
Abstract
Purpose:
A large part of the national opioid epidemic has been tied to prescription opioids, leading to a push to reduce or eliminate their use when feasible. The objective of this study was to evaluate outcomes of implementing an Enhanced Recovery After Surgery (ERAS) protocol for patients undergoing ureteroscopic stone treatment with stent placement geared toward minimizing opioid use.
Materials and Methods:
We performed a pre–post study concerning a process improvement project of consecutive patients undergoing ureteroscopic stone treatment with stent placement utilizing a novel ERAS protocol. A lead-in period with patients managed conventionally with opioids was performed before implementation of the ERAS protocol. Data regarding opioid utilization, postoperative outcomes, and patient-reported outcomes, including Patient-Reported Outcomes Measurement Information System (PROMIS), were compared between groups.
Results:
There were 28 pre-ERAS patients and 52 ERAS-managed patients. Patients discharged with an opioid prescription decreased from 93% to 0% (p < 0.05). Mean total morphine milligram equivalent decreased from 60.1 ± 41 to 7.7 ± 26 (p < 0.05). There was no significant difference noted for postoperative calls for pain in the pre-ERAS vs ERAS groups (25% vs 19%, p = 0.9) or in unscheduled provider encounters (0% vs 4%, p = 0.46). There were no clinically significant differences between groups on patient-reported measures.
Conclusions:
Implementation of an ERAS protocol for ureteroscopic stone treatment resulted in a significant reduction in perioperative opioids, a total reduction in discharge opioid prescriptions, and ∼90% reduction in total 30-day postoperative opioid prescribing with no adverse effects on recovery or increase in postoperative clinical encounters.
Introduction
Opioid analgesics have serious risks, including addiction, progression to illicit drug use, and death. The Centers for Disease Control reports that in 2016 nearly 42,000 overdose deaths involved an opioid in the United States. 1 In addition, 75% of heroin users seeking treatment reported an introduction to opioids through prescription drugs. 2
Urinary stone disease is characterized by symptomatic episodes of intense pain, and conventionally this has been managed with opioid medications. Shoag and colleagues showed that opioid use was significantly more prevalent in patients who form renal stones than patients with no history of urinary stones (10.9% vs 6.1%, respectively). 3 Kang and colleagues found that 61% of patients undergoing ureteroscopic management of urinary stones had already received an opioid medication preoperatively, were discharged with an additional opioid prescription, and 12% required an opioid refill within 30 days of surgery. 4
Enhanced Recovery After Surgery (ERAS) protocols involve the standardization of patient care to optimize postoperative recovery after surgery. They have been shown to improve outcomes across a range of surgical procedures, in part through optimization of postoperative pain management through opioid reduction and use of non-opioid multimodal analgesic therapies. 5,6 ERAS within urology has been studied with regard to oncologic procedures such as radical cystectomy 7,8 ; however, it has not yet been applied to benign urologic conditions, such as urinary stone disease. Although there are few studies on non-opioid alternative analgesic interventions for surgical stone patients, the existing evidence suggests that opioids may not be necessary in this population. In a cohort of 52 patients undergoing ureteroscopy and managed with diclofenac instead of opioids, there was no difference in postoperative pain issues compared with an opioid-managed cohort. 9 Successful pain management protocols have been implemented at other hospitals, with one site showing 75% of patients did not require opioids at discharge. 10 These studies were retrospective in nature and could be biased by patient selection. Furthermore, the medication changes made were predominantly in the postoperative discharge period and did not include a multidisciplinary approach.
After performing a needs assessment and gap analysis, we instituted an ERAS care pathway for patients undergoing ureteroscopic surgery with stent placement. We applied the use of nonopioid multimodal analgesic therapies targeting the perioperative period, which “optimizes patient comfort and facilitates functional recovery with the fewest medication side effects.” 11,12 As noted by our anesthesia colleagues, this may not correspond with the lowest pain perception possible. 11,12 The primary objective of this study was to assess the difference in morphine milligram equivalent (MME) prescribed between conventionally managed patients and those being treated with the ERAS protocol. Secondary objectives included postoperative outcomes regarding functional recovery and quality of life (QoL) based on validated questionnaires.
