
Abstract
Purpose:
There is increasing recognition of the advantages of holmium laser enucleation of the prostate (HoLEP) for benign prostatic hypertrophy (BPH) treatment in the United States but relatively little is known about the extent of HoLEP adoption over time. This study aims to assess national HoLEP adoption rates and regional trends from 2008 to 2014.
Methods:
We retrospectively analyzed a data set of 100% Medicare claims to determine the rate of U.S. HoLEP adoption in 2008, 2011, and 2014. Rates were adjusted by age and race and stratified by hospital referral region (HRR). Linear and logistic regression models were used to assess for trends in HoLEP adoption over time.
Results:
Total U.S. BPH cases decreased 24% from 2008 to 2014 and HoLEP cases increased significantly from 1086 (2008) to 3368 (2014). Despite this, HoLEP accounted for just 4% of total BPH cases in 2014. In 2008, 28/306 (9%) of HRRs recorded >10 HoLEP cases per year. This increased to 89 HRRs (29%) in 2011 but stabilized at 94 HRRs (31%) in 2014. In 2014, over 50% of states still had only 0 to 1 sites doing 10+ HoLEP cases per year.
Conclusions:
Based on this 100% sample of Medicare claims from 2008 to 2014, surgical BPH treatment volume has decreased, while HoLEP volume and regional adoption have tripled. However, rates of HoLEP remain extremely low at just 4% of all BPH procedures in 2014, and large regional gaps in care exist. These data indicate that HoLEP remains substantially underutilized and the majority of regions still lack access to centers performing >10 HoLEP cases per year.
Introduction
Benign prostatic hypertrophy (BPH) with lower urinary tract symptoms (LUTS) is a highly prevalent disease syndrome with significant potential morbidity and costs. It is estimated that >50% of men >50 years experience BPH/LUTS. 1 Untreated BPH may progress and eventually cause acute urinary retention, a medical emergency, chronic urinary retention, and/or renal failure. A 2005 study estimated that $3.9 billion dollars of health care costs were related to BPH/LUTS treatment in the United States. 2
Although transurethral resection of the prostate (TURP) remains the most common surgical treatment for BPH/LUTS, postoperative complications such as bleeding, incontinence, and sexual dysfunction have generated interest in a less-morbid option. Holmium laser enucleation of the prostate (HoLEP) emerged in the mid-1990s as a viable alternative to TURP. To date, at least six randomized controlled trials have shown that HoLEP has equivalent or significantly greater improvements in postoperative clinical outcomes with decreased complications. 3 In addition, multiple studies have shown that HoLEP has equivalent outcomes with significantly decreased morbidity compared with simple prostatectomy, 4 and the European Association of Urology (EAU) thus recommends HoLEP as first line treatment for glands >80 g. 5
However, despite the large body of evidence in favor of HoLEP vs TURP or simple prostatectomy, adoption in the United States remains low. Little is known about the rates of HoLEP use across the United States. A recent study of hospitals participating in the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) estimated that HoLEP accounted for just 5% of BPH procedures in 2015. 6 It is unknown whether HoLEP rates in the United States are increasing and the geographic distribution of HoLEP in the United States is also unquantified. Both have important implications for the future of HoLEP provider training as well as patient access to HoLEP in the United States.
The aim of this study is to expand on our understanding of HoLEP adoption in the United States using Medicare claims data. By using this data set, we will be able to more accurately assess HoLEP rates and determine the geographic distribution of HoLEP providers over time. This will enable us to assess the progress of HoLEP adoption in the United States and determine where gaps in HoLEP access and training exist.
Methods
A 100% sample of Medicare claims from the Centers for Medicare and Medicaid Services (CMS) was utilized to identify male beneficiaries undergoing HoLEP or any other BPH treatment procedure during the years of 2008, 2011, and 2014. It is estimated that 98% of adults >65 years are enrolled in Medicare. Before 2007, the current procedural terminology (CPT) code for “laser enucleation of the prostate with morcellation” (52649) did not exist and thus HoLEP rates cannot be accurately determined before this year.
