
Abstract
Introduction:
Although laparoscopic urachal excision in children has been well reported, there are limited data on a robot-assisted surgery (RAS) approach. The hidden incision endoscopic surgery (HIdES) technique is an established method of eliminating visible scars following a number of RAS urologic procedures. We report our experience of using a robotic approach to treat urachal anomalies in children, and we present the first description of utilizing the HIdES port configuration for this procedure.
Materials and Methods:
We retrospectively reviewed pediatric patients who underwent resection of a urachal remnant at our institution from 2013 to 2018. Surgical techniques were either the traditional open approach (OA) or RAS. HIdES trocar placement configuration was employed in all robotic cases. Patient demographics, perioperative data, pathology reports, and outcomes were abstracted and compared.
Results:
Twenty-three patients underwent a urachal remnant resection in the study period (RAS: 14 patients vs OA: 9 patients). RAS patients were older (8.5 vs 2.0 years, p = 0.031) and weighed more than OA patients (36.1 vs 13.9 kg, p = 0.063). Median operative time for RAS was longer than OA operative time (136 vs 33 minutes, p < 0.01). Fewer RAS patients were outpatient compared with OA (7.1% vs 66.7%, p < 0.01), but with a median length of stay of 1 day (0–1 day). Two patients (14.3%) in the RAS group experienced postoperative complications within 1 week of the procedure compared with 1 (11.1%) in the OA group. There was no significant difference in blood loss, postoperative narcotic requirements, or duration of follow-up between both groups.
Conclusion:
RAS is a safe and feasible alternative to open surgery for urachal anomalies. Complete excision can be achieved by using HIdES port configuration, allowing for excellent cosmetic outcomes that are superior to traditional surgical scars without limitation to essential surgical ergonomics.
Introduction
Urachal anomalies occur when the urachus fails to obliterate during normal embryologic development. Abnormal remnants may give rise to a spectrum of pathology, including urachal cysts, sinuses, and diverticula. Symptomatic cases may present as umbilical drainage, abdominal pain, and recurrent urinary tract infections (UTIs), but incidentally discovered asymptomatic remnants are not uncommon. Although malignant transformation has not been reported in children, it has been described in adults. 1 Consequently, some advocate surgical excision to completely eliminate the risk of future malignant degeneration. 2
Open surgery has, historically, been the standard of care, allowing complete excision of the urachal remnant, and bladder dome if necessary. Recently, laparoscopic and robot-assisted surgery (RAS) excision of the urachus has been reported as a safe and effective alternative to open surgery with the added benefit of improved cosmesis. However, historical and present series mainly comprise adults, with only a few studies including children. 3 –7
In this study, we report our experience employing RAS excision of urachal remnants in a pediatric cohort. To improve cosmesis, we employed the hidden incision endoscopic surgery (HIdES)℠ technique (Fig. 1). 8 The HIdES technique was developed by Gargollo in 2011 as an approach to improve cosmetic outcomes after RAS by eliminating visible scarring. Other studies have assessed the versatility of HIdES and support its use for a number of RAS procedures in pediatric urology. 8 –11 We hypothesize that HIdES offers a feasible alternative for a minimally invasive approach with the added advantage of hidden incisions compared with traditional open surgery in the management of urachal remnants. Herein, we describe the HIdES technique in the management of pediatric urachal anomalies and compare our outcomes to similar patients treated with open surgery.