Materials and Methods
We performed a pragmatic pre–post study concerning a process improvement project for ureteroscopic surgery. Institutional Review Board approval was obtained. Patients presenting to a single site for outpatient ureteroscopic stone surgery from August 2018 through December 2018 were included in this prospective observational study. Ureteroscopic surgery was performed by five surgeons and data from one encounter per patient were collected. All patients >18 years presenting for ureteroscopic stone management were included, regardless of stone size, location, laterality, or presence of prior stent. Patients were excluded if a stent was not placed. We collected demographic, perioperative, and postoperative characteristics, including pre- and postoperative opioid use, pain scores, and QoL measures.
One month before initiation of the ERAS protocol, a cohort of patients conventionally managed with opioids was included to provide a comparison group. Upon initiation of the ERAS protocol, systemic administration of opioids was minimized both intraoperatively and postoperatively in all patients and only used when indicated by uncontrolled pain. If a patient was unable to receive a medication within the ERAS protocol (e.g., because of age or renal function), that medication was omitted.
Ureteroscopic stone surgery ERAS protocol
Our ERAS protocol was created as a collaboration between anesthesiology and urology departments and includes preoperative, intraoperative, and postoperative elements (Table 1, full ERAS protocol in Supplementary Appendix SA1). Although the ERAS protocol addresses all phases of care, much of the protocol involved removing or minimizing medications from routine use such as intraoperative and postoperative opioids and ordering medications previously prescribed on an “as needed” basis to a scheduled basis. Preoperatively, a discussion took place between the urologist and the patient regarding the opioid crisis, risks of taking opioids, and the initiative to manage perioperative pain through non-opioid medications. This coincided with a change in Tennessee opioid prescribing laws and most patients were aware of this change. The anesthesia care team reinforced this concept in the holding area on the day of surgery. Intraoperatively, no induction opioids were used if possible, and ketamine and lidocaine were administered unless there was a contraindication. A 4.8F ureteral stent was used as the standard size stent as this was the stent size used for the majority of ureteroscopic stone cases in the comparison group.
Analgesic Components of the Enhanced Recovery After Surgery Protocol for Patients Undergoing Ureteroscopic Stone Surgery
Reduce to 650 mg PO if weight <70 kg. Do not use if history of liver disease.
Reduce to 100 mg PO in patients >65 years of age. Consider not giving in patients >75 years of age. Consider dose reduction to 100 mg in patients with creatinine clearance <30 mL/min or with history of obstructive sleep apnea.
Reduce to 15 mg IV if >65 years of age, creatinine clearance <30 mL/min, or patient weight <50 kg. Avoid if history of gastrointestinal bleed, chronic kidney disease stage IV/V, single kidney, or allergy.
PO = oral administration; PR = per rectum; prn = as needed.
No opioids were prescribed upon discharge. Patients who called the urology clinic with uncontrolled pain were prescribed 12 tablets of tramadol 50 mg or 12 tablets of oxycodone 5 mg if allergic to tramadol. Chronic pain patients remained on their baseline opioid medication(s) with an increase in frequency or dose as needed. Patients requiring further pain control were referred to the Transitional Pain Clinic in the Department of Anesthesiology.
Outcome measures
Demographic data obtained included age, gender, race, American Society of Anesthesiologists (ASA) physical status, chronic opioid use, stone burden, stone location, prestented status, ureteral access sheath use, anesthesia time, and stent duration. Chronic opioid use was defined as a recurring opioid prescription lasting >2 months.
The primary outcome measure was total MME prescribed postoperatively, including initial discharge prescription, refill prescriptions, and new opioid prescriptions, obtained from outside providers within 30 days after surgery. Each prescription category was also assessed individually as a secondary measure. Opioid prescription data were obtained from the Vanderbilt electronic medical record and Tennessee Controlled Substance Monitoring Database (CSMD). Postanesthesia care unit opioid administration was recorded and MME was calculated. Additional secondary outcome measures included patient phone calls, emergent/urgent visits to health care providers, and the results of validated pain and QoL surveys.
Pain and QoL measures
Before surgery, patients completed three questionnaires in the preoperative holding area: the American Urological Association Symptom Index (AUASI), the Patient-Reported Outcomes Measurement Information System (PROMIS) Pain Intensity 3a, and PROMIS Pain Interference 6b. Quality of recovery-15 (QoR-15) surveys were completed through phone within a few days after surgery. The AUASI, PROMIS Pain Intensity 3a, and PROMIS Pain Interference 6b were repeated at follow-up ∼1 week after surgery at the time of stent removal.
