation) that exceeded the t43 thermal threshold of 120 equivalent minutes is shown in Figure 3 for the renal calix trials (Supplementary Figs. S2 and S3 for the renal pelvis and ureteral trials). When all five trials exceeded the thermal threshold, the circle is colored red. When 0 of the 5 trials exceeded the thermal threshold, the circle is green. When some of the trials exceeded the thermal threshold, the circle is yellow. For instance, all trials exceeded the thermal safety threshold when using 7.5 W or greater and no irrigation. Similarly, all trials using 30 W and irrigation of 15 mL/min or less also exceeded the thermal safety threshold. To determine the parameter (power and irrigation) safety boundary, the data points of highest power that were green at each irrigation rate were plotted. For each scenario (renal calix, renal pelvis, and ureter), this parameter safety boundary is linear within the tested range with parameter pairs below the line considered safe and those above the line unsafe. For example, using a 20 W laser setting will not result in thermally dangerous temperature in the ureter, calix, or pelvis when using irrigation at 15 mL/min, which corresponds to setting the bag at 100 cm with no pressure irrigation while using an access sheath. The safety boundaries for each scenario (Fig. 4) are essentially parallel with slope and y-intercept displayed in Table 2. The maximum tolerable laser power for renal calix < ureter < renal pelvis indicating that higher laser power at a fixed irrigation rate may be tolerable in the renal pelvis but could be thermally dangerous in the ureter or calix.
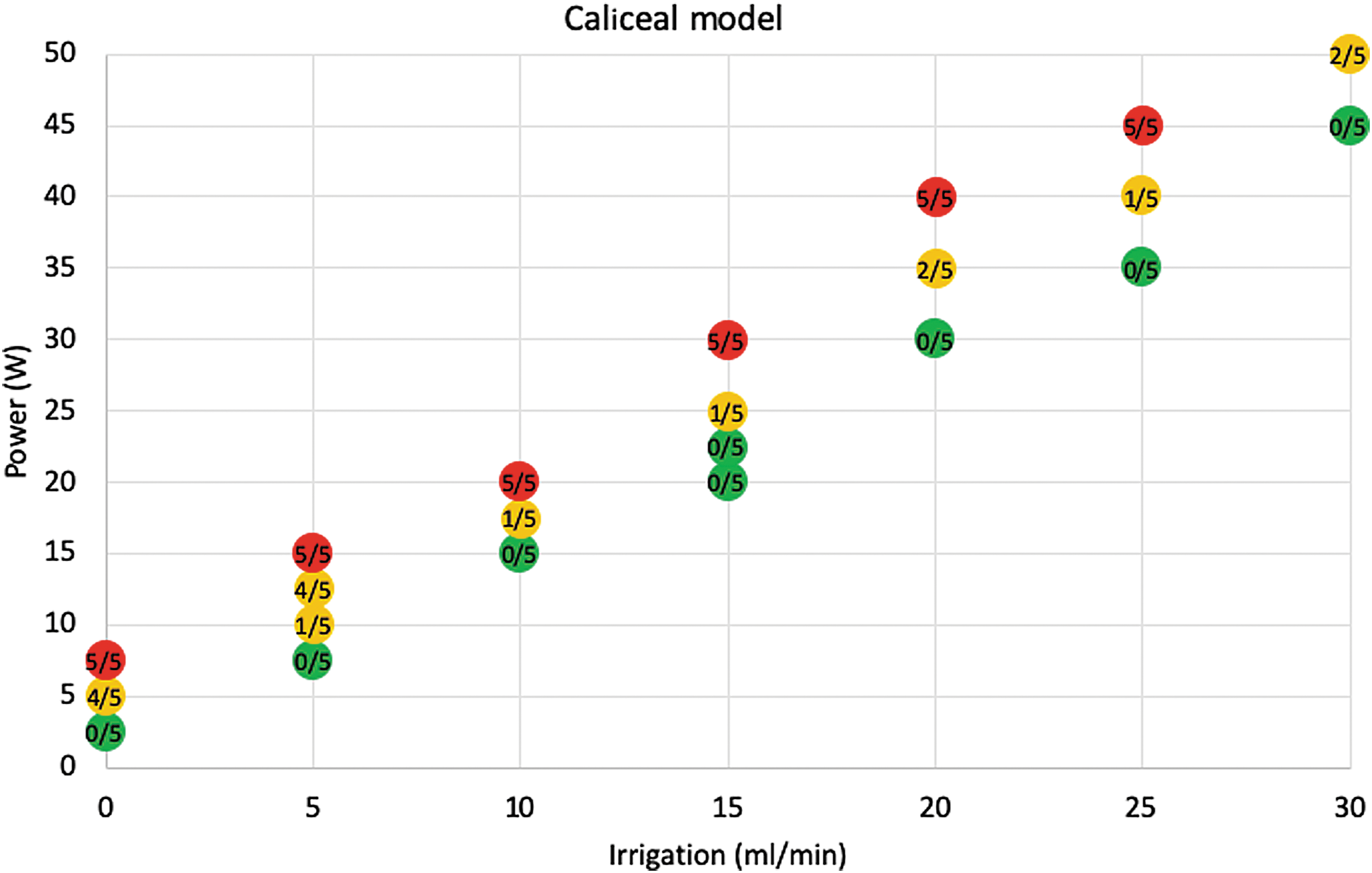
