
Abstract
Aims:
To compare the 30-day postoperative complications of robotic radical cystectomy (RRC) vs open radical cystectomy (ORC) in obese patients (body mass index ≥30) with bladder cancer (BC).
Methods:
The National Surgical Quality Improvement Program database was queried to identify obese BC patients who underwent RRC or ORC between 2005 and 2016. Patient demographics, postoperative mortality rate, morbidity, operating time (OPTIME), length of stay (LOS), readmission, and reoperation rates were recorded and compared between the two groups. Each RRC patient was matched with three ORC patients using a propensity score approach.
Results:
Four hundred forty-two RRC patients were matched with 1326 ORC patients. No difference in early postoperative mortality rate between RRC and ORC (0.7% vs 1.3%, relative risk, RR [95% confidence interval CI]: 0.27 [0.07–1.02]). Compared with ORC, the RRC group showed shorter mean OPTIME (364.7 [standard deviation, SD = 133.4] vs 387.8 [SD = 129.7] minutes, p = 0.001) and mean LOS (7.1 [SD = 5.6] vs 10.6 [SD = 6.6] days, p < 0.001). Compared with ORC, the RR of developing the following events in RRC group was lower: 30-day postoperative any complication (45%), any wound occurrence (64%), blood transfusion (70%), superficial surgical-site infection (78%), and wound disruption (77%). There was no difference in the RR of any-cause readmission (RR [95% CI]: 0.77 [0.57–1.05]) and reoperation (RR [95% CI]: 0.48 [0.22–1.04]) between the two groups.
Conclusions:
The study revealed that RRC for obese BC patients is associated with shorter OPTIME, shorter LOS, and lower risk of early postoperative complications when compared with a matched group of patients who received ORC. In addition, no difference in early postoperative mortality rate between RRC and ORC was observed.
Introduction
Obesity (body mass index [BMI] ≥30) has emerged as a growing challenge in patient care in the United States as the prevalence is close to 36% in the adult population. 1,2 Obesity is associated with higher morbidity and postoperative complications following urologic procedures. 3 Previous researchers have focused on postoperative outcomes of radical cystectomy (RC) among obese patients. However, there remains conflicting evidence regarding the effects of obesity on perioperative complication rate and mortality rate in RC patients. Arora and colleagues observed that high BMI was associated with a higher complication rate in RC patients, while Tyson and colleagues did not. 4,5 On the contrary, Bagrodia and coworkers reported a lower likelihood of perioperative complications in obese than normal weight patients except for transfusion rates, which added more controversy to the role of obesity in the management of bladder cancer (BC) patients. 6
Robotic radical cystectomy (RRC) was first described by Menon and colleagues in 2003 where robotic approach allowed for precise and rapid removal of the bladder with minimal blood loss. 7 Subsequently, RRC starts to gain popularity owing to the magnified visualization, improved precision of dissection, and eventually better postoperative outcomes in terms of shorter hospital stay and lower rate of short-term and long-term complications. 8 However, treatment outcomes of RRC have remained unknown in specific subgroups of patients such as obese patients. Robotic surgery may be more difficult in obese patients due to the complexity of patient positioning, limited access and visualization of surgical field, and limited range of motion for the robot arms. 9 Some experts in the field have also discussed that the comorbidities generally associated with higher BMI such as metabolic derangement, hypertension, and diabetes pose a significant risk against the success of robotic surgery in obese patients. 10 In addition to the concerns associated with the Trendelenburg position for a prolonged period in the obese patient, the thick intra-abdominal fat can pose significant obstacle to RRC in this patient population. 11 Although there are several reports that compared the outcomes of RRC with open radical cystectomy (ORC), 12 –14 to the best of our knowledge, no study has compared the early postoperative outcomes of RRC vs ORC in the obese BC patients.
In this study, we assessed the 30-day postoperative morbidity and mortality rate of obese patients who underwent RRC for BC and compared them with a propensity matched group of ORC patients. We utilized the National Surgical Quality Improvement Program (NSQIP) of the American College of Surgeons (ACS). We hypothesized RRC is associated with better early postoperative outcomes than ORC in the obese BC patient.