The AUASI is a validated measure that has been used to monitor lower urinary tract symptoms in many urologic practices. 13 The National Institutes of Health created the PROMIS instruments to evaluate patient-reported outcomes in a standardized manner across different disease processes, 14 and it has been used effectively to evaluate urolithiasis. 15 –17 The PROMIS Pain Intensity 3a measure was selected to gauge severity and the PROMIS Pain Interference 6b measure was selected to gauge impact on daily life. For PROMIS instruments, there is no perfect definition of meaningful change between patients, conditions, severity, and so on, but a general guideline of half a standard deviation (5) is an estimate of clinically significant change. 18 QoR-15 is a validated questionnaire that has been used to evaluate postoperative recovery after outpatient surgery. 19,20 The score is typically obtained a few days after surgery, and a higher score indicates better recovery.
Statistical analysis
We calculated a need for 29 patients in each arm to detect a difference of 30 MME (equivalent to 1 day of a typical oxycodone prescription) with a power of 80% and a type I error probability of 0.05. Univariate analysis was performed using Student's t-test assuming unequal variances and chi-squared analysis. These results were used to fit linear and logistic multivariable regression models using forward selection. A sensitivity analysis was performed to evaluate the effect of postoperative stent duration. Statistical analysis was performed using STATA v.14 (StataCorp, 2015).
Results
The final study cohort included 80 patients. Data on 30 pre-ERAS patients were collected and after excluding two because of negative ureteroscopies for stones, the final pre-ERAS group of 28 patients had a mean age of 53.8 years with 68% (19) being women. There were 52 patients in the ERAS protocol group with a mean age of 55.8 years with 46% (24) being women. Patient populations were found to be similar with no difference based on demographic or clinical characteristics, including age, gender, race, preoperative opioid use, stone burden, location, case time, or stent duration (Table 2).
Demographics
ASA = American Society of Anesthesiologists; ERAS = Enhanced Recovery After Surgery.
