
Abstract
Objective:
To demonstrate the safety and efficacy of flexible ureteroscopy lithotripsy (FURL) and miniaturized percutaneous nephrolithotomy (MPCNL) through the comparative studies in treating medium-sized lower-pole renal calculi.
Methods:
Two hundred and twenty eligible patients with lower-pole renal calculi (1–2 cm) were enrolled and further randomly assigned into FURL group and MPCNL group. Patients' demographics, preoperative characteristics, intraoperative and postoperative complications, stone-free rate, and comfort and pain indicated by Bruggrmann Comfort Scale (BCS) and visual analog scale (VAS) were evaluated and recorded. Trauma index such as white blood cells, C-reactive protein (CRP), and interleukin (IL)-6 were also detected.
Results:
The stone-free rate and the operating time were comparable in FURL and MPCNL groups. Intraoperative and postoperative complication analysis showed that blood loss and hospital stay were significantly lower in the FURL group compared with MPCNL group. No significant difference in minor pelvic perforation, false passage, hemoglobin drop, persistent hematuria, ureteral perforation, moderate fever, urosepsis, and postoperative serum creatinine level was observed. However, as to comfort and pain indicated by BCS and VAS and stress indicated by CRP and IL-6, FURL was superior to MPCNL.
Conclusion:
FURL could be a better alternative surgical method to MPCNL with similar curative effect and less blood loss and hospital stay.
Introduction
In general, nephrolithotomy options are based on the size and location of calculi. Lower-pole calculi are more challenging to treat compared with calculi in other areas of the kidney for the gravity-dependent positioning and anatomic features. What makes it more complicated is that cost, patient preference, patient body habitus, and local renal anatomy must be considered to determine the optimal treatment modality for medium-sized lower-pole renal calculi. 1,2
Extracorporeal shockwave lithotripsy (SWL) is the guideline recommended for the therapy of small and medium-sized (1 to 2 cm) renal calculi, with efficacy highly dependent on calculi size and location, accounting for the disappointing treatment results for lower-pole calculi. 3 –5 To get higher stone-free status, variable rate of second-look nephroscopy is needed in percutaneous nephrolithotomy in different transplant centers, which will lead to a prolonged inpatient hospital stay. 6,7 Compared with percutaneous nephrolithotomy, minimal morbidity and suboptimal stone-free rates are associated with SWL.
With miniaturized nephroscope and size reduced percutaneous tract nature, miniaturized percutaneous nephrolithotomy (MPCNL) is designed with the goal of lowering complication rates and maintaining high stone-free rate of percutaneous nephrolithotomy. However, in addition to the minimally-invasive nature, whether MPCNL has some inherent superiority over conventional percutaneous nephrolithotomy in safety and efficacy is still in dispute. 8 –10
Retrograde flexible ureteroscopy is widely utilized in the treatment of upper urinary tract calculi with the advantages of less invasiveness, less hemorrhage, and less hospital stay. In consideration of the improving retrograde instrumentation and suboptimal treatment effects of SWL and MPCNL, flexible ureteroscopy lithotripsy (FURL) may serve as a compromise between the percutaneous approach and extracorporeal procedure. Compared with SWL, FURL has substantially minimal morbidity, higher stone-free rate, and good safety profile, 6,11 –13 which is widely utilized in the management of medium-sized calculi.
In this research, the safety and efficacy of FURL and MPCNL are deciphered through the comparative studies in treating medium-sized lower-pole renal calculi.
Materials and Methods
Patients
A prospective, simple random sampling and unblinded controlled study were performed from May 2017 to July 2019 at Peking University Shougang Hospital. Patients found to have single lower-pole renal calculi (1–2 cm) on abdominal computed tomography were included in this research. Exclusion criteria were severe hydronephrosis, severe urinary infection or tuberculosis, coagulation disorders, renal anatomic anomalies, and serum creatinine level >177 μmol/L. Simple random sampling was adopted, and parallel randomization was conducted at a ratio of 1:1, stratified by site, and was carried out using computer software STATA® version 13.0 (StataCorp LP, College Station, TX) to generate random numbers. The whole study was approved by the Institutional Ethics Committee of Peking University Shougang Hospital, and informed consents were obtained from the patients enrolled. The Clavien–Dindo grading system, including operating time, hospital stay, hemoglobin drop, and postoperative pain, was utilized to evaluate postoperative condition. 14,15 Calculi density was indicated by Hounsfield units measured with computed tomography scan. Antibiotic (ciprofloxacin, 0.2 g) was infused intravenously 1 hour before operation, and balanced fluid was continuously infused during operation. Tolazamide (20 mg) and flumethiazide (5 mg) were given at the beginning of operation to reduce fluid absorption during operation and to prevent infection. The relevant medical records were retrospectively reviewed. Detailed clinic data and demographic characteristics are listed in Table 1.