Other BPH procedures included were TURP, laser vaporization of the prostate, transurethral microwave therapy, transurethral needle ablation, and simple prostatectomy. We identified these procedures using the following CPT codes that were in use from 2008 to 2014: 52601, 52612, 52614, 52620, 52630, 52647, 52648, 62649, 53850, 53852, 55821, and 55831. Bipolar enucleation of the prostate lacks its own code and should be captured within the other procedure codes.
For each year of analysis, we identified the hospital referral regions (HRRs) with >10 HoLEP cases performed and used these data to create geographic maps of HoLEP rates over time. HRRs are defined by the Dartmouth Atlas of Healthcare and consist of 306 regions that represent aggregated hospital service areas where patients receive the majority of their hospital-based care. 7
HoLEP rates were defined as the number of HoLEP procedures performed divided by the overall number of BPH procedures performed, determined by CPT code. Rates were stratified by HRR and year and adjusted by age and race. Linear regression models were used to assess for trends in the number and rate of HoLEP procedures performed over time. Logistic regression models were used to assess for uptake of HoLEP by both HRR (306 regions) and American Urological Association (AUA) section region. Statistical analysis was performed using STATA v.14 (StataCorp, 2015) and geographic maps were created using Tableau Software v.10.5. Institutional Review Committee approval was not required as data were already deidentified and aggregated by CMS.
Results
From 2008 to 2014, the total number of BPH cases in the U.S. Medicare population decreased 24% from 109,809 to 83,956. In 2008, HoLEP accounted for just 1% of total BPH procedures (1086 cases). This increased 180% by 2011 (3062 cases), but HoLEP still accounted for a small fraction (3.3%) of BPH procedures. From 2011 to 2014, HoLEP cases rose with a modest growth rate of 10%. However, the proportion of HoLEP compared with other BPH procedures remained low at just 4% in 2014 (Fig. 1).

Proportion of HoLEP vs total BPH cases in the United States (2011–2014). Light gray bars: represent the total number of BPH cases done in the United States from 2011 to 2014. Dark gray bars: represent the number of HoLEP cases in that time period. BPH = benign prostatic hypertrophy; HoLEP = holmium laser enucleation of the prostate.
In 2008, <10% (28/306) of HRRs performed at least 10 HoLEP procedures that year (Table 1 and Fig. 2a). This increased significantly in 2011 to 29% (89/306) of HRRs (p < 0.01, Fig. 2b). In 2014, an additional 28 HRRs started doing 10+ HoLEP cases compared with 2011; however, 23 HRRs either stopped doing HoLEP or decreased to <10 cases. This resulted in a nonsignificant net increase of just five HRRs (94/306) performing 10+ HoLEP cases per year from 2011 to 2014 (p = 0.4, Fig. 2c).

Regional Analysis of Sites Performing 10+ HoLEP Cases Per Year
Adjusted for age and race.
Boldface values indicate statistical significance.
HRRs = hospital referral regions.
There were substantial improvements over time in the proportion of HRRs performing 10+ HoLEP cases per year within each AUA section region. By 2014, every AUA section had at least one HRR performing 10+ HoLEP cases per year (Table 1). However, significant variation remains—only 15% of HRRs in the Mid-Atlantic section billed 10+ HoLEP cases compared with 44% of HRRs in the Western section (p = 0.02). Average HoLEP rates (compared with total BPH procedures) by region ranged from 1.5% to 4.3%, but this was not statistically significant. Although average HoLEP rates overall remained low by region, in individual HRRs performing 10+ HoLEP cases in 2014, HoLEP cases represented up to 49% of BPH cases at that site.
Although the number of HRRs with 10+ HoLEP cases increased significantly from 2008 to 2014, 69% of HRRs in 2014 recorded very low volume or no HoLEP cases. Large geographic gaps in access to HoLEP centers remain and do not appear to be improved over time (Fig. 3). The number of states without any HRRs performing 10+ HoLEP cases increased from 15 in 2011 to 16 in 2014, and the number of states with only a single HRR was the same (12) in both years. In 2014, only 15% of HoLEP cases nationally were performed at very low-volume (<10 HoLEP cases per year) sites, indicating that the majority of the 212 HRRs in our data set recording <10 HoLEP cases are performing no HoLEP.