Materials and Methods
Data source and patient population
The NSQIP-ACS data set from 2005 to 2016 was utilized. The NSQIP data are deidentified and include information on patient demographics, comorbidities, perioperative morbidity and mortality rate within 30 days of surgery from the participating hospitals in the United States. We queried NSQIP for all adult patients with a BMI >30 kg/m2 (i.e., obese) who received RC for BC between 2005 and 2016. We classified them into two groups: ORC and RRC. Common Procedural Terminology (CPT) codes 51570, 51575, 51580, 51585, 51590, 51595, 51596, and 51597 were used to identify patients who received ORC and CPT 51999 was used to identify those who received RRC. Urinary diversion in both groups was identified and categorized as ileal conduit (CPT—51590, 51595, and 50820) and neobladder (CPT—51596 and 50825).
Study measures
Postoperative mortality rate and the common reported complications occurring within 30 days of receiving RRC/ORC in obese patients were identified. An indicator for “any complication” within 30 days was also created if at least one complication was reported. An indicator for “any wound occurrence” within 30 days was also created if at least one of the following complications was reported: surgical-site infection (SSI) or wound disruption. The length of stay (LOS, days), operating time (OPTIME, minutes), readmission, and reoperation rates were reported as well.
Statistical analyses
Each RRC patient was matched with three ORC patients using propensity score (PS) methods. A PS model was built to determine the probability of receiving RRC depending on the observed patient demographics and comorbidities (Table 1). Chi-square and Student t tests were used to evaluate differences between the two groups, based on the variable type. A modified Poisson regression model with log link was used to determine the relative risk (RR) of postoperative mortality rate and complications in RRC (vs ORC) patients adjusting for the 1:3 matched design and type of diversion. All the analyses were conducted in SAS® v9.4 (SAS Institute, Inc., Cary, NC).
Pre- and Postmatch Patient Characteristics, Length of Stay, and Operating Time of Robotic Radical Cystectomy vs Open Radical Cystectomy
1:3 Patients were matched based on the probability of receiving “robotic cystectomy” given all the above characteristics except length of stay and operating time.