Patient's Demographics and Preoperative Clinical Characteristics Between the Two Study Groups
Data are presented as mean ± SD or n (%).
BMI = body mass index; FURL = flexible ureteroscopy lithotripsy; IPA = infundibulopelvic angle; MPCNL = miniaturized percutaneous nephrolithotomy; PNL = percutaneous nephrolithotomy; URS = ureteroscopy.
Flexible ureteroscopy lithotripsy
Ureteroscopy was performed with a Wolf semirigid Olympus ureteroscope (8/9.8F) in the affected side, which was placed along with the super-smooth guidewire in the lithotomy position. Next, a flexible ureteroscope (12/14F; Olympus, Japan) with a 200-μm laser fiber was advanced. The calculi were fragmented with a Holmium:Yttrium-Aluminum-Garnet (Ho:YAG) laser (1/1.2 J, 10 Hz). A Nitinol stone basket was utilized to remove large calculi fragments after preparing accessed sheaths, while small calculi fragments (<2 mm) were left in situ for spontaneous passage.
Miniaturized percutaneous nephrolithotomy
Under general anesthesia, an open-end ureteral catheter (5F) was inserted into the renal pelvis in the lithotomy position under cystoscopy vision. A puncture needle and guidewire were utilized to perform percutaneous access with the guidance of Doppler ultrasonography in the prone position. Subsequently, serial fascial dilators (6–16F) were used to dilate the percutaneous tract, and a peel-away sheath (16F) was maintained in the percutaneous access. After that, a rigid ureteroscope was inserted into the guidewire. Lithotripsy was performed with a Ho:YAG laser (1/1.2 J, 10 Hz). After the surgery, a Double-J ureteral stent (5F) was left in the presence of pyelocaliceal blood clots, which were removed 2 weeks later. Pelvic perforation drainage was performed with a silicone nephrostomy tube placed in the MPCNL channel.
Postoperative evaluation and follow-up
The differences in blood loss, hospital stay, hemoglobin drop, operation time, creatinine level, and complication incidence were compared. The stone-free rate was defined as no residual fragments (≥0.3 cm) on the ultrasonography or radiograph at 1 day and on computed tomography at 3 months post the operation. 16 The severity of pain was assessed at 6, 24, and 48 hours postoperation with a visual analog scale (VAS; range: 1–10) and Bruggrmann Comfort Scale (BCS) score (ranging between 0 “persistent pain” and 4 “cough is painless”). 15,17 The hospital stay was recorded from the time of surgery to the day of discharge. Blood loss was evaluated as previous reported equation (Blood loss [mL] = Hemoglobin drop during surgery [g/L] × flushing solution [mL]/Hemoglobin before surgery [g/L]). 18
White blood cell, C-reactive protein, and interleukin-6 measurement
The blood samples were drawn from venous lines at 6 AM at surgery day and postsurgery, and white blood cell (WBC) was measured through cell counter. C-reactive protein (CRP) was assayed immunoturbidimetrically in routine clinical chemistry analyzer (Roche, Hitachi). The level of serum interleukin (IL)-6 was detected with ELISA Kits (eBioscience, San Diego, CA) according to the manufacturer's instructions. All standards and samples were assayed with a microplate SpectraMax M5 reader (Molecular Devices, Thermo Fisher) at a wavelength of 450 nm.
Statistical analysis
Categoric data were analyzed using the Chi-square test. Continuous variable was assessed with t-test or post hoc test for the two-way analysis of variance analysis. The value p < 0.05 was statistically significant.
Results
The flow diagram for trial recruitment was indicated in Figure 1. Of the 264 consecutively enrolled patients, 220 patients were randomized into FURL group and MPCNL group. Four patients assigned in the MPCNL group had purulent fluid in the initial puncture, and the following MPCNL procedure was aborted. Patients' demographics and preoperative clinical characteristics, such as gender, age, surgery history, routine laboratory test, physical examinations, imaging examinations such as plain radiography of kidneys–ureters–bladder and computed tomography scan, and calculi character, are summarized in Table 1.