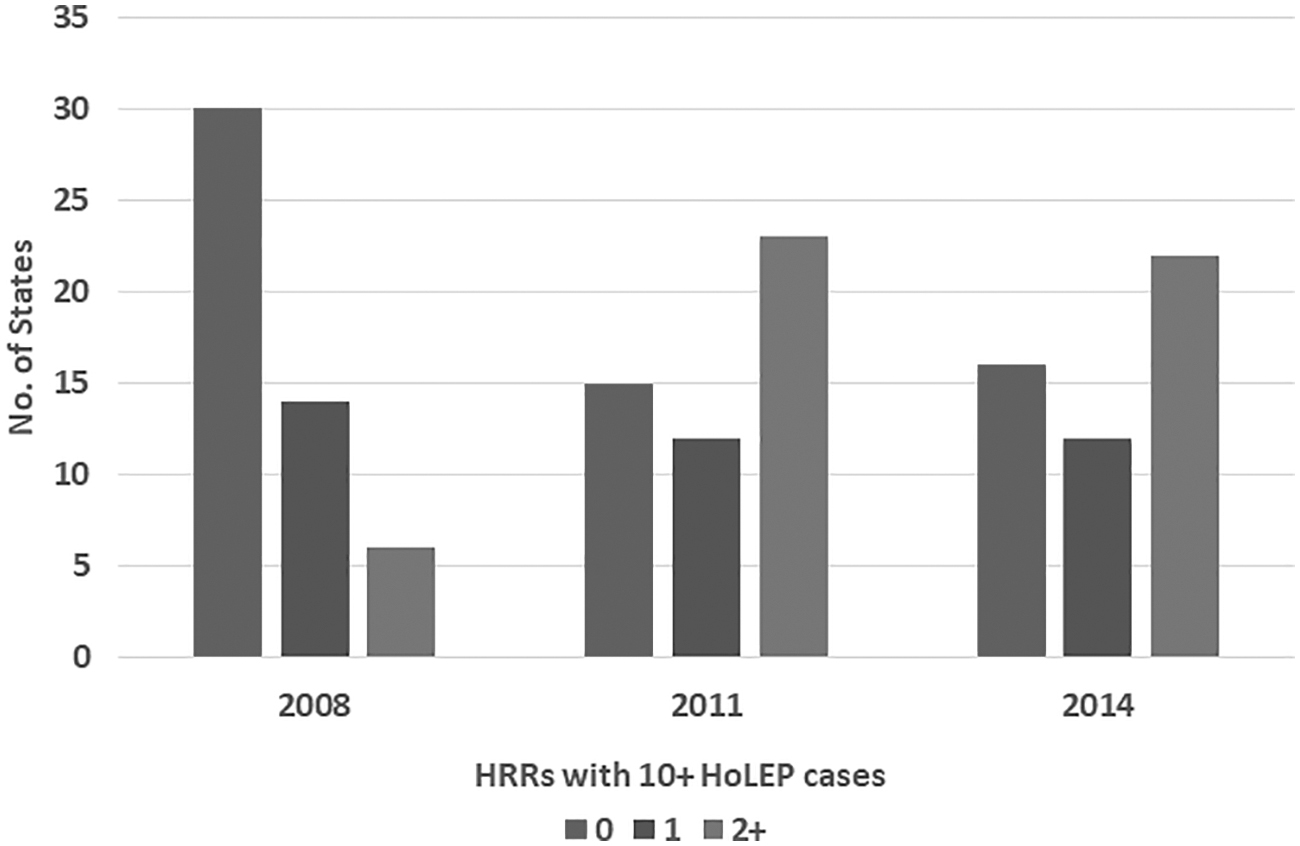
No. of states with limited access to HRRs performing 10± HoLEP cases per year. Each bar represents the number of states with zero locations performing >10 HoLEP cases that year (first bar), 1 location performing >10 HoLEP cases (second bar), or 2+ locations performing >10 HoLEP cases (third bar).