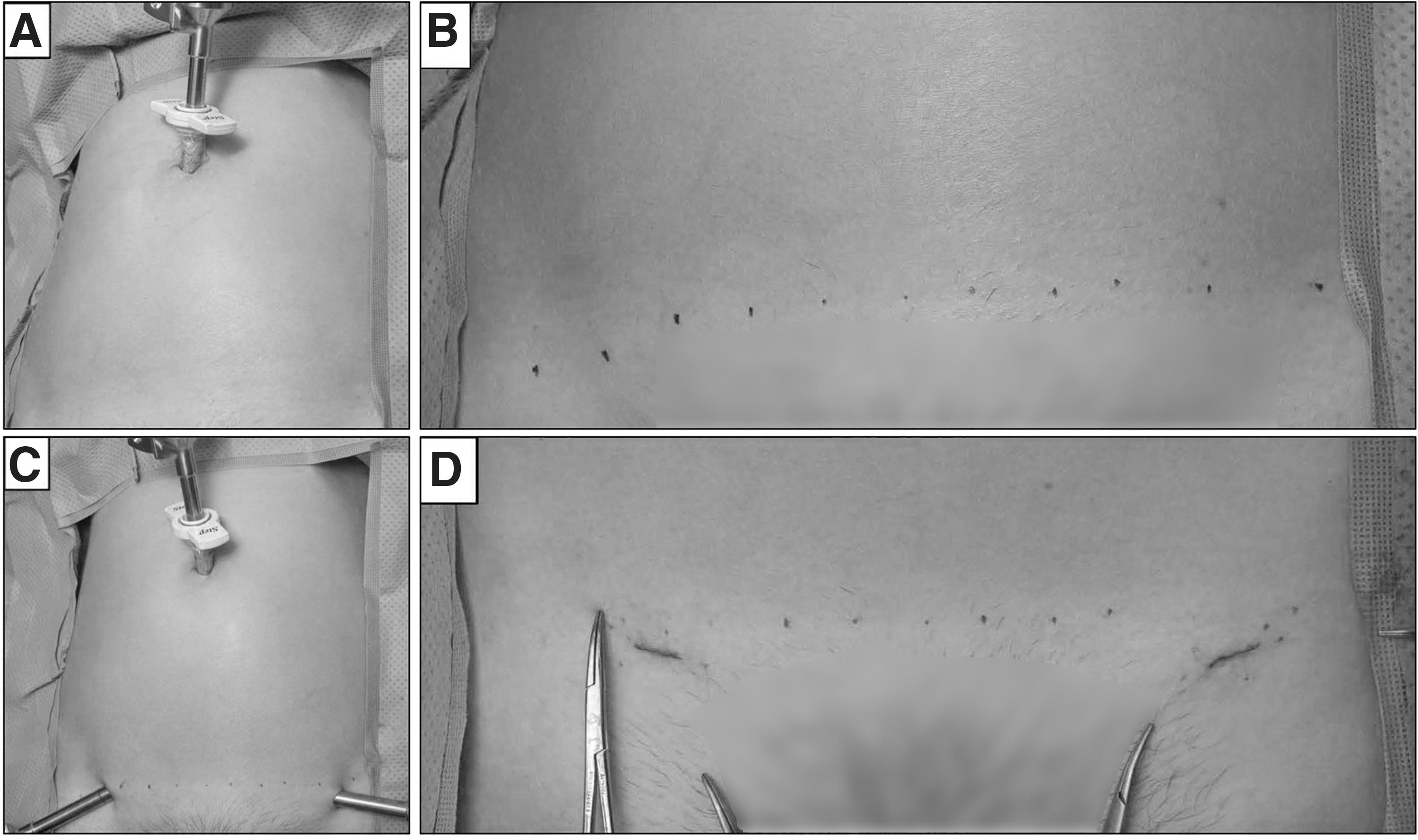
Hidden incision endoscopic surgery port placement for
Patients and Methods
Patient population and data collection
After obtaining Institutional Review Board approval (IRB no. 17-006368), we retrospectively reviewed the medical records of patients aged ≤18 years in whom urachal remnants were diagnosed at our institution from 2013 to 2018. Demographic data, clinical characteristics, surgical approach, perioperative outcomes, and length of stay (LOS) were reviewed and recorded. Follow-up data, including consequent visits to the emergency department (ED) within 1 week of the procedure or hospital readmissions due to postoperative sequelae, were also examined. The severity of complications was stratified according to the Clavien–Dindo (CD) classification system. 12
All patients had radiographic evidence (CT, voiding cystourethrogram, and/or ultrasonography) of urachal remnants before surgery. Indication for surgical excision included: symptomatic remnants and increase in size on serial imaging for asymptomatic or incidentally discovered remnants. All RAS cases and one open approach (OA) case were performed by pediatric urologists. The remaining eight OA cases were performed by pediatric general surgeons. Where OA was employed, access to the remnant was via an infraumbilical, or lower midline incision. For patients who underwent RAS, ports were placed by using HIdES configuration as initially described. 8
Surgical technique: HIdES
Cystoscopy was initially performed to survey the bladder for known or suspected communication between the bladder and the remnant. Operative times were measured as the time from the skin incisions for port placement to closure of incisions; the duration of the cystoscopy was not included. A Foley catheter was typically placed after cystoscopy to decompress the bladder and left indwelling for the duration of the case.