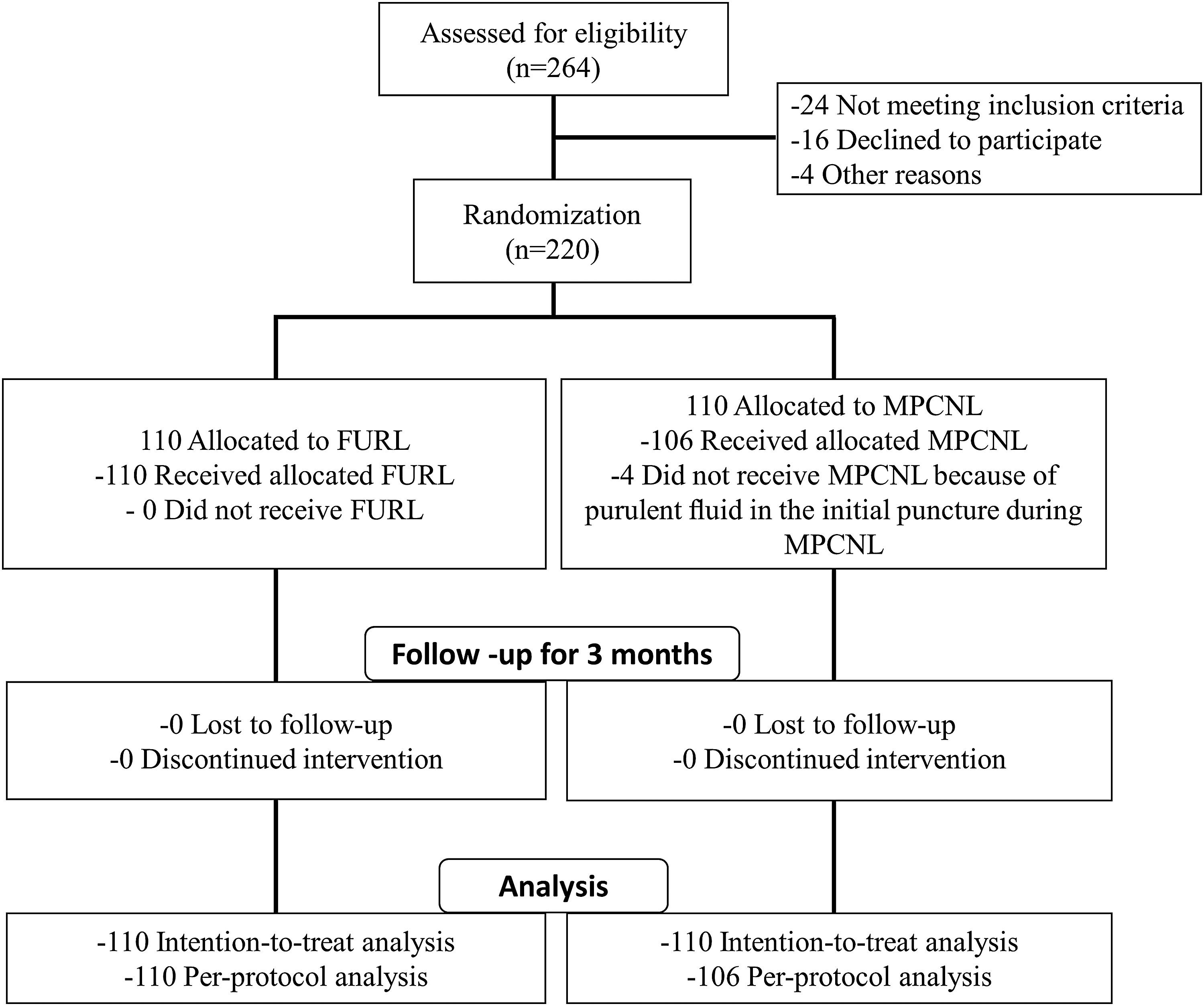
Flow diagram showing study recruitment. FURL = flexible ureteroscopy lithotripsy; MPCNL = miniaturized percutaneous nephrolithotomy.