ASA = American Association of Anesthesiologists; COPD = chronic obstructive pulmonary disease; ORC = open radical cystectomy; PRBC = packed red blood cell; RRC = robotic radical cystectomy; SD = standard deviation.
Results
We identified 442 obese patients who underwent RRC and were matched to 1326 obese patients who received ORC. Study flowchart is provided in Figure 1.
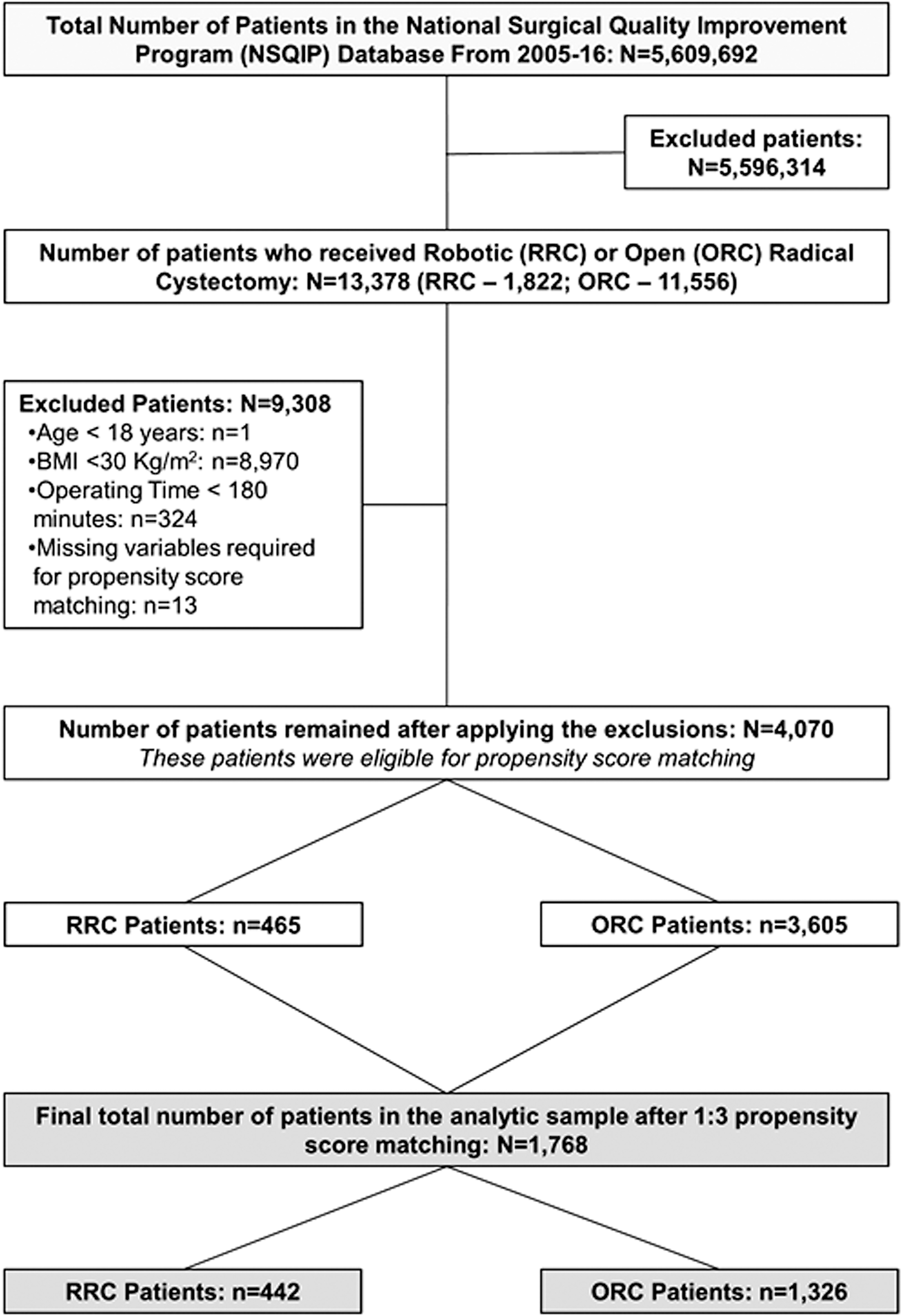
Study flowchart.
Patient characteristics
After matching, all patient characteristics were well balanced between the two groups. Majority of patients in both groups (RRC-ORC) were aged 65 to 74 years (37%–38%), males (75%–78%), white (84%–85%), nonsmoker (81%–82%), functionally independent (98%–99%), received RC post-2009 (∼97%), and were American Association of Anesthesiologists (ASA) Class III (∼64%). Hypertension (65%–66%), diabetes (25%–27%), and chronic obstructive pulmonary disease (∼5%) were the most frequent comorbid conditions between both groups. As to the type of urinary diversion, however, being underreported in the RRC group (76% missing), ileal conduit was the predominant procedure in both groups (68% in ORC and 19.5% in RRC) (Table 1).
LOS and OPTIME
Both the average LOS (days ± standard deviation [SD]) and the mean OPTIME (minutes ± SD) were significantly shorter in RRC vs ORC (7.1 ± 5.6 vs 10.6 ± 6.6, p < 0.001, and 364.7 ± 133.4 vs 387.8 ± 129.7, p < 0.001), respectively (Table 1).
Postoperative mortality rate
The overall 30-day mortality rate was low in both groups (0.7% [n = 3] in RRC and 1.3% [n = 17] in ORC) (Table 2). After adjusting for matched study design and type of diversion, there was no statistically significant difference in the RR of postoperative mortality rate between the two groups (RR [95% confidence interval, CI]: 0.27 [0.07–1.02]).
30-Day Postoperative Mortality Rate, Morbidity, and Relative Risk of Complications in Patients Receiving Robotic Radical Cystectomy vs Open Radical Cystectomy
“Any wound occurrence” is defined as presence of either superficial SSI, deep incisional SSI, organ space SSI, or wound disruption.
Each RR estimate is obtained from separate regression model adjusted for 1:3 matched design and type of diversion. If the 95% CI for the RR does not include 1, then the difference is significant and p-value is <0.05.