The urachal excision was performed by using a transperitoneal approach. Pneumoperitoneum was established by using a Veress needle (Covidien, Norwalk, CT) inserted at the umbilicus; insufflation pressures were age dependent. Laparoscopic ports were placed by using the HIdES technique as follows: An 8.5-mm trocar was inserted through an incision in the umbilicus for the camera port. Additional working ports were placed by using trocars inserted medial to the anterior superior iliac spine bilaterally below the line of Pfannenstiel incision (Fig. 1). Before docking the robot, the urachal stalk was transected from the umbilicus in a conventional laparoscopic fashion with scissors or electrocautery. Both the da Vinci Si® and Xi® surgical systems (Intuitive Surgical, Inc., Sunnyvale, CA) were utilized.
After the robot was docked, peritoneal attachments to the bladder dome were dissected. The region where the remnant attached to the bladder apex was circumferentially isolated and excised with electrocautery. A small cuff of bladder mucosa was removed en bloc with the remnant if a communication between the remnant and the bladder was suspected or identified pre-operatively. The excised specimen was placed into an EndoCatch™ specimen retrieval pouch (Covidien Plc., Mansfield, MA) and sent to pathology for cryosection and histological assessment. The cystotomy (or partial cystectomy) was repaired in two layers with V-Loc™ (Covidien Plc.), 3-0 Vicryl® (Ethicon, Inc., West Somerville, NJ), or 3-0 Quill™ (Angiotech Pharmaceuticals, Vancouver, Canada) sutures. After the closure, the bladder was irrigated with normal saline, or methylene blue, to assess for leakage. Foley catheters were left indwelling, or they were removed at the end of the procedure depending on the extent of the partial cystectomy.
Postoperative analgesia
Where RAS was employed, patients received intraperitoneal aerosolized 0.25% Bupivacaine sprayed onto the diaphragm by using a Mucosal Atomization Device (MADett®) endotracheal aerosolizer (Wolfe Tory Medical, Inc., Salt Lake City, UT) after undocking the robot. Alternatively, patients received local 0.25% Bupivacaine injected into incision sites before closure at the end of the procedure.
For both RAS and OA, patients were administered a combined regimen of Acetaminophen and Ketorolac (or Ibuprofen) for pain control postoperatively. Narcotics were administered on a case-by-case basis as needed. Administered dosages of narcotics were converted to their postoperative milligram morphine equivalents and recorded.
Statistical analysis
Analyses were performed by using JMP® Pro 14.0 (SAS, Inc., Cary, NC). Differences between categorical and continuous variables were evaluated for significance by using the chi-squared test (or Fisher's exact test where necessary) and Wilcoxon rank-sum test, respectively. A p-value <0.05 was considered significant.
Results
Patient characteristics
We identified 24 children who were surgically treated for urachal remnants during the study period. Fourteen (58.3%) received RAS and 9 (37.5%) were treated with OA; 1 (7.1%) patient was treated by using traditional laparoscopy and was excluded from the study. Cohort demographics and clinical characteristics are summarized in Table 1. Patients who underwent RAS were significantly older (median age [range]: 8.5 [2–16] vs 2 [1 week–16] years, p = 0.031), and they were markedly heavier than children treated with OA (median weight at surgery [range]: 36.1 [11.4–152] vs 13.9 [3.8–66.3] kg, p = 0.063).
Patient Demographics and Presenting Symptoms
Majority of the symptomatic patients presented with >1 chief complaint.
HIdES = hidden incision endoscopic surgery; OA = open approach; UTI = urinary tract infection.
The majority of patients (RAS: 10/14, 71.4%; OA: 5/9, 55.6%) were symptomatic at presentation, with most patients presenting with multiple symptoms. Abdominal pain (6, 42.9%) and fever (5, 35.7%) were the most common symptoms in the RAS group, whereas umbilical drainage (44.4%) was more prominent in the OA cohort. Approximately a third of both groups were incidental (28.6% vs 33.3%).