Only 28.8% (15/52) of patients in the ERAS group received opioids in the recovery room with a mean MME of 9.2 ± 5.5. Table 3 shows postoperative outcomes for MME requirement, escalation of pain management, phone calls for pain, and unscheduled provider encounters. Total postoperative opioid prescription dose decreased 87% after implementation of the ERAS protocol (60.1 ± 41 vs 7.7 ± 26). No ERAS protocol patients got an opioid prescription at the time of discharge. There was no significant difference in pre-ERAS vs ERAS groups in the number of patients who required a refill prescription from Vanderbilt University Medical Center (VUMC): 3.6% (1) vs 5.8% (3) (p = 0.4), respectively (Fig. 2). There was no difference in the number of patients who filled an opioid prescription by a provider outside of our institution as identified by the CSMD: 0% vs 3.8% (0 vs 2) (p = 0.2). There was no difference in the number of postoperative phone calls for uncontrolled pain between pre-ERAS and ERAS populations: 25% (7) vs 19% (10) (p = 0.9), or for postoperative provider encounters for pain within 30 days of surgery: 0% vs 4% (0 vs 2) (p = 0.46). No major medical complications (renal injury, urinary retention, etc.) were noted from utilization of the ERAS protocol. All complications were limited to Clavien–Dindo Grade I (opioid prescription for uncontrolled pain), and no Clavien–Dindo Grade II or higher complications occurred.
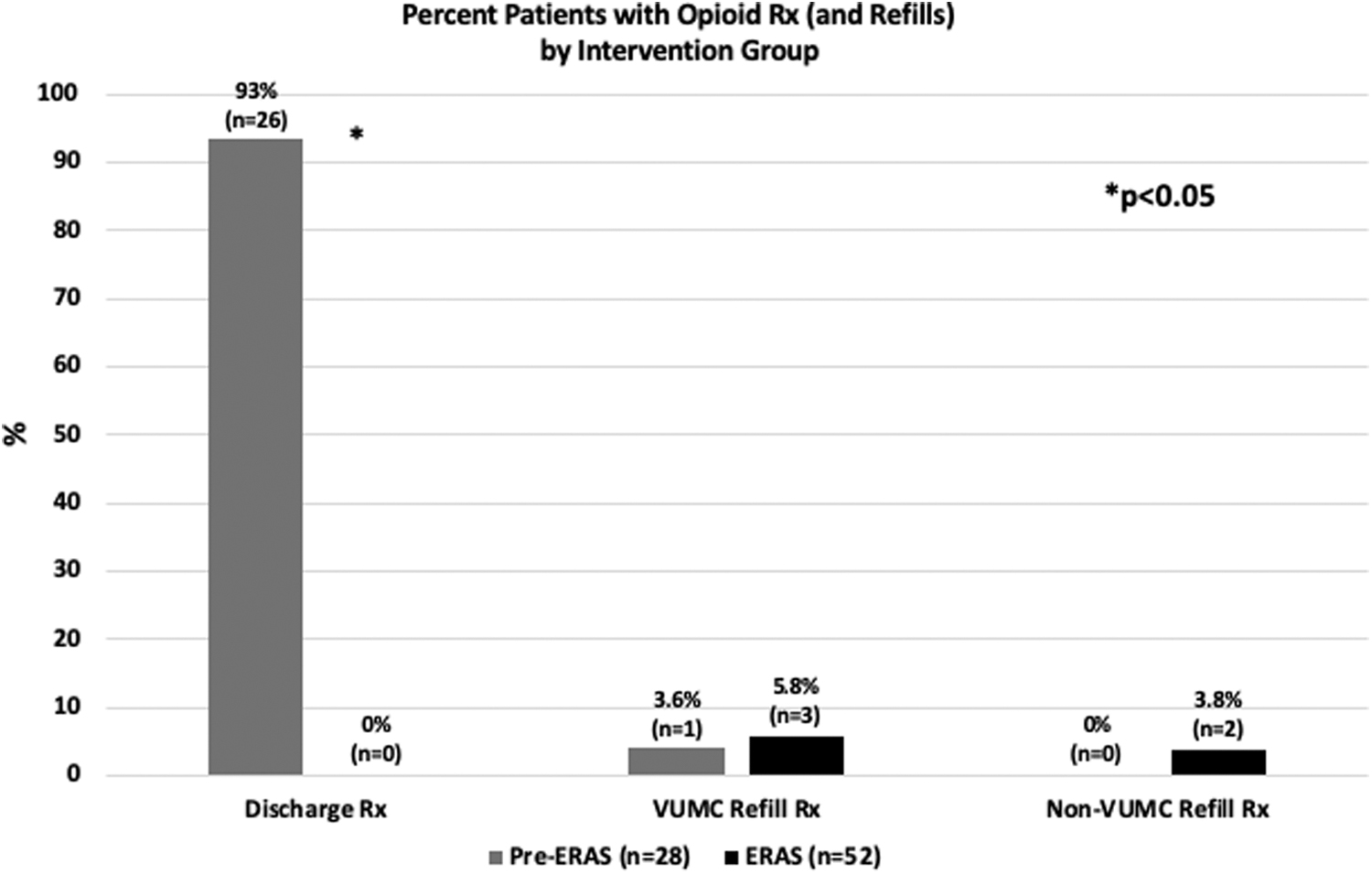
Percent patients with opioid prescription and refills by intervention group. Statistical significance was found for opioid discharge prescriptions between study populations.
Postoperative Outcomes, Multivariable Analysis
Bold indicates statistical significance.
Controlling for age, gender, preoperative PROMIS 3a T score.
Univariate analysis—too few events for multivariable regression analysis.
MME = morphine milligram equivalent; PROMIS = Patient-Reported Outcomes Measurement Information System; VUMC = Vanderbilt University Medical Center.
There was a significant difference in preoperative PROMIS 3a T-scores between the pre-ERAS and ERAS populations, 52.2 vs 47.4, respectively (p = 0.04) (Fig. 1). There was no significant difference in preoperative AUASI (11.4 vs 11.8 (p = 0.83) or PROMIS 6b T-score (60.6 vs 56.9 (p = 0.17) between pre-ERAS and ERAS populations. Based on results of univariate analysis, a multivariable analysis controlling for age, gender, and preoperative PROMIS 3a T-score was performed showing a statistically significant higher score for postoperative PROMIS 3a T-score and postoperative PROMIS 6b T-score (Fig. 1) for the ERAS group relative to the pre-ERAS group. Postoperative AUASI and QoR-15 were not significantly different.