CI = confidence interval; CPR = cardiopulmonary resuscitation; DVT = deep venous thrombosis; RC = radical cystectomy; RR = relative risk; SSI = surgical-site infection; UTI = urinary tract infection.
Postoperative complications
Incidence of “any complication” in the RRC group was significantly lower than ORC (28.3% vs 56.6%) as well as for “any wound occurrence” (6.3% vs 18.6%). Incidence of specific complications between the two groups is illustrated in Table 2. After adjustment, the risk of “any complication” and “any wound occurrence” was 45% and 64%, lower in RRC patients compared with ORC patients. Also, the risk of blood transfusions, superficial SSI, and wound disruption were significantly lower in the RRC patients compared with ORC patients. There was no significant difference in the risk of the following complications between the two groups: urinary tract infections (UTI), deep venous thrombosis (DVT), renal impairment, myocardial infarction, cerebrovascular accident/stroke, sepsis, organ space SSI, deep incisional SSI, septic shock, pneumonia, pulmonary embolism, and unplanned intubation (Table 2). We found that patients who had more than one complication were more prevalent in the ORC group than in the RRC (25% vs 12.4%) (Table 3).
Number of Complications in Robotic Radical Cystectomy vs Open Radical Cystectomy Group
SE = standard error.
Readmission characteristics
Readmission rate was lower in the RRC group (17.3%) compared to the ORC (24.2%). However after adjusting for diversion, there was no difference in RR of any-cause readmission (RR [95% CI]: 0.77 (0.57–1.05)) between the two groups. In both groups, the mean duration between discharge and any readmission was similar (16 days). UTI, sepsis and space SSI (i.e., pelvic collection) were the most commonly recorded causes of readmission (Table 4).
Readmission and Reoperation Characteristics in Robotic Radical Cystectomy vs Open Radical Cystectomy Group
Indicates all the reoperation procedures with frequency of occurrence of ≤3 in ORC and 1 in RRC.
Reoperation characteristics
Reoperation rate was lower in the RRC group (2.9%) compared with the ORC (5.8%). However, after adjusting for type of diversion, there was no difference in RR of any-cause reoperation (RR [95% CI]: 0.48 [0.22–1.04]) between the two groups. The most common cause of reoperation in both groups was exploratory laparotomy. Other causes of reoperation in the ORC group were resection of small intestine and secondary closure of abdominal wall dehiscence (Table 4).
Discussion
In this study, using the NSQIP database, we compared the 30-day postoperative morbidity and mortality rate of RRC vs ORC in obese BC patients. To reduce selection bias, we utilized a PS matching approach to match RRC patients with ORC patients. Our study revealed significant differences in average OPTIME and LOS with them being shorter in RRC patients compared with ORC. The RRC group was associated with significantly less rates for any complication, any wound occurrence, bleeding requiring blood transfusion, superficial SSI, and wound disruption. The rates of UTI, sepsis, DVT, and cardiovascular, pulmonary, renal, and neurologic complication were similar between the two groups. Also, no difference in early postoperative mortality, reoperation, and readmission rates between the two groups was observed.
RRC has gained popularity as the preferred choice of surgery in BC patients. However, few studies have focused on comparing the postoperative complications following RRC and ORC in obese patients. In none of the studies that compared RRC with ORC, the mean/median BMI of the studied population was ≥30 (i.e., obese). 12,14,15 A review of the available literature revealed important observations. Parekh and coworkers in a recent noninferiority trial (median BMI 28) demonstrated that RRC was noninferior to ORC in terms of 2-year progression survival rate and complication rates, along with significantly shorter LOS and lower blood transfusion rate, however, longer OPTIME. 12
Sathianathen and colleagues performed literature review and meta-analysis and demonstrated that RRC is associated with less risk of blood transfusion and marginally longer OPTIME, but no difference in major complications (Clavien III–V), postoperative 90-day quality-of-life assessment, or disease progression between RRC and ORC. 16
The literature is inconsistent regarding postoperative morbidity when comparing RRC and ORC. Khan and colleagues in their prospective single-center study comparing RRC, ORC, and laparoscopic RC in 60 patients (all groups had BMI <30) revealed higher complication and readmission rates for the ORC group, which concurs with our current study findings. 15 However a recent European multicenter study by Soria and coworkers (mean BMI was 26) revealed a higher readmission rate for RRC compared with ORC. 14 The authors of the former study believe that the shorter LOS after RRC may have contributed to the higher readmission rate. In a study utilizing the National Cancer Database (NCDB), where the patient BMI was not reported, the readmission rate between RRC and ORC was not different. 13 Our results demonstrated in the obese BC population, RRC is associated with lower readmission rate than ORC, which represents savings to the health care costs involved in the management of the obese BC undergoing RC.