Discussion
HoLEP is arguably the “gold standard” of BPH treatment. 8 There are at least six randomized controlled trials with long-term data showing equivalent or significantly greater improvements compared with TURP in postoperative AUA symptom scores, peak urine flow rates, postvoid residuals, and sexual function with significantly decreased complications such as need for transfusion, catheterization time, and hospital stay. 3,9 Multiple studies have found equivalent outcomes with decreased morbidity compared with both open and robotic simple prostatectomy. 4,10,11
Despite the extensive evidence supporting HoLEP, we found that HoLEP accounted for just 4% of total BPH procedures performed in 2014 in the U.S. Medicare population. This low percentage is especially notable given that HoLEP is recognized by both the AUA and EAU guidelines as the only BPH treatment modality that is recommended for prostates of any size. The number of HoLEP cases performed in the United States nearly tripled from 2008 to 2011, but there was only a small and nonsignificant increase in HoLEP use from 2011 to 2014, indicating a plateauing of provider interest in the procedure.
Reasons for the low adoption of HoLEP in the United States are multifactorial. Although studies have found that there is no difference in difficulty between learning HoLEP vs other enucleation procedures, 12 it is thought that the learning curve is in the range of 20 to 40 cases, 13 which may be difficult for providers to achieve without close mentorship. Our study revealed that significant geographic gaps in HoLEP adoption exist with >50% of states having 0 to 1 HRRs performing 10+ HoLEP cases per year. Given this, it is a reasonable assumption that most urologists and trainees lack access to an experienced HoLEP provider to learn the procedure and receive sufficient mentorship.
Lack of access to HoLEP training has not been identified as a significant issue in the United States in part because, unlike the EAU guidelines, HoLEP is not recommended as a first-line therapy for BPH in the AUA guidelines. In the EAU guidelines, HoLEP is given a level 1a recommendation for BPH treatment of any gland size and is recommended as the treatment of choice for large glands >80 g. In contrast, the AUA guidelines advise providers to “consider” HoLEP with a Grade B evidence level. For the purposes of this discussion, it does not matter which guideline is more “correct,” only that providers are likely more motivated to learn a technique, despite potential difficulty, if it receives a strong recommendation in official guidelines.
Cost has been identified as another significant barrier to HoLEP adoption. Direct equipment costs include the cost of a high wattage (>80 W) laser and an endoscopic morcellator. Although some institutions are beginning to question the need for a high wattage laser, 14 there are also indirect labor costs such as increased operating room time compared with other endourologic modalities. 15 However, costs alone are unlikely to be the sole driver of low HoLEP adoption in the United States. There are other procedures with high costs of initialization (e.g. robotic surgery) that have become widely utilized despite the costs, largely because there are other positive incentives driving provider adoption.
Although HoLEP is arguably the best clinical choice for many BPH patients, there is no real economic incentive in its favor. This can have substantial impact on adoption—most of the U.S. health care system remains on a fee-for-service reimbursement model and multiple studies have shown that financial incentives within this model may influence provider behavior. 16 Unlike competing technologies such as Greenlight™ photovaporization or Urolift™, there is no company that is marketing HoLEP to providers or consumers. Medicare reimbursement is nearly identical between HoLEP (24 relative value units [RVUs]) and TURP (21 RVUs), and there are no disincentives for multiple lifetime BPH procedures in a fee-for-service model.
There are two additional potential reasons why the adoption of HoLEP significantly slowed down after 2011. Multiple other endourologic BPH treatment modalities such as laser photovaporization and prostatic urethral lift became popular during this period. We also found that the number of total BPH procedures decreased 24% from 2008 to 2014. We believe we are the first to report this national trend. This is likely due to the rise of medical management for BPH, which began with the publication of the Medical Therapy of Prostatic Symptoms (MTOPS) trial in 2003 and inclusion in the AUA guidelines for the treatment of BPH in 2006. Filson et al. found that the use of medical management increased from 14% of visits in 1993–1995 to 40% in 2008–2010. 17
A strength of this study was our ability to identify the practice locations (HRRs) of providers who perform 10+ HoLEP cases per year over time. We found that there is significant geographic variation—in 2014, >33% of the New England, Southeastern, and Western section HRRs performed 10+ HoLEP cases vs <15% in the Mid-Atlantic section. From 2011 to 2014, the majority of new HRRs performing 10+ HoLEP cases were in states that already had 2+ HRRs performing high-volume HoLEP cases. Geographic clustering of HoLEP providers may be a result of training and/or mentorship proximity or may reflect development of regional patient demand.