Results for the caliceal model from five laser trials at each selected parameter pair with the number of trials exceeding the thermal threshold for tissue injury (t43 = 120 minutes) indicated on each data point. Green circles represent no instances of excessive thermal dose, red circles represent 100% of trials exceeded thermal threshold, and yellow circles indicate that some trials exceeded the thermal threshold.
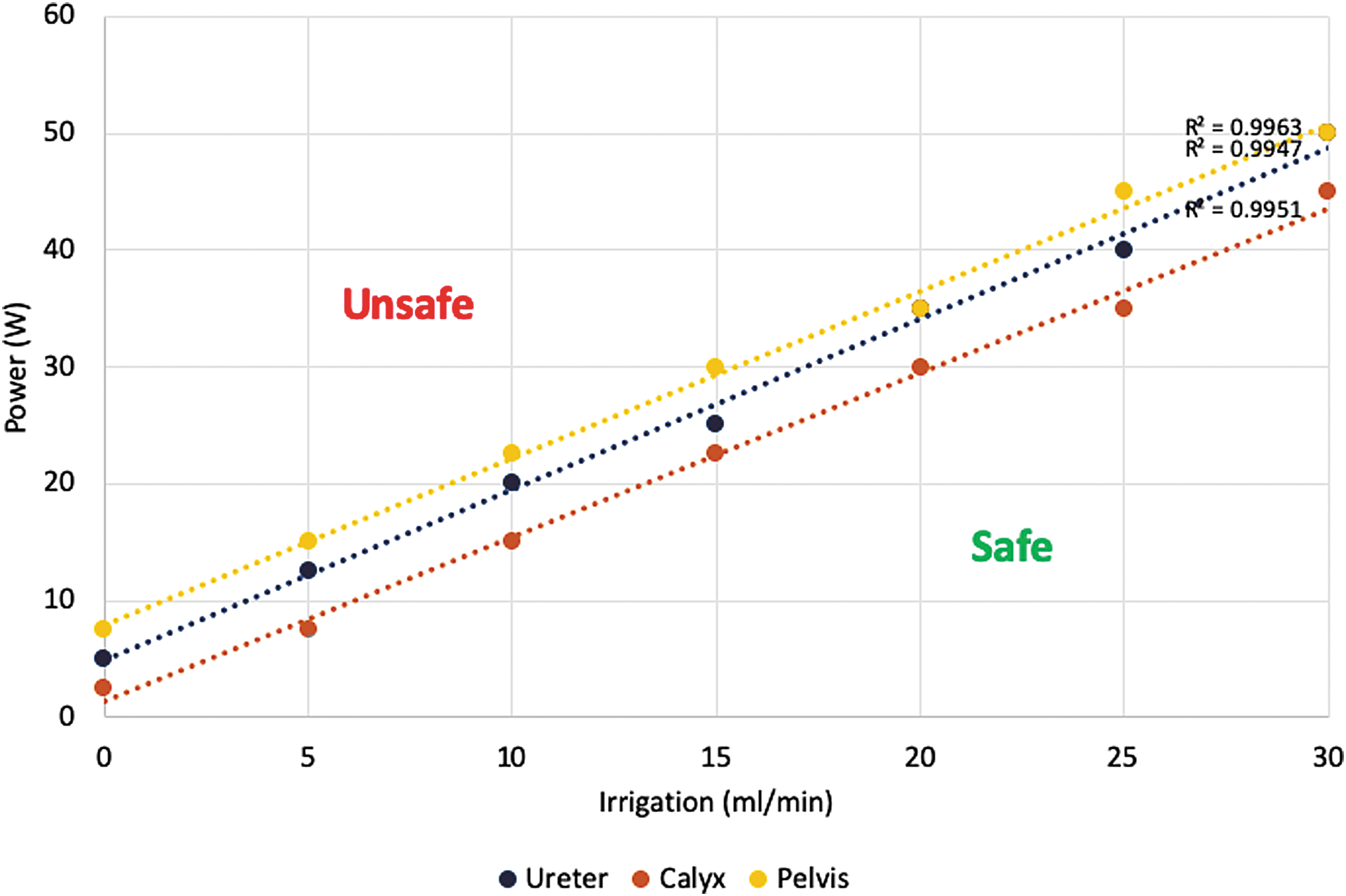
Parameter safety margins for renal calix, ureter, and renal pelvis models. Parameters below the lines are safe. Parameters above the lines may exceed the thermal threshold for tissue injury during ureteroscopy with laser lithotripsy.
Slope and Intercept Used to Fit the Safety Boundary Margins
The slope and intercept correspond to lines shown in Figure 4.
Discussion
With the advent of higher power laser systems for lithotripsy and dissemination of new techniques for stone comminution, greater attention must be paid to the rate of energy applied within the urinary system. The rate of energy delivered is defined as time-averaged laser power (W) and can be simply calculated as pulse energy (J) × pulse frequency (Hz). For example, both 0.5 J × 40 Hz and 1 J × 20 Hz laser settings deliver 20 W of power and will produce equivalent temperature elevation.
In addition to results from in vitro and porcine in vivo studies, 8 –12,14 –17 early clinical evidence is beginning to emerge of thermal tissue injury after high-power laser lithotripsy. In a recently published human study, Wang and colleagues 24 measured ureteral fluid temperature during ureteroscopic laser lithotripsy and found temperatures >56°C in 19 of 30 cases. Furthermore, the authors suggested that hydronephrosis and flank pain, which subsequently developed in three of these patients, might have been the result of thermal injury and ureteral obstruction. 24