Operative outcomes, pathology, and follow-up data
Median operative time was longer in the RAS cohort (133 vs 33 minutes, p < 0.01). Four (28.6%) patients in the RAS group and 3 (33.3%) in the OA group underwent concurrent procedures at the time of surgery (Table 2). Notably, concurrent procedures did not affect the marked difference in procedure length between both groups. Urachal cysts were the most prevalent diagnoses in our cohort (9/24, 37.5%). Four patients (28.6%) in the RAS group had urachal cysts that were infected with Escherichia coli at presentation. These patients were initially managed with percutaneous drainage and culture-specific antibiotic therapy before surgery. All excised specimens were benign on pathologic assessment. There were no conversions to open surgery in the RAS cohort, and no difference in the median blood loss between groups (5 mL [range: 0–20 mL] vs 5 mL [range: 0–5 mL], p = 0.06) (Table 3).
Perioperative Characteristics, Pathology, and Complications of Hidden Incision Endoscopic Surgery and Open Approach Patients
CD = Clavien–Dindo; LOS = length of stay; MME = milligram morphine equivalents; NOS = not otherwise specified.
Summative Postoperative Characteristics and Outcomes of Patients
Postoperatively, a Foley catheter was left indwelling in 12 (85.7%) patients postoperatively for a median of 2 days (range: 0–4 days) in the RAS cohort, whereas 4 (44.4%) patients in the OA group had indwelling catheters for a median of 1.5 days (range: 0–9 days). A median dosage of 9.15 mg (range: 7.5–37.6 mg) morphine equivalent was administered orally to 4 patients (28.6%) in the RAS group and 1 (11.1%) in the OA group. Median LOS was 1 day (range: 0–1 day) for all patients; only 1 patient (7.1%) was discharged on the same day as the procedure in the RAS cohort, whereas 6 patients (66.7%) in the OA cohort were sent home on the same day.
Two (14.3%) patients in the RAS cohort and 1 (11.1%) in the OA cohort had complications requiring a visit to the ED within 1 week of the procedure. In the RAS group, patient no. 1 presented to our ED on postoperative day (POD) 2 with generalized abdominal pain. Further work-up revealed a UTI (CD grade II) as the likely etiology; the patient was treated empirically with antibiotics. Notably, this patient had a history of urinary retention. Similarly, patient no. 2 presented to our ED with uncomplicated abdominal pain on POD 3. Pain control was re-established with over-the-counter analgesics (CD grade I). Of note, this patient had a history of chronic pain syndrome. In the OA group, one patient presented to our ED on POD 4 with peri-incisional superficial cellulitis. This was treated with antibiotics (CD grade II). No patient from either cohort was admitted to the hospital as a result of their symptoms.
Overall, median duration of follow-up was ∼1 week in both groups (6.5 days [range: 0–4 months] vs 8 days [range: 0–1 month], p = 0.41).
Discussion
Advances in minimally invasive surgery (MIS) techniques have ushered changing paradigms in the management of pediatric urologic conditions. In line with this trend, robotic surgery has continued to gain popularity as an attractive alternative to open surgery by offering select benefits, including improved cosmesis and less postoperative pain. Although the benefits of traditional laparoscopic and robot-assisted laparoscopic techniques in urologic procedures have been well defined in adults, there is a paucity of reports evaluating similar outcomes in children. In the present series, we demonstrate complete excision of urachal anomalies and successful bladder repair using RAS in a pediatric series. To our knowledge, our article is the first to describe the HIdES technique for robot-assisted excision of urachal remnants in children.
Urachal anomalies result from a failed or incomplete obliteration of the urachal lumen during the 4th to 5th months of gestation. Symptoms from these remnants, by virtue of the differences in lesions, are varied and may overlap. In line with existing literature, periumbilical drainage, abdominal pain, and fever were the most common symptoms in our series (Table 1). 13 Similarly, additional findings, such as hematuria and UTIs, were infrequent in our series, similar to previous reports. 2,14 On the other hand, remnants may be discovered incidentally as seen in 29% of our entire cohort (Table 1). Naiditch and associates advocated for removal of only symptomatic remnants, as asymptomatic remnants may be safely observed for spontaneous resolution without exposing patients to undue risk without well-defined long-term benefits. 1,14,15 Whether these lesions will eventually become problematic or undergo malignant degeneration lacks consensus, making the decision for surgical removal controversial. 1
Urachal cysts were the most prevalent diagnoses in our series (Table 2); this distribution is in line with the current opinion. 2,14,15 Although urachal malignancies in children have never been reported, initially benign remnants in children are believed to be associated with an increased risk of bladder adenocarcinomas in adults. 16 The strength of this association, if any exists, remains unclear, resulting in opposing views on the best management approach. 1,2 We found no evidence of malignancy in any of the excised specimens in our series.