Postoperative wound complications (infection/dehiscence) were fewer in RRC (6.3%) compared with ORC group (18.6%) (Table 2). Obesity is commonly associated with hypoalbuminemia and malnutrition, both of which can impair wound healing following ORC. 17 The cardiovascular, pulmonary, renal, and neurologic complication rates were similar between the two groups in this study. The lack of difference between the two groups in terms of complications related to specific organs post-RC may favor that obesity and its metabolic syndrome rather than the surgical approach (open/robotic) are the cause of such lack of difference. However, we observed that the proportion of patients who had more than one complication was significantly higher in the ORC group vs the RRC (p < 0.001).
Our results demonstrated the advantage of robotic surgery in reference to blood transfusion rate, which was lower in the RRC vs ORC group (10.9% vs 37.1%). A recent systematic review and meta-analysis comparing RRC with ORC demonstrated the advantages of RRC over ORC with less risk of blood transfusion. 15 Blood transfusion was reported to be associated with increased risk of perioperative infections following RC, which may be related to transfusion-related immunomodulation. 18
Also, contrary to some reports that showed RRC is a longer procedure than ORC, 13 our results showed the opposite in obese patients who underwent RRC. This may be related to the lack of ORC-associated long skin incision that may be time-consuming to close, difficulty in retracting wound edges together with bowel and intraperitoneal fat handling, which may interfere with surgical exposure during ORC, all of which may have contributed to the shorter OPTIME observed in the RRC group.
We acknowledge the limitations of our study. It is retrospective and nonrandomized, however, we used a PS to mitigate such limitation. It also bears mentioning that only self-selected institutions contribute to the data presented in the NSQIP database. Due to the nature of NSQIP database, some biases are inevitable. Only generic variables are available, and therefore, no other variables except those mentioned in this study could be assessed to limit confounding variables. We used BMI as an indicator and measure of obesity for patient selection, however, Psutka and colleagues have noted that visceral fat is another preoperative factor that can complicate surgery in the obese patient, which is not well represented via BMI measurements. 19 Also, NSQIP does not collect specific information on the approach (open/robotic) the urine diversion was performed. Consequently, while all the ORC group patients would have had their urine diversion done by the open technique, the RRC group patients may have had the urinary diversion performed intracorporeally or extracorporeally. However, the literature is not clear on the superiority of one approach on the other. There are recent reports showing no difference in complications between intracorporeal and extracorporeal urine diversion, while others are reporting favorable trends in complications associated with intracorporeal urine diversion. 20,21
Conclusions
We utilized the NSQIP database to compare the early postoperative morbidity and mortality rate between obese BC patients who underwent RRC, with a matched group who underwent ORC. Our results demonstrated lower perioperative morbidity, LOS, and OPTIME in the obese RRC group. No difference in the early postoperative mortality rate between the two groups was noticed. We demonstrate that obesity is not a limiting factor in offering robotic surgery for obese BC patients requiring RC and with better-reported outcomes in the NSQIP database. While the results of this study were drafted from a retrospective quality improvement national database, further clinical trials with precise definition of inclusion criteria and complications will be necessary to draw a firm conclusion regarding safety and efficacy of RRC in obese patients.
Footnotes
Author Disclosure Statement
The coauthor N.R.B. was a PhD candidate at the University of Arkansas for Medical Sciences when this study was conducted. He is currently employed by Eli Lilly and Company, Indianapolis, IN. No other authors report any conflict of interest.
Funding Information
No funding was received for this article.