Thermal tissue damage is dependent on the extent of temperature elevation and the time maintained at elevated temperature. Outcomes reported only as peak temperature achieved, or time to reach an arbitrarily chosen temperature value can be misleading and provide an incomplete measure of the risk of thermal injury. Sapareto and Dewey developed the concept of thermal dose to standardize the temperature–time relationship for tissues exposed to varying temperatures. 22 Tissue maintained at 43°C for 120 minutes receives the same thermal dose as tissue maintained at 50°C for 56 seconds or 56°C for 1 second. Any time/temperature curve can be transformed to a single measure of “equivalent minutes at 43°C” referred to as t43. This concept has been validated in numerous tissue types including kidney. 23 Most soft tissues are rendered nonviable with a t43 of 120 to 240 minutes. 25,26 There is some variability in this threshold for kidney tissue, with 70 minutes claimed to be the onset of thermal necrosis in a study by Yarmolenko and colleagues. 23 However, in determining the parameter safety boundary in this current study, a conservative tack was taken. The threshold for renal and ureteral tissue injury was selected to be t43 = 120 minutes. Parameter pairs were categorized as safe only if 0/5 trials exceeded the thermal threshold. The parameter safety boundary was calculated from the highest power setting that returned 0/5 trials exceeding thermal threshold.