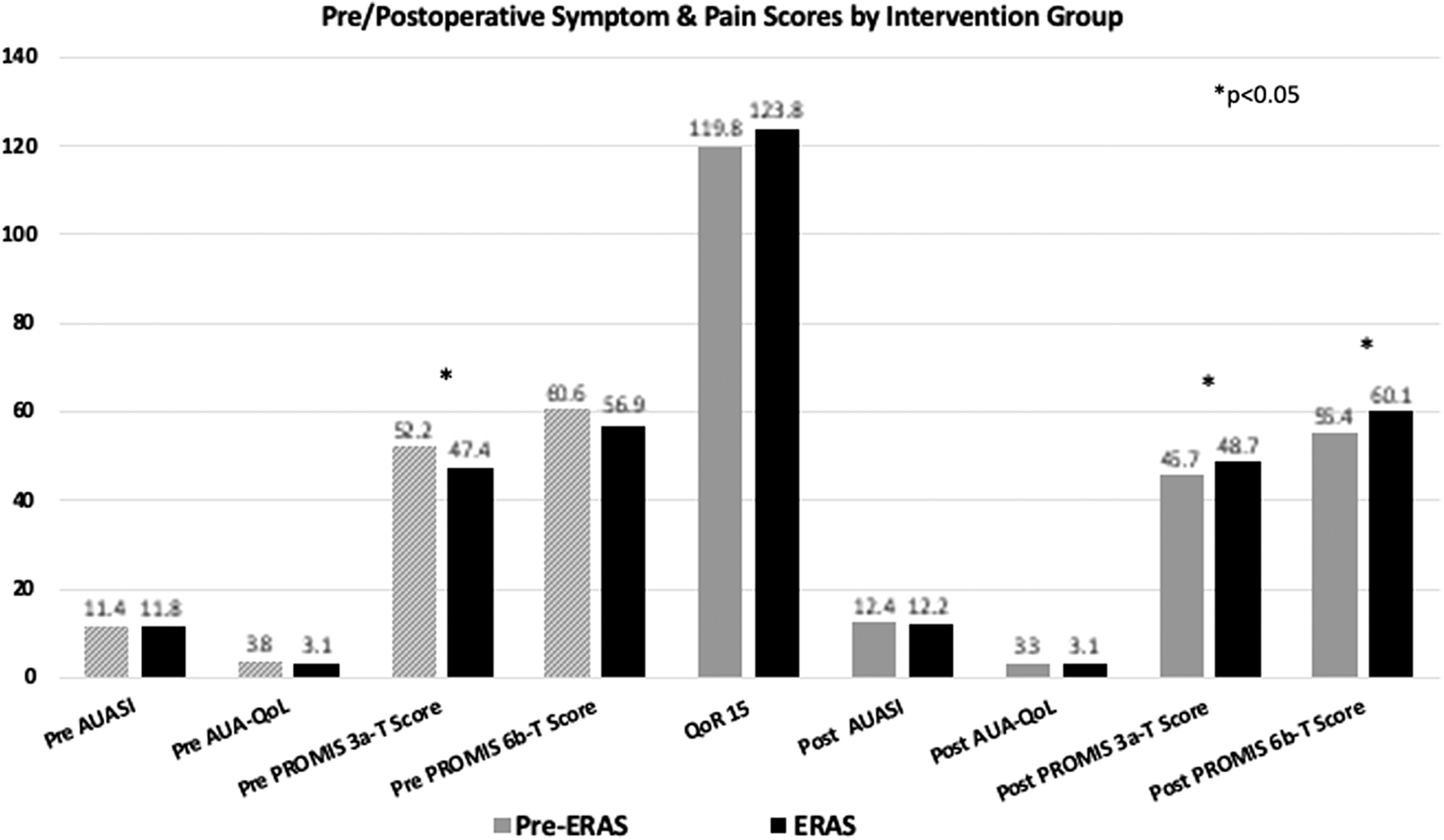
Pre- and postoperative symptom and pain scores by intervention group. Statistical significance was found for pre-PROMIS 3a, post-PROMIS 3a, and post-PROMIS 6b. AUASI = American Urological Association Symptom Index; PROMIS = Patient-Reported Outcomes Measurement Information System; QoL = quality of life; QoR = quality of recovery.
Discussion
Urinary stone disease is a common issue facing a large percentage of the population and many of these patients choose to undergo ureteroscopic management. This procedure has historically been managed with opioids, and the quantities of opioids prescribed have been alarming. Accordingly, we performed a quasi-experimental pre–post process improvement study surrounding the implementation of an ERAS care pathway for ureteroscopic surgery that included principles of opioid minimization and use of nonopioid multimodal analgesic therapies. Our results demonstrate several interesting findings. First, we reduced discharge opioid prescriptions to zero and found no significant difference in requests for opioid refills. Second, we found no adverse effects on clinical encounters such as phone calls or unexpected clinic visits between study populations. Third, we found no clinically significant difference between study populations on several validated instruments. Each of these will be discussed as follows in light of the current literature.