A small number of publications have described robotic excision of urachal lesions in children. Rivera et al. reported their outcomes from RAS urachal excision in an 11-patient series, wherein 3 were children. 6 Notably, 2 out of 3 pediatric patients in their series required an average of 11.25 mg morphine equivalents of postoperative narcotics. This is lower than the mean dosage of roughly 16 mg required by 4 out of 14 patients in our RAS cohort, and 1 out of 9 in our OA cohort who required 22.5 mg. The age difference between the groups on pain management requirements cannot be overlooked. Indeed, only patients older than 8 years received narcotics in both groups; hence, it is expected that the markedly younger OA cohort received fewer narcotics for pain control postoperatively.
Ahmed et al. recently reported promising outcomes utilizing RAS in 16 pediatric patients with varied urachal lesions. 17 The authors reported a median operative time of 107 minutes, which is shorter than our median of 133 minutes. We attribute this finding to prolonged adhesiolysis stemming from reactive inflammation caused by the infected cysts. The significant difference in operative duration was not surprising. We anticipate the difference in operative time to significantly narrow with increasing experience. 18 In addition, Ahmed et al. reported a median LOS of 1.5 days; this decreased to 1 day if a bladder cuff was not taken, and it increased to 2 days if a bladder cuff was excised. The median LOS in our cohort was 1 day; this remained unchanged among patients regardless of whether or not a bladder cuff was removed with the remnant.
However, although the majority of the OA patients were outpatient, only one RAS patient was discharged on the same day as the procedure. Although decreased LOS has been a frequently reported outcome after pediatric urologic RAS, this was not the case in our study. 19 –21 However, the reason for this incongruity was clear. It is routine in our practice to excise a bladder cuff en bloc with the urachal remnant.
Indeed, 10 out of 14 (71.4%) of the RAS cohort had a partial cystectomy to excise the rim of bladder dome where the remnant was inserted. As a result, we deem it necessary to observe these patients in the hospital overnight. In fact, the only patient we sent home on the day of surgery did not have a bladder cuff removed. Contrarily, only 3 out of 9 (33.3%) of the OA cohort had a bladder cuff excised and all three spent one night in the hospital. Although routine resection of a bladder cuff collectively with the remnant is recommended, there is a difference in opinion among surgeons on which practice is superior, or even necessary, if there is no obvious involvement of the bladder. 22 At this time, long-term implications of the decision to take a bladder cuff remain unknown.
In the reports by Rivera et al. and Ahmed et al., the authors report longer follow-up durations than our findings. 6,17 We believe this to be due to the status of our institution as a tertiary referral center for complex pediatric genitourinary cases from providers in distant counties and adjacent states. Indeed, many patients were instructed to return to their local providers for continued postoperative care, sparing the need and the cost associated with long-distance travel.
With regard to complications, Ahmed et al. reported 1 (6.3%) complication in their series, a bladder leak discovered on POD 2 that required surgical repair (CD grade IIIb). 17 Similarly, we observed a low complication rate (2, 14.3%) although of lesser severity in our RAS cohort: a UTI (CD grade II) in one patient on POD 2 and postoperative pain (CD grade I) in the other on POD 3. It is important to note that both patients had other co-morbid conditions that potentially contributed to these complications. Only 1 (11%) patient in the OA cohort experienced complications postoperatively: superficial cellulitis (CD grade II) around the incision site empirically treated with antibiotics. No patient in our entire cohort experienced complications that may have prolonged their LOS or required re-admission within 1 week of the procedure.
Although undesirable, the complications we encountered in our series are not rare following RAS procedures in children. In a large multicenter study, Dangle and associates examined the nature and incidence of complications occurring in children 90 days perioperatively after robotic urological surgeries. 23 In their series (n = 858), 18 of 59 (30.5%) CD grade I complications were postoperative pain, and 12 of 70 (42.8%) CD grade II complications were UTIs. Notably, the authors found that a majority of CD grade I and II complications were self-limited or were managed conservatively, suggesting that these complications are typically of no long-term consequence if discovered and managed in a timely fashion. In addition, administration of bupivacaine either through direct injection to incisions or as an intraperitoneal aerosol was at the discretion of the surgeon and, thus, not standardized in our series. Although we did not specifically evaluate pain differences based on route of analgesia administration, we do not believe it to be associated with our outcomes.
In addition to the improved 3-D optics and range of motion when robotic assistance is employed, improved patient and parent satisfaction with cosmetic outcomes after robotic surgery compared with open surgery has been well reported. 9,24 –26 Indeed, less scarring has been one of the major appeals of RAS and other MIS techniques. However, as these initially small incisions from traditional port placement grow linearly with the patient, improved cosmesis attributed to MIS becomes marginal. 27 In a recent crowd-sourced survey, Garcia-Roig et al. assessed the impact of scarring on body image in adult patients with surgical scars obtained in childhood. 28
Notably, 54.2% (357/660) of participants were perturbed, to some degree, by their surgical scars and 52.7% (341/647) sensed that previous scars would cause less distress if hidden by underwear. In the same study by Garcia-Roig et al., survey respondents preferred larger incisions from an OA out of clear view or completely covered by undergarments over smaller visible scars from MIS when asked to hypothetically choose for their children. The authors concluded that patients predominantly favored invisibility over size irrespective of familiarity with MIS benefits. 28 Keeping this information in mind, it is therefore within reason to conclude that the optimal approach, then, must both offer the advantages of MIS and virtually eliminate all visible scarring. With the HIdES technique, this prospect is conceivably achieved. 8
With HIdES, laparoscopic trocars are inserted at or below the level of Pfannenstiel incision (Fig. 1). On healing, incision sites are rendered unseen if the abdomen is exposed or if the patient is wearing a bathing suit or undergarments. Notably, HIdES has been demonstrated to leave essential laparoscopic triangulation intact without a rise in laparoscopic instrument collision or compromising surgical ergonomics. 8,9,25 Although we did not explicitly evaluate and compare postoperative appearance of incisions between our RAS and OA cohorts, the smaller scars and decreased visibility of incisions achieved by the HIdES principle is a well-established benefit. 8 –10,25
In addition to the initial description by Gargollo, other studies have discussed the adaptability of the HIdES trocar placement for pediatric RAS and reported favorable perioperative and cosmetic outcomes. 9,25 Indeed, the flexibility afforded by the robotic arms allows a complete excision of the urachal remnant with a bladder cuff and intracorporeal suturing without difficulty. Although the duration of the procedure is notably prolonged, surgical success and outcomes are comparable between groups, and they are congruent with previous published experiences. Indeed, our experience supports utilizing the HIdES port placement technique for urachal excisions. 6,17
Limitations in specialized laparoscopic instrumentation for pediatric patients may also limit the use of RAS among small infants. Smaller working areas in infants may hinder surgical ergonomics, increase frequency of collisions between robotic arms, and potentiate injury hazards. There is no unanimous opinion on age or weight thresholds for RAS; however, older and concomitantly heavier children represent the bulk of patients receiving RAS in urology, and our study was no exception. 21,24 Indeed, patients in our cohort who underwent RAS were significantly older and weighed more than 10 kg at the time of surgery. Thus, we cannot affirm the feasibility of robotic excision of urachal lesions among infants in this weight domain (≤10 kg) despite the promise of our findings. Although RAS in patients weighing less than 10 kg has been reported, 29 further studies assessing generalizability are warranted.
Our study is limited by its retrospective nature and small sample size. The patients of two pediatric urologists and at least two pediatric surgeons were included in our study. The impact of surgeon experience and preferences in perioperative cares on our findings, though unclear, cannot be overlooked. Thus, although we recognize the potential of this technique to achieve greater cosmetic outcomes compared with traditional port placement, further studies validating our findings are encouraged. However, compared with open urachal excision, RAS with HIdES port placement offers notably superior cosmetic outcomes without compromise in surgical quality or convalescence.
Conclusions
Robot-assisted laparoscopic excision of urachal remnants is a safe and feasible alternative to open surgery for pediatric patients with urachal anomalies. We describe the first experience employing HIdES trocar placement principles for urachal remnant excision in children. Complete excision and bladder repair can be achieved by using the HIdES configuration over traditional port placement, allowing for excellent cosmetic outcomes as well as a short hospital stay, low perioperative complication rates, and low narcotic requirements.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.