First of all, the clinical safety between FURL and MPCNL treatment was evaluated. The patients were well tolerant with the operation, and minor and short-term complications were observed. No significant difference in operating time (Table 2, 87.2 ± 13.34 vs 79.6 ± 14.86 min, p = 0.124) was observed. Two patients in the MPCNL group had minor renal pelvic perforation with prolonged Double-J stenting for 2 weeks (Clavien–Dindo Grade II), and one patient in the MPCNL group developed urosepsis postoperatively. All patients improved after antibiotic treatment. One patient in the MPCNL group and three patients in the FURL group had an iatrogenic false passage with prolonged Double-J stenting for 4 weeks (Clavien–Dindo Grade II) (Table 2). There was no significant difference in intraoperative complications (minor pelvic perforation, false passage, and hemoglobin drop) and postoperative complications (persistent hematuria, ureteral perforation, moderate fever, and urosepsis) between FURL and MPCNL treatment (Table 2). The comparable creatinine level in MPCNL (88.9 ± 30.6) and FURL (91.6 ± 25.7) indicated that both procedures are well tolerated with the patients from a renal function viewpoint. It was worth noting that significantly reduced blood loss (p = 0.002) and hospital stay (p = 0.007) were observed at the FURL group compared with the MPCNL group.
Comparison of Intraoperative and Postoperative Variables Between the Flexible Ureteroscopy Lithotripsy and Miniaturized Percutaneous Nephrolithotomy Groups
Data are presented as mean ± SD or n (%).
Moderate fever, 100.5–102°F. The bold fonts indicate the statistical significance (p < 0.05).
As shown in Table 3, there was no significant difference in the first week, first month, and 3 months postoperative renal stone-free rate. The 3 months stone-free rate in both FURL and MPCNL treatment were more than 97%. FURL treatment could improve 6, 12, 24, and 48 hours BCS scores (p < 0.01) compared with MPCNL group. The mean pain indicated by VAS at 6, 12, 24, and 48 hours was significantly lower in the FURL group compared with the MPCNL group (p < 0.001 or p < 0.01), which suggested that FURL had treatment benefit over MPCNL on pain relief.
Comparison of Stone-Free Rate, BCS Score, and Pain Visual Analog Scale Score Between the Flexible Ureteroscopy Lithotripsy and Miniaturized Percutaneous Nephrolithotomy Groups
Data are presented as mean ± SD or n (%).
The bold fonts indicate the statistical significance (p < 0.05).
BCS = Bruggrmann Comfort Scale; VAS = visual analog scale.
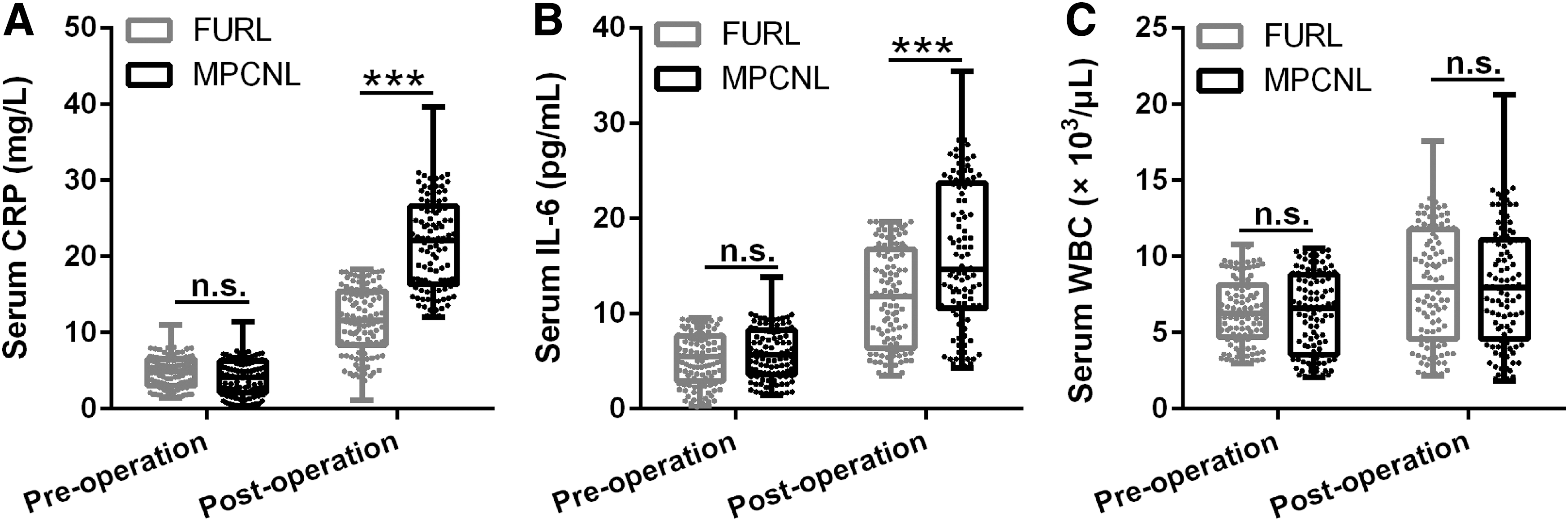
As to the trauma index (WBC count, CRP, and IL-6) detected, there was no significant change in WBC count (Table 4 and Fig. 2C), while significant change in serum CRP and IL-6 levels was observed (Table 4 and Fig. 2A, B, p < 0.001) in FURL group compared with MPCNL group.
