
Abstract
Purpose:
To perform a systematic review and meta-analysis and to assess the clinical benefit of prophylactic pelvic drain (PD) placement after robot-assisted laparoscopic prostatectomy (RALP) with pelvic lymph node dissection (PLND) in patients with localized prostate cancer.
Materials and Methods:
An electronic search of databases, including Scopus, Medline, and EMbase, was conducted for articles that considered postoperative outcomes with PD placement and without PD (no drain) placement after RALP. The primary outcome was rate of symptomatic lymphocele (requiring intervention) and secondary outcomes were complications as described by the Clavien–Dindo classification system. Quality assessment was performed using the Modified Cochrane Risk of Bias Tool for Quality Assessment.
Results:
Six relevant articles comprising 1783 patients (PD = 1253; ND = 530) were included. Use of PD conferred no difference in symptomatic lymphocoele rate (risk difference 0.01; 95% confidence interval [CI] −0.007 to 0.027), with an overall incidence of 2.2% (95% CI 0.013–0.032). No difference in low-grade (I–II; risk difference 0.035, 95% CI −0.065 to 0.148) or high-grade (III–V; risk difference −0.003, 95% CI −0.05 to 0.044) complications was observed between PD and ND groups. Low-grade (I–II) complications were 11.8% (95% CI 0–0.42) and 7.3% (95% CI 0–0.26), with similar rates of high-grade (III–V) complications, being 4.1% (95% CI 0.008–0.084) and 4.3% (95% CI 0.007–0.067) for PD and ND groups, respectively.
Conclusion:
PD insertion after RALP with extended PLND did not confer significant benefits in prevention of symptomatic lymphocoele or postoperative complications. Based on these results, PD insertion may be safely omitted in uncomplicated cases after consideration of clinical factors.
Introduction
Robot-assisted radical prostatectomy (RALP) has become the most commonly used treatment for men with localized prostate cancer. Consistently reported benefits of RALP over open prostatectomy include reduced blood loss and a shorter duration of hospitalization 1,2 for equivalent oncologic and functional outcomes. 2,3 These benefits have led to a wide adoption of RALP in our region and internationally. 3 –6
Intraperitoneal pelvic drain (PD) placement is commonly performed as a standard step after RALP by many robotic centers globally. The rationale for drain insertion is to drain urine, lymphatic fluid, and blood to prevent formation of lymphocele, allow drainage of anastomotic urine leaks and to prevent pelvic hematomas. The risk of lymphocele may be higher after extended pelvic lymph node dissections (ePLND). 7 Potential drain-associated complications include retained foreign body, increased infection risk, drain site pain, and drain site bleeding. The evidence base for benefit of a PD over no drain (ND) is unclear, largely driven by surgeon or institutional preference. 8
Current surgical trends are moving toward enhanced recovery protocols, decreased length of stay (LoS), and early discharge; therefore, omission of routine drain placement can aid in this shift to decreased LoS. Hence, we sought to evaluate the available evidence regarding the benefits of PD use, specifically considering the prevention of lymphocoele and other complications.
Materials and Methods
Evidence acquisition
After registration in the PROSPERO database (registration no. CRD420191280370), a systematic review with meta-analysis was conducted in accordance with the PRISMA statement 9 and Cochrane Collaboration guidelines. 10 The primary outcome was difference in symptomatic lymphocele between the PD and ND groups. The secondary outcomes were postoperative complications according to the Clavien–Dindo (CD) classification. 11
Data sources
The Scopus, Medline, and EMBASE databases were searched in May 2019 using the search strategy outlined in Supplementary Table S1. Database citations were imported into EndNote X9 (Thomson Reuters) with subsequent removal of duplicates and irrelevant articles based on titles, abstract, and full text review according to prespecified eligibility criteria to PRISMA statement guidelines (Supplementary Fig. S1). Two authors (W.Z. and J.S.) independently reviewed the search strategy, determined the eligibility of studies, and performed quality assessment.
Eligibility criteria
Included studies, published in English, considered the outcomes after RALP for localized prostate cancer that reported the use of PD or ND, and then stratified according to whether pelvic lymph node dissection (PLND), or ePLND was performed. PLND is defined as the dissection of external and obturator lymph nodes (LNs), whereas ePLND is defined as the dissection of the external and internal vessels up to the iliac bifurcation in this study. Outcomes included symptomatic and asymptomatic lymphocoele, as well as complications according to the CD classification. Both randomized controlled trials (RCTs) and nonrandomized studies were included to reflect clinical practice and to provide a more complete summary of treatment effect in an area with limited evidence. Exclusion criteria were surgery other than RALP and patients with metastatic disease.
