
Abstract
Purpose:
The aim of this survey was to obtain an overview of current European standards in the endoscopic visualization and management of bladder tumors.
Methods:
An online survey was launched in July 2018 for a duration of 4 months. It was distributed to all members of the European Association of Urology (EAU) and included 23 questions divided into 3 thematic sections: general information, white light cystoscopy (WLC) and imaging, and transurethral resection of bladder tumor (TURBT) techniques.
Results:
Responses of 222 participants were included for analysis. The majority of physicians were between 30 and 40 years of age (48.2%, n = 107) and performed over 50 TURBT per year (52.2%, n = 115). Overall, 52.3% (n = 116) reported WLC findings in written form only, 23.8% (n = 53) added endoscopic footage, and 79.2% (n = 176) considered preliminary WLC/TURBT reports before performing a subsequent bladder intervention. About half of the participants (50.5%, n = 104) used additional tumor visualization methods (aTVMs), but aTVMs were utilized by a greater proportion of physicians from Western countries (58.1%, n = 90) compared with developing countries (20.0%, n = 7). Photodynamic diagnosis was the predominant aTVM technique employed (43.8%, n = 60). Bipolar current was the most common technique for TURBT (46.6%, n = 149). Most urologists in this study occasionally utilized techniques like resections in fractions (80%, n = 161) or en bloc resection (87.2%, n = 182). A repeated TURBT was performed when no muscle was found in the specimen (70.6%, n = 149) and/or if the tumor was stage pT1 (72.0%, n = 152) or high grade (63.0%, n = 133).
Conclusion:
Implementation of resection techniques or repeated TURBT within EAU guidelines is promising, but it can be further challenged. For example, WLC/TURBT reporting should be improved since urologists consistently consider previous documentation. Given the moderate application rate of aTVMs, an attempt to increase its utilization would lead to a better assessment of its potential benefit.
Introduction
Bladder cancer (BC) is the second most frequent urological malignancy and the sixth most common cancer in the European Union. 1 About 75% of newly diagnosed BCs are of the nonmuscle invasive bladder cancer (NMIBC) subtype. 1 Due to high recurrence and progression rates, patients with NMIBC require frequent endoscopic follow-up and reintervention. Expenses for the management of BC have reached about €4.9 billion per year (5% of all cancer coasts) in the European Union, making BC one of the most expensive cancers to treat. 2 Consequently, there is great interest in optimizing NMIBC management.
Generally white light cystoscopy (WLC) followed by transurethral resection of bladder tumors (TURBT) is the gold standard for diagnosis, staging, and therapy of NMIBC. The use of modern imaging techniques such as photodynamic diagnosis (PDD) or narrow band imaging (NBI) increases tumor detection and may prolong recurrence-free survival (RFS). 3,4 The application of distinct TURBT resection techniques like en bloc resection (EBR) or resection in fractions (RiF) might help to improve surgical outcomes and pathological staging. 5,6 A comprehensive documentation of cystoscopy (CY) and TURBT findings is important for the communication between physicians and for patient counseling. 7,8
Generally, the management of NMIBC should follow international or national guideline recommendations, which provide an excellent compendium of evidence-based instructions in diagnosis and disease management. On the other hand, NMIBC management might be influenced by economic factors, availability of appropriate technology, technical equipment, and staff qualifications and thus may differ from guideline recommendations. Previous studies have suggested widespread underuse of guideline recommendations. 9 Therefore, we conducted a survey to assess current European practices in management of NMIBC to identify weak points in European guideline implementation and to uncover potential options for improvement.
Materials and Methods
Survey design
An online questionnaire was developed and distributed using cloud-based survey software (SurveyMonkey® Europe, Dublin, Ireland). The survey consisted of 23 questions that were divided into 3 categories: general information (n = 8), CY and imaging (n = 5), and TURBT techniques (n = 10). Questions were either close ended or multiple choice and could be skipped or revised after a first reply when desired. All questions were formulated to encourage the best possible estimate, with the assumption that exact data would be laborious to generate. The questionnaire was checked for content validity by 10 urologists of different educational status in an Academic Medical Center (AMC). The survey was open for urologists of all ages, origins, educational status, workplace, or experience level. Participants were excluded from the study if they completed <50% of the survey, had incomplete general information data, or supplied contradictory answers.