The parameter safety boundaries determined in this study are linear across the clinically relevant parameter ranges tested and are essentially parallel for the three scenarios. This would imply that the irrigation rate needed to protect from thermal injury can be calculated based on the laser power applied and the volumes of fluid mixing (y-intercept) for each scenario (ureter, renal pelvis, and calix). If these relationships are validated in subsequent studies, it bodes well for creating a simple formula to determine the irrigation rate needed to mitigate thermal toxicity.
While it was expected that the more capacious renal pelvis would tolerate higher laser power more readily than the ureter or renal calix based on fluid volumes, it was surprising that the ureter fared better than the renal calix. Dye studies using each of these models (unpublished) suggest that although the ureter presents a smaller fluid volume in the vicinity of the laser than the renal calix, there may be a greater volume of fluid mixing than in the renal calix.
It must be noted that data collected in this study is based on in vitro measurement and may not completely account for all factors in vivo. However, results from previous in vitro and porcine in vivo laser lithotripsy thermal studies were closely correlated. 8,9 Another limitation of this study is that data are derived from 60 seconds of continuous laser activation. Typically, during clinical ureteroscopy cases, the laser is activated intermittently for shorter bursts of energy delivery. The duration of 60 seconds was chosen to match with the methodology of previous in vitro and porcine in vivo data in the literature. The concept of “operator duty cycle”—defined as the percentage of time the laser pedal is activated—is being studied as a way to account for varying patterns of laser use, thus providing a way to reconcile the fluid temperature elevation and thermal dose generated in clinical scenarios with the data and results in this study. Preliminary work from our group found that the operator duty cycle during the 1-minute of highest laser activity was 72%. This means that the laser was active for 43 seconds of the 60 seconds. Previously, we assessed the effect of 50% operatory duty cycle on heat generation in an in vitro study. 27 We found that even if the laser was activated intermittently, temperatures can still exceed thermal safety thresholds in certain scenarios.
An additional limitation of this study is that the laser was activated without targeting on a stone. In theory, some of the energy from a laser pulse is used to fragment stone, leaving less energy to heat the fluid. However, unpublished data from our laboratory from laser activation with and without targeting on a stone revealed no temperature difference. This may be because much of the energy absorbed by the stone may be reradiated as heat. Moreover, it has been demonstrated that for the vast majority of kidney stone materials, there is little measurable chemical decomposition during lithotripsy, and the laser only serves to break the stone into smaller pieces of the same material. 28 An alternative practical explanation is that a large portion of the energy from each pulse is absorbed into the fluid to create a vapor bubble; furthermore, during some forms of laser lithotripsy, such as high-power pop-dusting, only 17% of laser pulses strike stone, the remainder of the pulses miss with energy completely absorbed into the fluid. 29
While parameter plots with designated safety boundaries can be useful in selecting appropriate laser settings and irrigation rates, this requires assessment of irrigation rate, which can vary based on height of the irrigation bag above the patient, size of instruments within the working channel of the ureteroscope, pressure within the renal pelvis, and a variety of other factors. Some commercially available systems can deliver irrigation at a constant flow rate, but these are not yet widely utilized. As pressure and temperature are the two most relevant parameters to ensure safe ureteroscopy and laser lithotripsy, future evolution of technology should include sensors to directly measure these parameters to provide real-time feedback.
Conclusions
This study describes the methodology to determine parameter safety boundaries that can be used to guide proper selection of thermally safe laser settings and irrigation rates during ureteroscopy with laser lithotripsy. Using established thresholds for thermal tissue injury, laser lithotripsy settings ranging from 2.5 to 50 W and irrigation rates ranging from 0 to 30 mL/min were tested in vitro and used to define a parameter safety boundary for renal calix, renal pelvis, and ureteral scenarios. These parameter plots can be used to formulate guidance to select laser lithotripsy and irrigation settings that are thermally safe. Alternatively, these plots allow determination of the irrigation rate needed to safely control the thermal dose from specific laser settings. This methodology will also provide a framework to assess the effectiveness of various strategies to control and mitigate thermal dose.
Footnotes
Author Disclosure Statement
K.R.G. is a consultant for Lumenis and Boston Scientific. W.W.R. is a consultant for Boston Scientific.
Funding Information
This study was supported by a scientific research grant from Boston Scientific.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.