Quality assessment and data extraction
Methodological quality assessment of studies was performed using both the Modified Cochrane Risk of Bias Tool for Quality Assessment for RCTs 10 and the Risk Of Bias In Nonrandomized Studies—of Interventions tool for non-RCTs. 12 Review Manager (version 5) was used to perform and illustrate the quality assessment.
Study characteristics, including sample size, country of study, year of recruitment, type of study, type of intervention, outcome measures (lymphocele and CD complications), and salient issues, were extracted into Microsoft Excel.
Statistical methods
The primary outcome measure was rate of symptomatic lymphocele requiring intervention. Secondary outcomes included the incidence of CD complications (Grade II–V and III–V) between groups. Risk difference (RD) was estimated for comparative studies, whereas incidence estimates were determined according to use of PD or ND within studies. Meta-analysis was performed using the inverse variance heterogeneity (IVhet) model 13 within MetaXL 5.3, 14 with effect sizes expressed as proportions with 95% confidence interval (95% CI). Assessment of effect size heterogeneity was per the Q-statistic (p < 0.1) or τ2> 0, whereas publication bias was assessed using a Doi plot 15 –17 given the small number of studies (funnel plots require a minimum of 10 studies 18 ).
Results
Study selection
After removal of duplicates and citation review, 19 full-text articles were reviewed (Supplementary Fig. S1). Thirteen articles were excluded as they did not assess RALP or did not report the respective proportions of patients receiving drain or ND in their results. 19 –31 As a result, six articles were eligible for inclusion in the evidence synthesis.
Characteristics of included studies
In total, 1783 patients undergoing RALP were included among six studies, comprising two RCTs, 32,33 three prospective case series, 34 –36 and a retrospective data set 37 (Table 1). Three studies (two RCTs and one case series) allowed direct comparison between PD and ND, whereas others reported PD (two studies) or ND (one retrospective study) only. Five studies exclusively evaluated RALP, 32 –36 whereas one study assessed both RALP and open radical prostatectomy. 37 Patient age (reported mean range 61–65 years), prostate-specific antigen (reported mean range 5.1–9.0 ng/mL) and indication for ePLND were similar between studies (Table 1). Although all patients included in this study underwent ePLND, definitions of ePLND and thus the template used were different between studies, whereas marked variability in LN yield was observed (range in mean/median LN yield 10.4–28; Table 1).
Summary of Included Studies
The number of patients in the drain group of this study belongs to the ORP group.
CD, Clavien–Dindo; ECE = extracapsular extension; ELND = extended pelvic lymph node dissection; ePLND = extended pelvic lymph node dissection; LN = lymph node; LND = lymph node dissection; LoS = length of stay; ND = no drain; ORP = open radical prostatectomy; PD = pelvic drain; PSA = prostate-specific antigen; RALP = robot-assisted prostatectomy; RCT = randomized controlled trial; RRP = radical retropubic prostatectomy; SVI = seminal vesicle involvement.
Outcome measures overall were similar with different emphasis, as the primary outcome in the comparative studies 32,33,35 was complicated (reported according to the CD classification system), whereas noncomparative case series 34,36,37 used the primary outcome of lymphocoele incidence based on routine imaging. All studies reported drain removal on day 1–2 postoperatively. 32 –37 Comparative studies reported no difference in complications or symptomatic lymphocoele requiring intervention, whereas noncomparative case series generally reported higher incidence of asymptomatic (9%–20%) compared with symptomatic lymphocoele (1%–5%). Risk of bias assessments (Supplementary Table S2) demonstrated a clear difference based on study design, with included RCTs being rated as low risk of bias, in contrast to nonrandomized studies that were at high risk of bias. 37,38
Lymphocoele
Symptomatic lymphocoele
The use of PD compared with ND among comparative studies showed no difference in symptomatic lymphocoele rate (RD 0.01; 95% CI −0.007 to 0.027; Fig. 1a). When the studies were considered individually according to use of PD vs ND, a marginally higher absolute incidence was observed for PD (0.028; 95% CI 0.018–0.039) compared with ND (0.011; 95% CI 0.003–0.032). No heterogeneity was observed overall or between studies (p > 0.05, I 2 = 0%).