Survey distribution
The survey was distributed through the European Association of Urology (EAU) and EAU Section of Uro-Technology e-mail distribution lists as well as the European Society of Residents in Urology Google Groups® account (Google LLC, Mountain View, CA), potentially reaching 15,000 EAU members (10,500 board-certified urologists, 4500 residents). It was additionally posted on the EAU twitter feed. Participation was voluntary and not rewarded. Personal information was not collected and data were anonymous. The survey was launched at the end of July 2018, and recruitment of participants continued until November 2018.
Subgroups
Cohort answers were first integrally analyzed and subsequently separated into the following subgroups: Country of origin: Western countries (W; e.g., England and Germany), Eastern countries (E; e.g., Poland and Ukraine), and developing nations (R; e.g., Brazil and Turkey). Age: under (<) or over (≥) 30 years of age. Number of TURBT procedures: under (<) or over (≥) 50 per year. Institution: academic vs nonacademic. Hospital operator: private vs nonprivate. Qualification: resident vs board-certified urologist.
Statistical analyses
Statistical analyses were performed with JMP® software (version 14.0.0; SAS Institute, Cary, NC). Values are expressed as percentage for qualitative variables and as median for continuous variables. The chi-squared test and Fisher's exact test were used to compare categorical variables. Variations were judged as significant at p values <0.05.
Results
General cohort information and response rate
The information on the cohort surveyed is presented in Table 1.
General Cohort Information
AMC = Academic Medical Center; prc = procedures; TURBT = transurethral resection of bladder tumors.
CY techniques
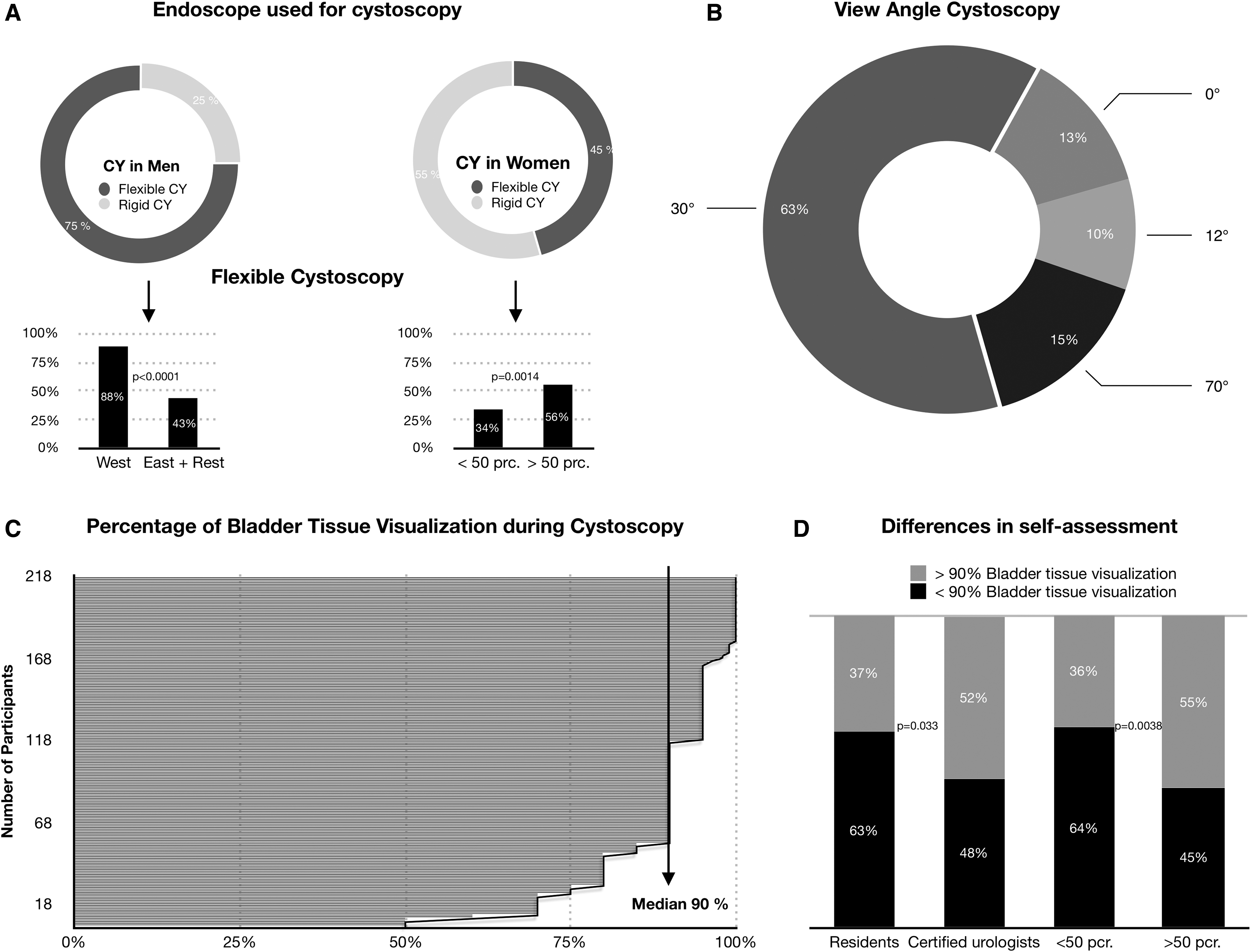
In Western countries, urologists used flexible instruments in men significantly more often than in the remaining two geographic areas (W 88.4%, n = 137; E 40.6%, n = 13; R 45.7%, n = 16; p < 0.0001). Just over half of urologists (54.5%, n = 121) routinely use a rigid cystoscope in women (Fig. 1A). The main view angle used for rigid WLC was 30° (Fig. 1B). Participants were asked to estimate a subjective percentage of the bladder surface that was visualized when performing a routine WLC. The median estimate of the bladder surface examined was 90% (range 50%–100%) (Fig. 1C). A detailed self-assessment evaluation of the visualization shows that residents and urologists who perform <50 TURBT procedures per year provided significantly lower estimates of the area of bladder surface visualized (Fig. 1D).
Documentation and transfer of CY and TURBT reports
Overall, 52.3% (n = 116) of the participants used a written report alone for documentation of WLC findings (Fig. 2A). There were no significant differences between subgroups. Of all participants, 23.8% (n = 53) added additional endoscopic images and 8.6% (n = 19) stored additional video footage for documentation of WLC.

The transfer of endoscopic findings to other attending physicians (Fig. 2B) was done by mail by almost half of the physicians (45.5%, n = 101). Urologists over 30 years of age prefer this modality significantly more than the younger group (50.0%, n = 79 vs 25.4%, n = 16; p = 0.002). On the other hand, residents tended to use secured electronic data transfer (i.e., by a picture archiving and communication system server) significantly more often (54.9%, n = 50 vs 29.7%, n = 39; p = 0.0002).
Around 79.2% (n = 176) of participants considered previous WLC/TURBT reports in >60% of cases, and 54.1% (n = 120) did so in every case (Fig. 2C). Board-certified urologists considered preliminary reports significantly more often than residents (p = 0.011). The majority of patients received oral information about the diagnostic findings (Fig. 2D).
Endoscopic imaging techniques and diagnosis of the upper urinary tract
Overall, 50% (n = 104) of urological surgeons used additional tumor visualization methods (aTVMs) during TURBT (Fig. 3A). aTVMs were used significantly less by participants from developing countries in comparison to physicians from Western countries (R 20.0% vs W 58.1%; p < 0.0001). Physicians employed in public hospitals used aTVMs significantly less often in comparison to private hospital employees (51%, n = 105 vs 29%, n = 6, respectively; p = 0.049).
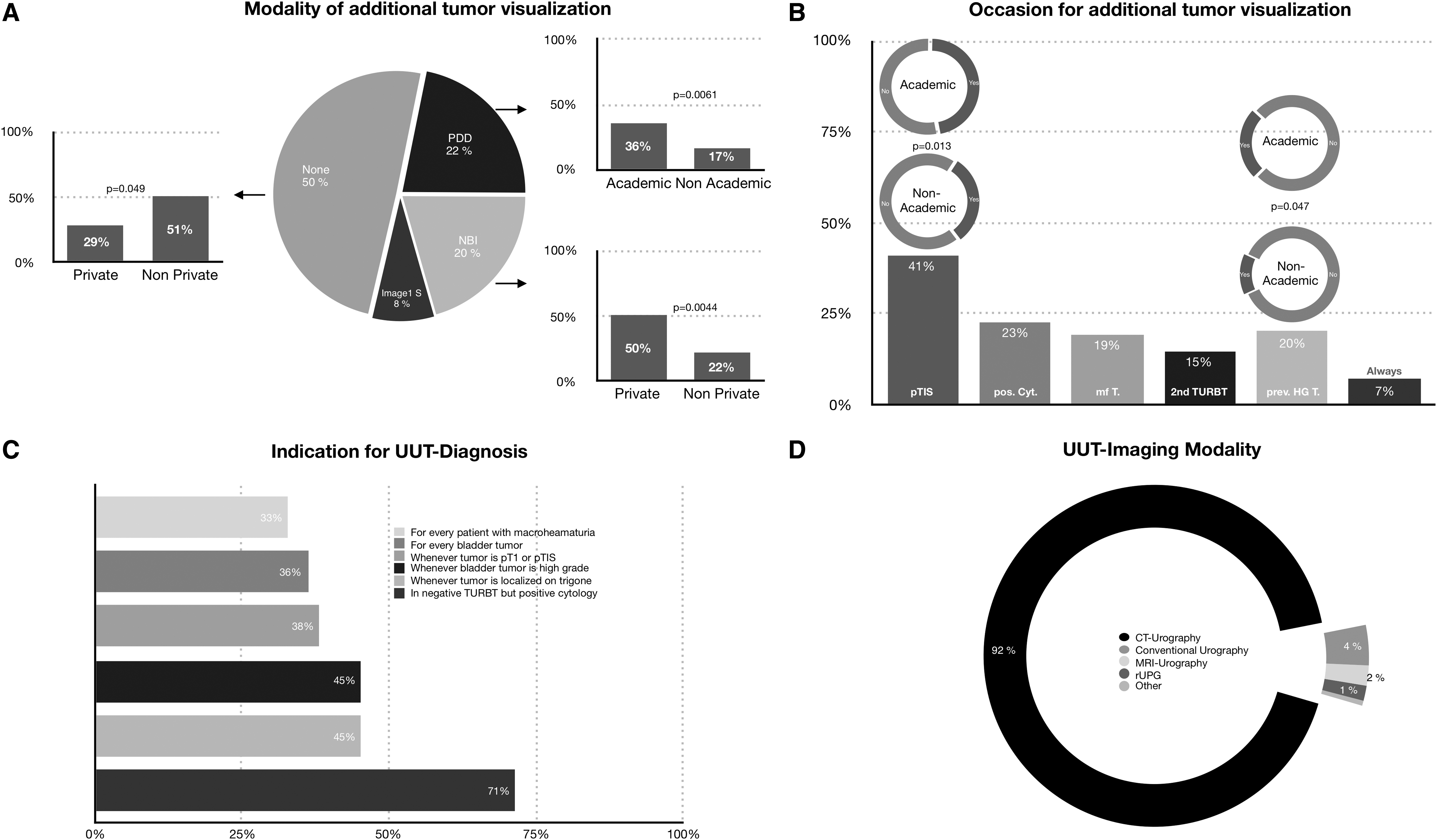
PDD is the predominant additional technique, employed by 43.8% (n = 60) of responders who use aTVMs. Urologists in AMC used PDD significantly more often than in nonacademic centers (35.8%, n = 43 vs 16.6%, n = 17, respectively; p = 0.006). PDD was used significantly more often by participants from Western countries than elsewhere (W 34.8%, n = 54 vs E 15.6%, n = 5; and vs R 2.9%, n = 1; p < 0.0001). NBI was utilized by 40.1% (n = 55) of aTVM users and Storz Professional Image Enhancement System (SPIES) by 16.1% (n = 22).
The predominant reason for using an aTVM was a suspected pTIS lesion (41.0%, n = 87) (Fig. 3B). aTVMs were significantly more often used by AMC-employed, board-certified urologists over 30 years of age (p = 0.006–0.01). Overall, 71.4% (n = 150) of the participants recommended upper urinary tract (UUT) diagnosis for patients with negative TURBT but positive cytology, and 36.2% (n = 76) recommended UUT diagnosis for every diagnosed BC (Fig. 3C). CT-urography was by far the most frequently used modality (91.8%, n = 194) for UUT diagnosis, regardless of region or workplace (Fig. 3D).