Comparison of CRP
Comparison of C-Reactive Protein, White Blood Cell, and Interleukin-6 Preoperation and Postoperation Between the Flexible Ureteroscopy Lithotripsy and Miniaturized Percutaneous Nephrolithotomy Groups
Data are presented as mean ± SD. Bold fonts indicate significant difference.
CRP = C-reactive protein; IL = interleukin; n.s. = no significant difference between the indicated groups; WBC = white blood cell.
Discussion
Lower-pole renal calculi can be symptomatic, infection related, locally obstructing, size increasing, and intervention required disorders. The treatment options of medium-size calculi are controversial regarding respective roles of SWL, PCNL, and ureteroscopy. It is worth noting that intrarenal anatomy and stone fragility should also be considered to give appropriate therapeutic intervention. 19,20 Although MPCNL is introduced in this study to decrease the risk of conventional PCNL, MPCNL is not superior to FURL in operative times, hospital stay, and blood loss, which may be attributed to the temporary placement of ureteral stents or tubes. Moreover, MPCNL has comparable stone-free rates with FURL, which can be considered as the critical parameter to evaluate the efficacy of nephrolithotomy. The patients who underwent the FURL treatment will have relative comfort perception compared with MPCNL group as indicated by BCS and VAS. This study indicates that medium-sized lower-pole calculi are best managed with FURL, at least comparable to MPCNL. However, the consistence of such observation needs to be confirmed in multicenter research.
Advanced techniques are utilized in FURL, such as flexible scopes and highly effective Ho:YAG laser, 21,22 which can help to access the lower-pole (difficult stone localizations) and fragment calculi with different textures indicated by Hounsfield units on computed tomography scan. FURL is retrograded into the natural canal of the human body along with ureter, renal pelvis, and calix, and Nitinol stone basket is utilized to basket out large calculi fragments (>2 mm), all of which will also add the risk of ureter damage. 23,24 MPCNL requires more aggressive procedures, such as guidewire placement, puncture needle and drainage nephrostomy tube removal, and single-step or serial tract dilation, which might increase the risk of the blood loss and prolonged hospital stay observed in this research. Hemorrhage and relevant complication are worrisome after MPCNL treatment, while in this research only one patient shows urosepsis, which indicates the feasibility of such procedure. It is worth noting that although in dispute, the negative determining factors related with renal anatomy for calculi clearance, 25 –27 such as infundibulopelvic angle <45°, infundibular length >3 cm, and infundibular width <5 cm, are not deciphered in this study, which may need further detailed investigation.
The stress response can also be detected in minimally invasive surgery due to the trauma and the related pain and inflammation effects, which may contribute to the upregulated inflammatory factors, such as CRP and IL-6. IL-6 can function as the vital factor to promote liver cells to secrete CRP and cell phagocytosis to facilitate tissue repair. 28 –30 As a sensitive stress associated marker, CRP level is raised in most infection, inflammation, or tissue damage conditions. FURL treatment causes less upregulation of CRP and IL-6 compared with MPCNL group, which suggests that FURL can induce decreased systematic stress compared with MPCNL.
It is estimated that 50% of first-time stone formers will recur within 10 years, highlighting the significance of long-term follow-up study. In such a situation, further randomized, controlled multicenter trials with the long-term follow-up would be needed to verify this observation in the future. Our study suggests the potential advantages of FURL compared with MPCNL due to less bleeding, hospital stay, and pain, which will give another treatment option.
Conclusion
FURL has comparative efficacy but improved safety profile and patient tolerability on the treatment of medium-sized lower-pole calculi compared with MPCNL.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.