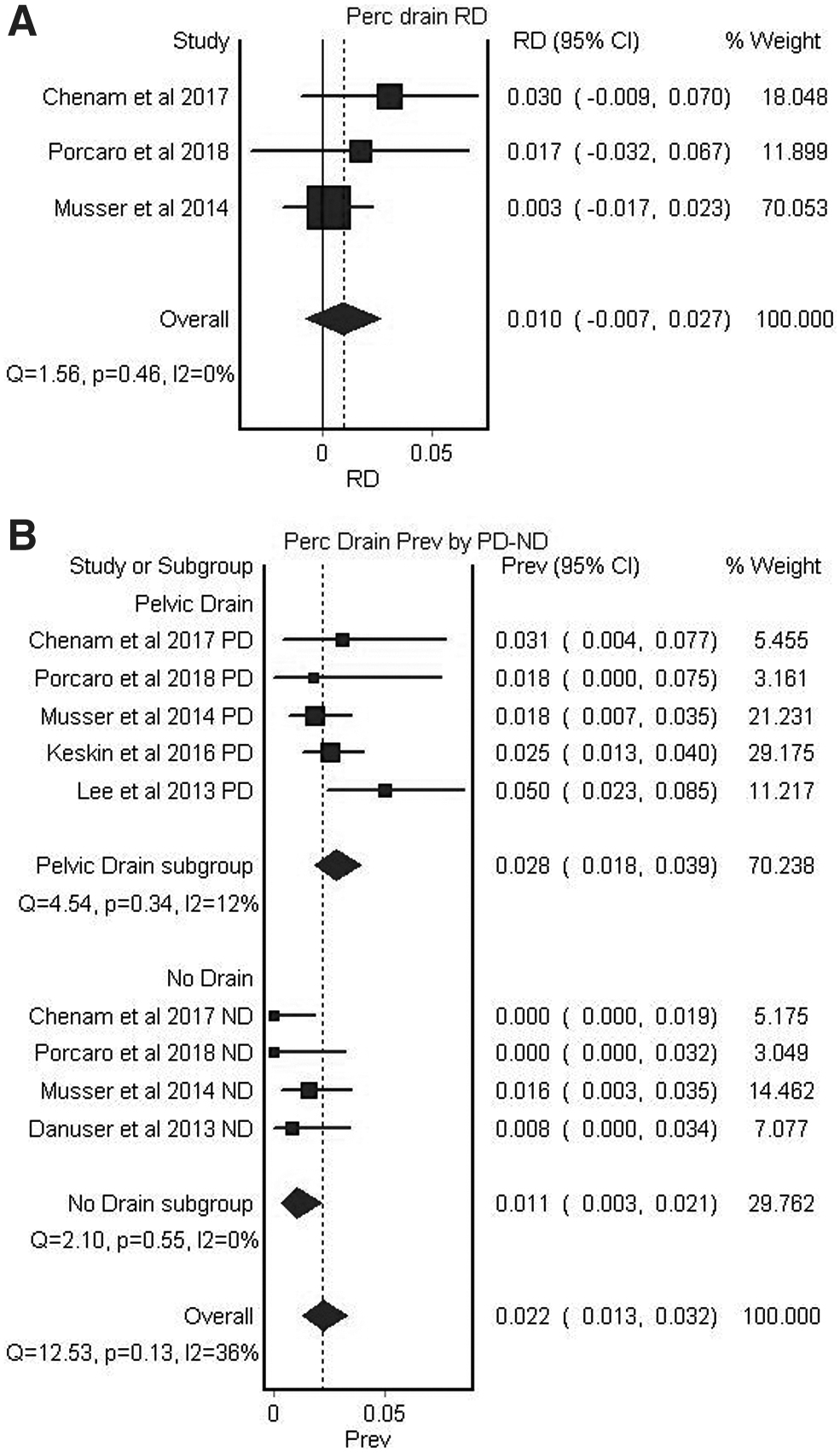
Forest plot after meta-analysis of symptomatic lymphocele rates requiring percutaneous drainage;
Asymptomatic lymphocoele
Pooled estimates from three studies (two with PD, one with ND) with routine imaging to assess for lymphocoele included 10.2% (95% CI 0.016–0.21) overall incidence, in which significant heterogeneity was observed (p < 0.01, I 2 = 93%). Two studies where PD was used reported an incidence of 8.8% 36 and 20.5%, 38 whereas the single study assessing ND reported an incidence of 3.2%. 37
Complications
Among comparative studies reporting complications between PD and ND groups according to the CD system (Fig. 2), there was no difference in low-grade (I–II; RD 0.035, 95% CI −0.065 to 0.148) or high-grade (III–V; RD −0.003, 95% CI −0.05 to 0.044) complications. No heterogeneity was observed overall or between studies (p > 0.05, I 2 = 0%).

Forest plot after meta-analysis of asymptomatic lymphocele rates determined by routine imaging post-RALP.