Large geographic areas remain that lack access to a provider who does 10+ HoLEP cases per year. The number of states with zero high volume HoLEP providers increased from 2011 to 2014 and >50% of states in 2014 had <2 HRRs performing 10+ HoLEP cases per year. This represents a significant issue for patients, who often must travel out of state to find a HoLEP provider. Similarly, urologists in those states would have to travel significant distances to become trained in HoLEP and would have no opportunities for personal mentorship. Figure 2 shows the high-priority areas for HoLEP provider training and recruitment.
Although studies have analyzed trends over time of other BPH procedures such as simple prostatectomy or laser photovaporization of the prostate, 18 there is a paucity of data on HoLEP. Anderson and colleagues reported on trends in major BPH procedures, including HoLEP, using NSQIP data from 2011 to 2015. 6 Compared with our study, they found a similar low rate of HoLEP use—their finding of a HoLEP rate of 5% (vs 4% in our study) may be an overestimation because larger practice sites, which are more likely to do HoLEP, are disproportionately represented within NSQIP. A strength of our study is that it captures 100% of Medicare claims, from all sites nationally, whereas <10% of hospitals participated in NSQIP from 2011 to 2015. 19
This article has several limitations. Medicare claims captures the vast majority of U.S. men >65 years but does not capture everyone, and notably, it includes no one <65 years. We believe men younger than 65 years represent a small proportion of men undergoing HoLEP and in the NSQIP study by Anderson et al., the lowest mean age in the HoLEP group was 68.7 years. 6 Furthermore, it is unlikely that there are HoLEP providers only seeing younger men who would be missed on our geographic analysis.
Our data set represents national Medicare claims aggregated by HRR. Although it has been adjusted for age and race, we lack further granular detail about HoLEP providers, patients, or rates of other BPH treatment modalities. As such, we are unable to identify HRRs that are performing no HoLEP (0 cases) vs those that are low volume (<10 cases per year). Although this would add further specificity to our data, we do not believe it would change our results, as sites that are performing very low volume HoLEP do not substantially improve access to HoLEP for patients or trainees.
Lastly, our data set is limited to 2008 to 2014 and it is possible that HoLEP utilization has subsequently increased significantly. However, our data show that HoLEP use and adoption were relatively stable from 2011 to 2014, so we would not expect this to acutely change. With the continued increase in BPH medical management and new treatment modalities, we would expect HoLEP rates to either be stable or decrease over time, not increase. Lastly, the NSQIP data set confirms the stability of HoLEP rates since 2011. 6
Conclusions
Although there are multiple randomized controlled trials supporting the use of HoLEP over other BPH treatment modalities such as TURP or simple prostatectomy, based on a 100% Medicare claims data set, rates of HoLEP use in the United States remain very low. Adoption of HoLEP substantially slowed after 2011 and significant geographic variation remains among practices that perform at least 10+ HoLEP cases per year. Lack of access to a HoLEP provider represents a serious issue for both patients and other providers or trainees. These data may be used to determine how best to allocate future resources for HoLEP provider training and/or recruitment.
Footnotes
Acknowledgments
This material is based on work supported by the Office of Academic Affiliations, Department of Veterans Affairs, VA National Quality Scholars Program and with resources and the use of facilities at VA Tennessee Valley Healthcare System, Nashville, TN.
Author Disclosure Statement
J.R. and V.P. have no conflicts to disclose; N.M. is consultant for Boston Scientific, Thermedx, and Intuitive Surgical.
Funding Information
The data employed in this analysis were obtained from The Dartmouth Atlas, which is funded by the Robert Wood Johnson Foundation and The Dartmouth Clinical and Translational Science Institute, under award no. UL1TR001086 from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH).