
Abstract
Introduction and Objectives:
After transurethral prostatectomy, erectile dysfunction and ejaculatory dysfunction are significant concerns for patients. We compared ejaculatory hood-sparing technique in patients who underwent photoselective vaporization of the prostate using the GreenLight Laser (EjS-PVP) with the ejaculatory hood-sparing technique in patients who underwent bipolar button plasma vaporization of the prostate (EjS-BPVP) in the surgical management of benign prostatic hyperplasia (BPH).
Materials and Methods:
Twenty-seven patients were randomized to either undergo EjS-PVP or EjS-BPVP from August 2016 to March 2018. All of the patients were sexually active with antegrade ejaculation before prostatectomy. We evaluated International Prostate Symptom Score (IPSS), quality of life (QoL), peak flow rate (Qmax), postvoid residual volume (PVR), International Index of Erectile Function and ejaculatory function by the Male Sexual Health Questionnaire (MSHQ). Men were evaluated preoperatively and at 1, 3, and 6 months postoperatively. The primary outcome was ejaculation preservation measured as no change or preservation in antegrade ejaculate at the last follow-up visit by MSHQ (6 months).
Results:
Twenty-seven patients with a mean age of 65.6 ± 8.4 years underwent either EjS-BPVP or EjS-PVP (Table 1). There were no differences in baseline characteristics between the two groups. Improvements in IPSS, QoL, Qmax, and PVR were durable throughout the study period in both groups. There was no difference in outcomes between groups. Postoperatively, there was no change in ejaculatory function with EjS-BPVP utilizing either 180 W EjS-PVP or bipolar energy. The change in MSHQ Ejaculation Scale was −2.1 and −5.4 at 6 months in both arms. The 6-month ejaculatory preservation rate was 85% in the EjS-PVP group and 78% in the EjS-BPVP group.
Conclusions:
EjS GreenLight photoselective vaporization and bipolar plasma button vaporization is a safe and effective method for treating men with lower urinary tract symptoms secondary to BPH with maintenance of antegrade ejaculation.
Introduction
One of the most common reported complications occurring after benign prostatic hyperplasia (BPH) surgery is retrograde ejaculation. 1 This is a major concern for patients who are sexually active and those who have a continued interest in fertility. The gold standard for treating BPH is the transurethral resection of the prostate (TURP) and can cause up to 70% of retrograde ejaculation. 1,2 GreenLight photoselective vaporization of the prostate (PVP), which uses a high-energy laser, as well as bipolar button plasma vaporization of the prostate (BPVP), which utilizes high-energy bipolar radio frequency plasma energy in a button-shaped tip to vaporize the prostatic tissue, also report high rates of retrograde ejaculation of 67.1%. 3,4
The exact mechanism of ejaculation has not been well defined, classically, the closure of the bladder neck is necessary for antegrade ejaculation. 5 More recently it has been found that, the musculus ejaculatorius, which is located at the mid to proximal end of the verumontanum is the more likely location of this backstop through a mechanistic closure of the paracollicular and supracollicular tissue, also known as the ejaculatory hood. 6,7 Thus, preserving the ejaculatory hood may preserve ejaculation (Fig. 1). We sought to compare ejaculatory hood-sparing PVP (EjS-PVP) to ejaculatory hood-sparing BPVP (EjS-BPVP) in the surgical management of BPH.

Diagram of ejaculatory hood-sparing technique in surgical management of BPH.
Materials and Methods
After IRB approval, 27 patients were randomized to either undergo EjS-PVP or EjS-BPVP from August 2016 to March 2018. All of the patients were sexually active and had antegrade ejaculation before their surgical intervention. Furthermore, patients were diagnosed with lower urinary tract symptoms (LUTS) secondary to BPH, an International Prostate Symptom Score (IPSS) >12, maximum flow rate (Qmax) <15 mL/s, and prostate volume (PV) <80 mL by transrectal ultrasound (TRUS). Patients with a diagnosis of chronic prostatitis, chronic pelvic pain syndrome, urethral stricture, or bladder neck contracture within the past 5 years were excluded. Patients with pre-existing erectile or ejaculatory dysfunction were also excluded.
Patients were assessed at baseline, 1, 3, and 6 months postoperatively. Patient characteristics, perioperative and postoperative parameters were compared across groups. The primary outcome, ejaculation preservation, was measured through the Male Sexual Health Questionnaire (MSHQ) as no change or preservation in antegrade ejaculate at the last follow-up visit (6 months).
Secondary outcomes included Short Form Health Survey (SF-12), overactive bladder questionnaire-short form (OAB-SF), International Prostatic Symptom Score (IPSS), and quality-of-life scores. Other parameters assessed included free flow uroflowmetry, postvoid residual urine measurement (PVR), PV, and prostate-specific antigen (PSA).
Patients in this study were treated by two surgeons (B.C. and A.E.T.) at a single center. Both EjS-BPVP and EjS-PVP were performed with the same technique. The procedure commenced at the prostatic apex with careful removal of the apical tissue to protect the verumontanum and the external sphincter by only resecting tissue up to about 0.5 to 1 cm above the verumontanum laterally and proximally preserving the ejaculatory hood to provide a backstop during ejaculation. The end of the procedure was a TURP-like cavity lined by capsular fibers with preservation of the ejaculatory hood (Fig. 1). The prostatic urethra was viewed from the apex with a 30° lens to ensure adequate resection of tissue. No tissue was projecting into the visual field when the bladder was full. Before concluding the procedure, the prostatic cavity was inspected for bleeders by partially draining the bladder and turning off the irrigation to reduce hydrostatic pressure. At the end of the procedure, the bladder was filled with the irrigation solution and the cystoscope removed. A 20F Foley catheter was inserted in all patients and left to gravity drainage.
The total sample size for the study was 27 patients. For this trial, the objective was to detect a difference of 25% in MSHQ scores. For a type 1 error of 0.10, a power of 0.80, it was anticipated that groups of equal size were required. The total sample size required to achieve these objectives was at least 22 subjects per arm. With an attrition rate of 10%, 24 subjects per arm were required. The study also planned for a futility analysis when 50% of patients completed follow-up.
The study enrolled half of the study sample size in each arm, and followed up with patients until all these patients completed the primary endpoint assessment. An interim analysis was performed and the conditional power was computed with the estimated treatment effects from these patients and the planned total sample size for the study. The interim analysis was performed by an independent statistician and the specific study results were not shared with the study investigators, site personnel, and patients. There were three potential outcomes based on the conditional power at the interim analysis: (1) conditional power <50%, stop for futility, (2) 50% to 80% conditional power, continue with sample size reestimation, and (3) ≥80% conditional power, continue the study with the original sample size. Given the findings at the interim analysis, the study protocol was terminated.
Power analysis
After enrollment, the patients were randomly allocated with a fixed block size of 2. Both blocks were equal and the order of treatments within the block was randomly permuted. A random number sequence was used to choose a particular block. Patients allocated into group A underwent EjS-PVP and patients in group B underwent EjS-BPVP.
This study was not intended as a registration trial and was designed to screen for an early indication of efficacy. Therefore, the statistical design using a one-sided 0.10 alpha level was chosen to minimize type I error within the constraints of what was feasible in terms of patient accrual. The use of a one-sided 0.10 alpha level is recommended when performing randomized phase II studies.
Statistical analysis
The differences in patient characteristics and perioperative parameters between the two groups were analyzed using a t-test. Success or failure of the ejaculation preservation in the two groups was analyzed using a chi-square test. A two-sided p-value of 0.05 was considered statistically significant.
Results
A total of 27 patients with a mean age of 65.6 ± 8.4 years underwent either EjS-BPVP or EjS-PVP (Table 1). The mean body mass index was 27.7 ± 5.4 kg/m2. About half (48.1%) of patients had a prior diagnosis of hyperlipidemia, and patients had a mean Charlson Comorbidity Index of 2.7. The mean baseline PSA was 3.3 in the EjS-PVP group and 4.2 in the EjS-BPVP group (p = 0.692). There were no statistically significant differences in preoperative baseline characteristics between the two groups.
Baseline Patient Characteristics
Student's t-test.
EjS-BPVP = ejaculatory hood-sparing bipolar button plasma vaporization of the prostate; EjS-PVP = ejaculatory hood-sparing photoselective vaporization of the prostate; PSA = prostate-specific antigen; SD = standard deviation.
Patients in both the EjS-PVP group and the EjS-BPVP group had a baseline mean IPSS of 18 (range 5–34), as shown in Table 2. There was an overall postoperative decrease in IPSS in both groups as seen in Figure 2. At 3 months posttreatment, there was a mean change (Δ) of IPSS of −8.3 and −11.3, respectively, in each group, and this trend was also evident at 6 months postoperatively with an IPSS mean change of −11.2 and −13.5, respectively (p = 0.535) (Table 3). Figure 3 shows the mean change in voiding function. In both the EjS-PVP group and EjS-BPVP there was no significant change in PVR or Qmax 6 months postoperatively.

Postoperative mean change in urinary symptoms.
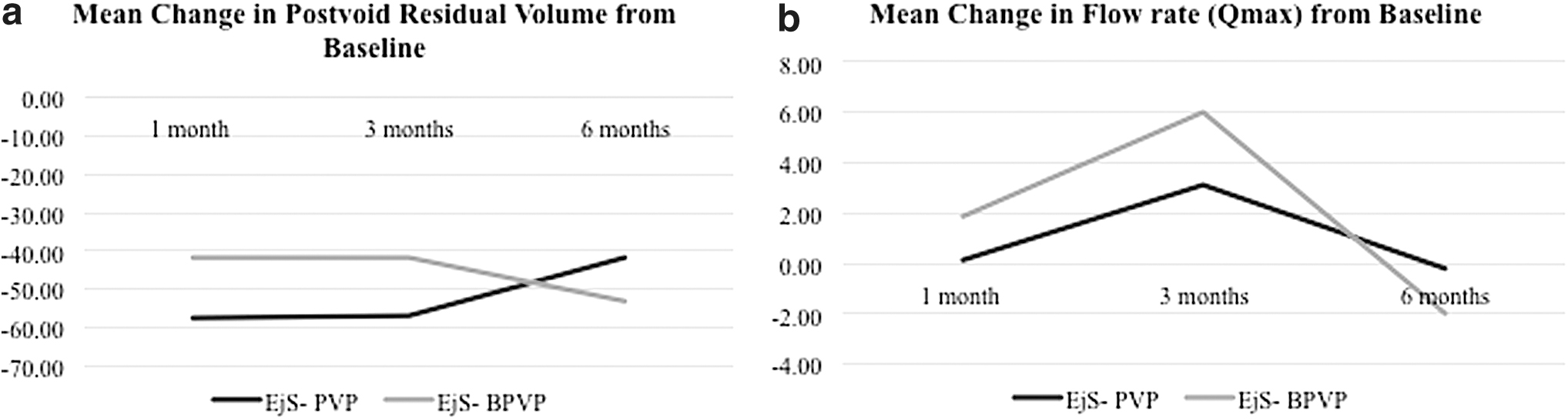
Postoperative mean change in voiding function.
Baseline and Postoperative Mean Values of Lower Urinary Tract Symptoms
Student's t-test.
IPSS = International Prostate Symptom Score; OAB-SF = overactive bladder questionnaire-short form; PVR = postvoid residual volume; SF-12 = short form health survey; QoL = quality of life.
Postoperative Change in Lower Urinary Tract Symptoms from Baseline
Student's t-test.
Patients in the EjS-PVP group and the EjS-BPVP group had a baseline mean OAB-SF score of 79.1 ± 44.7 and 65.8 ± 38.0, respectively, as shown in Table 2. There was an overall 6-month postoperative decrease in OAB-SF scores in both groups as seen in Figure 2. At 3 months postoperatively, there was a mean change of OAB-SF scores of −26.7 and −22.0, respectively. However, at 6 months both groups showed a mean change of −44.1 and −37.1, respectively (p = 0.568) (Table 3).
Patients in the EjS-PVP group had a baseline mean total MSHQ of 61.3 ± 28.9, while the EjS-BPVP treatment group had a mean baseline total MSHQ of 67.7 ± 30.7 (Table 4). The mean change in total MSHQ score 1 month postoperatively was 0.92 in the EjS-PVP group and −18.0 in the EjS-BPVP group. At 6 months, the mean change in total MSHQ was −3.5 and −19.6, respectively (p = 0.347) (Table 5). Figure 4 shows the mean change in total MSHQ, Ejaculation Scale, and Erection Scale 1, 3, and 6 months postoperatively. The mean Ejaculation Scale 1 month postoperatively was unchanged in the EjS-PVP group but decreased at 6 months (18.1 vs 9.8). A similar trend was observed in the EjS-BPVP group, with a mean change of −7.2 at 1 month postoperatively, and −5.36 at 6 months (Table 5). Figure 4 also indicates an increase in the mean change in the Erection Scale in both groups at 3 months with a decline at 6 months. The mean change in Erection scale at 6 months was −1.07 in the EjS-PVP group and −2.29 in the EjS-BPVP group (p = 0.601).
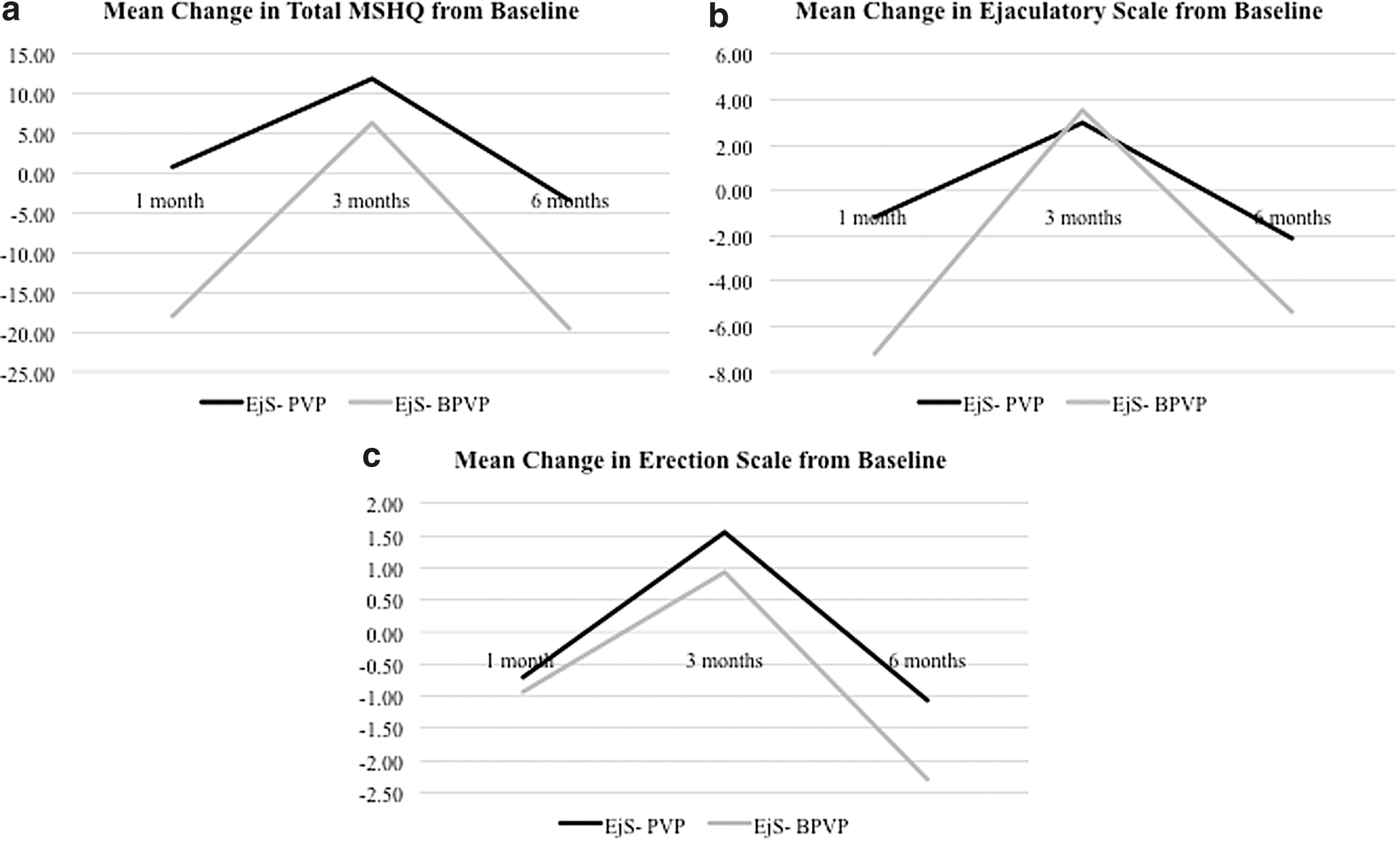
Postoperative mean change in sexual function.
Baseline and Postoperative Mean Values of Sexual Function Parameters
Student's t-test.
MSHQ = Male Sexual Health Questionnaire.
Postoperative Change in Sexual Function Parameters from Baseline
Student's t-test.
At baseline, the mean SF-12 was 50.2 ± 23.3 in the EjS-PVP group and 35.7 ± 23.8 in the EjS-BPVP group (Table 2). There was an increase in postoperative SF-12 in both groups, as demonstrated in Figure 2. The mean change in SF-12 from baseline was greater in the EjS-BPVP group than the EjS-PVP group at all time points, with a 6-month mean change of −7.5 and 0.57, respectively (p = 0.485) (Table 3).
Discussion
We found no change in ejaculatory function with EjS-BPVP utilizing either 180 W EjS-PVP or bipolar energy. The change in MSHQ Ejaculation Scale was −2.1 and −5.4 at 6 months in both arms. The 6-month ejaculatory preservation rate was 85% in the EjS-PVP group and 78% in the EjS-BPVP group. These findings were similar to a study by Alloussi et al., who demonstrated a rate of 90.8% of ejaculation preservation using ejaculation-preserving TURP with avoidance of paracollicular digging. This study utilized the Wolff 24F high-flow resectoscope to perform a monopolar resection. The procedure involved cutting 1 cm proximal of the verumonatum, complete resection of the middle lobe, and resection of lobes lateral to the capsule. This was followed by circular resection of the bladder neck and apical resection with the distal resection border determined by the colliculus seminalis. 10 Our study was able to utilize a similar technique with a bipolar or laser energy source and demonstrate that there is similar efficacy in preserving ejaculatory function.
Another study by Leonardi et al. showed a success rate of 96% in ejaculation preservation following a laser vaporization prostatectomy with a 980 nm laser using a urethral mucosal triangle-sparing method. This strategy involved engraving the ejaculatory triangle from the bladder neck at 5 and 7 o'clock. This was followed by progression downward, and bilaterally upward about 2 mm from the seminal colliculus. Prostate tissue was lifted to create furrows that were then ablated using a “lifting and rolling” technique. This strategy spared the verumontanum, the bilateral prostatic apex, as well as bladder neck muscle fibers. 8
A recent study in April 2019 by Abolazm et al. used an EjS technique vs standard technique of GreenLight laser PVP to assess sexual function. This study found that EjS-PVP had an antegrade ejaculation rate of 85% vs 32% using standard PVP. The group also reported a significant reduction in the Ejaculation Scale MSHQ score after standard PVP but no difference after EjS-PVP, as demonstrated in our study. 12,13,14 Additionally, a study by Tabatabaei et al. additionally reported on PVP using a technique that preserved the bladder neck, precollicular tissue, and the paracollicular tissue. This group demonstrated ejaculation preservation at a rate of 87.5%, further supporting use of ejaculation-sparing techniques in BPH surgery using PVP. 11
In addition to evaluating ejaculatory preservation, our study found that there was a trend toward better ejaculatory function in the EjS-PVP, but these findings were not statistically significant. This has been observed in similar studies such as Ouyang et al., who showed in a prospective trial that the use of the 160 W PVP resulted in International Index of Erectile Function-5 scores that decreased at 3 months but returned to baseline at 6 and 12 months postoperatively. This study concluded that the 160 W PVP technique did not increase the risk of erectile dysfunction. 15 This has been seen in several similar studies, and further supports our results in which erectile function, as measured by the Erection Scale Subscore of the MSHQ, was unchanged in both the PVP and EjS-BPVP groups.
Ejaculation is one of the fundamental components of sexual function and occurs through an emission and expulsion phase following stimulation of the glans penis. 8 Activation of the autonomic nervous system leads to release of seminal fluid into the prostatic urethra. Contraction of pelvic floor muscles allows for expulsion, with prevention of retrograde ejaculation by intact bladder neck closure. In the surgical treatment of BPH, TURP has been utilized as the gold standard. 1,3 However, one of the most commonly reported complications of TURP is retrograde ejaculation, characterized by the retrograde passage of semen. The typical technique of transurethral resection involves the resection of obstructive tissue at the bladder neck and removal of apical tissue around the verumontanum. These have been thought to contribute to a loss of the normal antegrade ejaculatory mechanism because of incompetence of the bladder neck to close. Recent studies contest this hypothesis, showing on TRUS that antegrade ejaculation can occur even in the absence of bladder neck closure and that preservation of the paracollicular tissue and the ejaculatory hood is crucial. Therefore, ejaculation-sparing techniques have been increasingly implemented in BPH surgeries. Applying these methods, several groups have reported ejaculation preservation at rates of up to 80% to 96%. 9
Our study utilized an EjS technique in both EjS-BPVP and GreenLight laser PVP treatment groups. Our study demonstrates that utilizing these techniques, both energy sources were able to spare ejaculatory function from baseline as demonstrated by the very small change in MSHQ scores at all postoperative time points. However, the PVP group demonstrated a trend toward greater preservation of ejaculation function as measured by the Ejaculation Scale in the MSHQ. Additionally, overall sexual function (as measured by total MSHQ score) was preserved to a greater extent in the PVP group than the BPVP group 6 months postoperatively, but this was not statistically significant.
Both techniques utilized in the present study were safe with minimal complications. Overall, complications were similar in the study group vs the control group. Patients in both study groups reported minimal postoperative dysuria. There were no differences in perioperative and postoperative complications according to Clavien–Dindo classification.
There are a few limitations in our study. First, there was a small sample size and based on the interim analysis the study was terminated. The present study was limited to patients with prostates 80 mL or less. Future studies are needed to evaluate the efficacy of these ejaculatory hood-sparing techniques in patients with larger prostates, potentially in combination with other techniques such as enucleation. Additionally, the present study utilizes subjective parameters of postoperative ejaculatory function. Future studies with larger sample sizes are needed to correlate and validate these subjective findings with objective parameters of ejaculatory function, including semen volume. Despite these few limitations, this is one of the first randomized studies to compare ejaculation-preserving GreenLight and bipolar energies with 6 months of follow up. Ultimately, utilizing this technique, ∼92% of patients preserved antegrade ejaculation through sparing of the paracollicular and supracollicular tissue.
Conclusions
EjS GreenLight photoselective vaporization and bipolar plasma button vaporization is a safe and effective method of treating men with LUTS secondary to BPH with maintenance of antegrade ejaculation.
Footnotes
Author Disclosure Statement
B.C. is a consultant for Boston Scientific, Olympus, Meditate. For M.K., A.E.T., J.A.K., and S.K.: No competing financial interests exist.
Funding Information
This study was supported by an unrestricted grant by Boston Scientific.