Incidence estimates for low-grade (I–II) complications were 11.8% (95% CI 0–0.42) and 7.3% (95% CI 0–0.26) for PD and ND groups, respectively, with significant heterogeneity (p < 0.01, I 2 = 95%–97%). High-grade (III–V) complications were similar, being 4.1% (95% CI 0.008–0.084) and 4.3% (95% CI 0.007–0.067) for PD and ND groups, respectively, with borderline heterogeneity (p = 0.05–0.07, I 2 = 55%–62%).
LoS comparison was limited to the proportion of patients staying >1 day in two studies. 32,35 It was estimated that 22% (95% CI −0.03 to 0.46) additional patients stayed >1 day if PD was used, with prevalence estimates of 0.32 (0.08–0.60) and 0.09 (0.06–0.13) for PD and ND groups, respectively (Fig. 3; Supplementary Figs. S2 and S3). Significant heterogeneity (p < 0.01, I 2 = 55%–62%) was noted overall, driven by heterogeneity in the PD group (p < 0.01, I 2 = 95%), whereas the ND group was homogeneous (p = 0.51, I 2 = 0%).
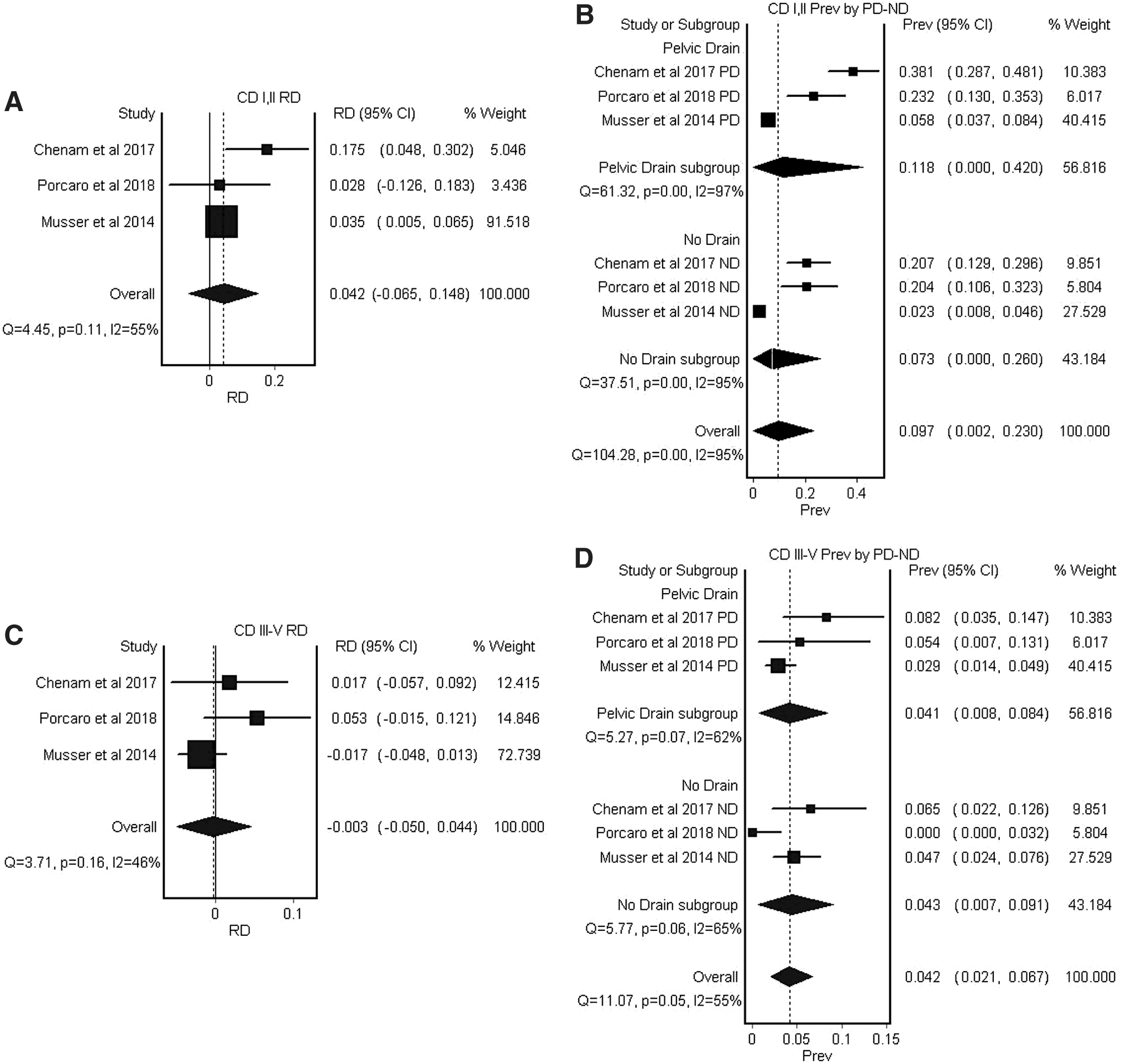
Forest plot after meta-analysis of complications according to Clavien–Dindo classification in comparative studies. Grades I and II,
Discussion
This systematic review and meta-analysis, for the first time to our knowledge, evaluated the available evidence regarding use of PD compared with ND after RALP with ePLND in 1783 patients. Overall, there was no statistically significant difference in the rates of symptomatic lymphocoele or complications after RALP between the PD and ND groups, suggesting drain placement can be safely omitted.