Traditionally, renal colic and pain after ureteroscopic surgery with stent placement has been managed primarily with opioids. Leapman et al. showed in a cohort of >22,000 patients undergoing surgical stone management (86% ureteroscopic), the median number of days opioids were prescribed for patients was 10 and the median total MME dispensed was 180 MME. 21 However, because of the opioid epidemic there has been a large push recently to manage these patients with non-opioid medications. Large et al. and Sobel et al. published retrospective reviews of their early experience of switching to non-opioid management of patients undergoing ureteroscopy with stent placement and found their regimens to be well tolerated. 9,10 These protocols introduced the use of intraoperative ketorolac and belladonna/opium suppositories. We implemented a more comprehensive care pathway that spanned the entire perioperative period, targeted complete opioid avoidance, and prospectively collected patient outcomes. With use of our ERAS protocol, we were able to eliminate all opioid prescriptions on discharge and reduce total postoperative opioid use to near zero without negative effects. We noted no significant change in the number of clinical encounters postoperatively between the two study groups. This includes phone calls for pain, unscheduled provider visits for pain, or opioid prescription refills. Notably, this was true even for patients with chronic opioid use preoperatively.
Our study is unique in that we evaluated several health-related quality measures to ensure that pain severity and QoL were not adversely affected after switching to the ERAS protocol. In situations where a stent is placed temporarily, patients typically note a rise in bothersome voiding symptoms. There was no worsening of voiding symptoms after eliminating opioids as seen on the AUASI. QoR-15 scores showed that ureteroscopic stone surgery remains a challenging procedure from which to recover regardless of how pain is managed. Although the initial creation of the QoR-15 did not categorize severity, recovery has subsequently been interpreted based on the score, with various ranges signifying excellent (136–150), good (122–135), moderate (90–121), and poor (0–89) recovery. 22 The scores noted within our two study arms showed moderate recovery from the procedure with no difference between those managed with opioids and those managed with the ERAS protocol. Our results demonstrated statistically significant mean differences between groups on both the postoperative PROMIS 3a and 6b T-score. The authors believe this to be a statistical finding more so than a clinically significant finding. Although this can be interpreted as comparatively poorer pain control, this did not translate into increased phone calls, clinical encounters, or requests for opioid prescriptions. As described previously, the protocol's intention was to optimize recovery while minimizing adverse medication effects and may not translate to lowest pain perception feasible. Furthermore, a threshold of 60 has been used for defining severe pain 15,16 and both of our study populations possessed means at or below this threshold for PROMIS 3a and 6b suggesting both management strategies adequately control pain.
An important component of the success of this protocol is patient awareness, education, and acceptance. Legislative efforts limiting the amount and duration of narcotic prescribing in Tennessee 23 positively contributed to patient awareness of the potential harms of opioid use and prescribing limitations. Patients were concurrently educated in our clinic and at all phases of perioperative care that the goal was to adequately control pain while simultaneously reducing narcotic utilization. We found patients to be willing to accept the ERAS protocol. We also think there may be a benefit of discharging patients with a written prescription even for over-the-counter (OTC) medications, because we hypothesize patients perceive these medications as having greater efficacy than when dispensed OTC. From a pragmatic perspective, the ERAS protocol was smoothly adopted by both the urology and anesthesia teams, suggesting it could be implemented at other sites and integrated into routine perioperative management for ureteroscopic procedures.
Our study does have some limitations. First, this is a relatively small patient population and thus the results, although positive, require confirmation with larger trials. Although the study was powered to detect the primary outcome, we assessed numerous postoperative outcomes and may not have had the power to detect a difference in every outcome. In addition, our Prescription Drug Monitoring Program only searched opioid prescriptions filled in Tennessee and not outlying states, but 94% (49/52) of the intervention cohort resides in Tennessee. Finally, we cannot say specifically which part of this ERAS protocol allowed the significant reduction in opiate prescribing as the protocol intentionally targets all phases of care as is true in all ERAS protocols and as a quality improvement study was not designed to test the effects of a single intervention. However, much of the protocol involved standardization of medications we were already using or adjusting prn medications to scheduled while still substantially reducing opiate prescribing.
Conclusions
Ureteroscopic stone management with stent placement can result in postoperative pain; however, herein we demonstrate the utilization of an ERAS protocol that permits minimization of perioperative systemic opioid administration, decreased use of discharge opioid medications, and a nearly 90% reduction in total postoperative opioid prescribing within 30 days of surgery. Furthermore, the implementation of this protocol did not result in adverse effects on recovery or increase in postoperative clinical encounters.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix SA1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.