These findings confirm those from previous individual studies in open and laparoscopic prostatectomy. 39,40 The estimates here (2.2%) are less than that reported in a systematic review without meta-analysis (3.1%), which suggested that lymphocoele-related complications are among the most common after RALP with ePLND, 41 whereas ePLND predisposes to a higher lymphocoele rate than limited PLND. 7 Risk factors for development of lymphocoele after ePLND include comorbidity, prostate cancer disease profile such as number of positive LNs, surgical experience, and perioperative use of heparin for deep vein thrombosis (DVT) prophylaxis, 33,34,36 and warrant consideration intraoperatively when deciding to whether or not to place a PD.
Assessment of asymptomatic lymphocoele incidence was limited, as the consequences of an asymptomatic lymphocoele are unclear and thought not to influence outcomes. However, Keskin and colleagues reported that 24% of asymptomatic lymphocoeles persisted at 3 months, with 64% of persistent lymphocoeles eventually becoming symptomatic. 36 Thus, asymptomatic lymphocoele may be an important risk factor for complications, such as intervention for symptomatic lymphocoele, and worth considering in future studies. As such, PLND will continue to be performed and the role of PD use in prevention of PLND-related complications, such as lymphocoele formation, requires consideration. This study suggests no benefit for PD in preventing percutaneous drainage of symptomatic lymphocoeles.
The advent of RALP with improved dexterity and observation in the pelvis has resulted in improved reconstructive techniques, including continuous urethrovesical anastomosis and bladder neck reconstruction (where indicated). Anastomotic leak rates and their ensuing complications are thus low compared with historical series. 42 Independent of urinary reconstruction, other surgical specialties have found limited benefit of postsurgical drain use. 43 –46
Similar to that seen in the current meta-analysis, no clear benefits in terms of length of hospitalization, the need for further intervention and other drain-related complications were found for gynecologic surgeries such as oophorectomy and hysterectomy, or general surgeries such as gastrectomy and cholecystectomy. 43 –46 With this in mind, many robotic surgeons now advocate to omit PD placement for urinary leak prophylaxis if the intraoperative leak test is negative. 47
There are important limitations of this review that should be taken into account when interpreting the findings. First, there is a selection bias as the decision to place a drain was at the discretion of the surgeon. Some factors affecting this decision include hemostasis, extent of LN dissection or presence of urine leak after urethrovesical anastomosis. Furthermore, no studies further stratified the rate of lymphocele in relation to the level of LN dissections, a point that future studies need to address and improve upon. There is data to support that degree of PLND affects the incidence of lymphocele with rates being higher in ePLND. 46, 48
In other types of cancer surgery, such as breast surgery, prophylactic drain insertion reduced the incidence of lymphoceles or surgical collections, as well as the need for further interventions for the collections. 45 But these findings are likely not generalizable to pelvic surgery. We have elected not to discuss the role of ePLND in prostate cancer management as this is a controversial topic outside the scope of this study.
Conclusions
PD insertion after RALP with ePLND does not confer significant benefits in prevention of symptomatic lymphocoele or postoperative complications. Thus, PD insertion can be safely omitted in an uncomplicated case with a watertight vesicourethral anastomosis. Surgical expertise, clinical experience, and patient factors should always be considered within the decision for drain placement. Further studies are required to stratify the degree of LN dissection to lymphocele rate and the subsequent impact of PD insertion, as well as predicting progression from asymptomatic to symptomatic lymphocoele for better identification of patients requiring standard imaging follow-up.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors thank financial supporters of Nepean Urology Research Group (NURG), including TOLMAR, Abbvie, and AstraZeneca.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.