Techniques of TURBT
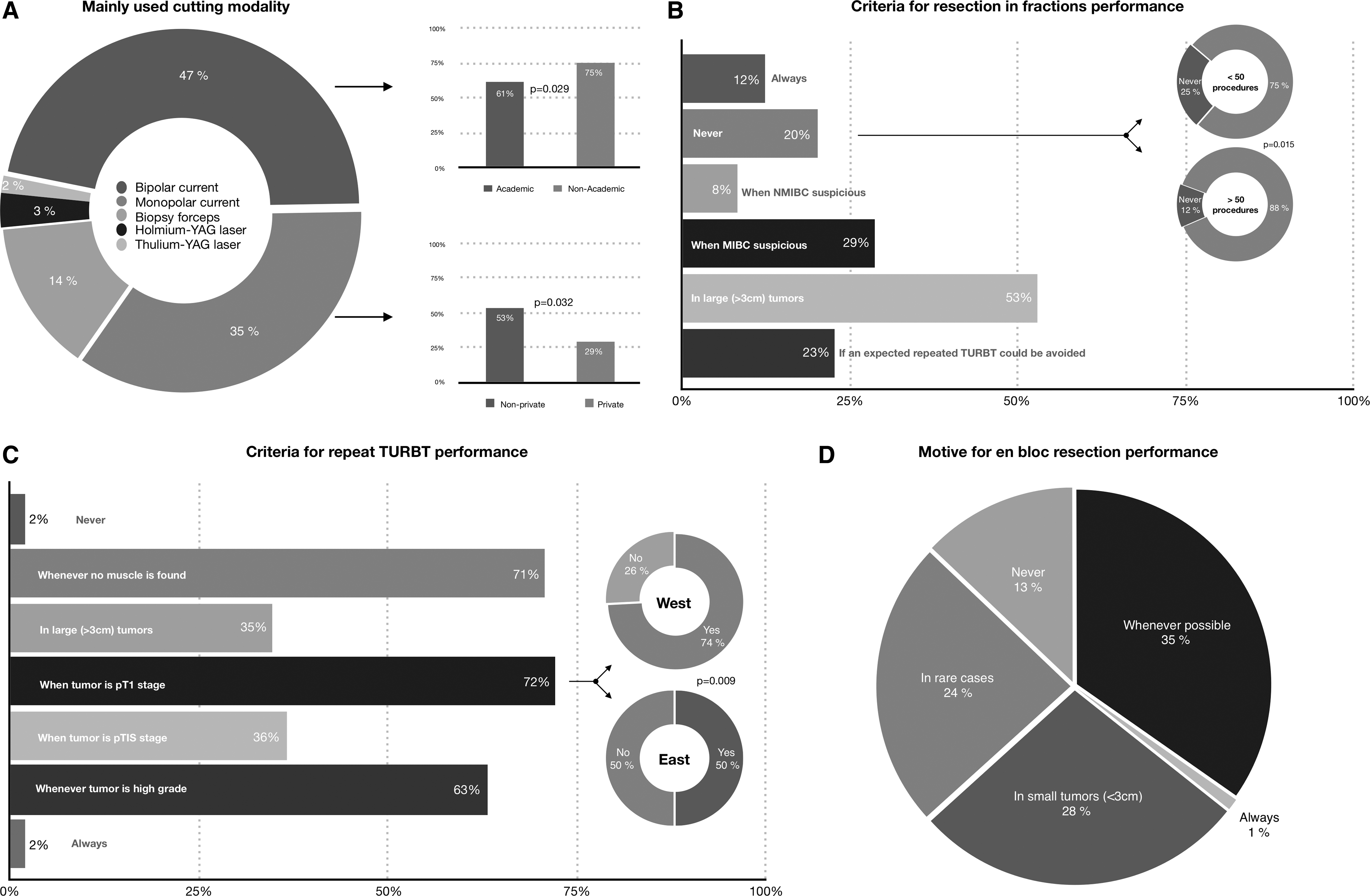
TURBT was performed using bipolar current by 46.6% (n = 149) of study participants (Fig. 4A). Monopolar current was used by 35.0% (n = 112) of participants and was more common in nonprivate hospitals (52.7%, n = 106 vs 28.6%, n = 6; p = 0.032).
(
Participants primarily applied tumor resection and sampling in fractions (tumor, tumor ground, tumor boundaries) for large tumors (>3 cm; 52.9%, n = 116) or if muscle-invasive BC was suspected (28.8%, n = 63) (Fig. 4B). When compared with residents, board-certified urologists would perform RiF more often to avoid a repeated TURBT (27.5%, n = 36 vs 15.4%, n = 14; p = 0.031). Overall, 20% (n = 42) of participants never performed RiF, and this rate was lower for more experienced physicians (12.2%, n = 14). Predominant reasons to perform a repeated TURBT were pT1 stage (72.0%, n = 152), the absence of muscle in the specimen (70.6%, n = 149), or a high-grade (HG) tumor (63.0%, n = 133) (Fig. 4C). Compared with Western countries, significantly fewer participants of Eastern countries chose a pT1 tumor as a reason for repeated TURBT (74.1%, n = 115 vs 50.0%, n = 16; p = 0.0087). Altogether, 34.8% (n = 73) of participants indicated that they would perform an EBR whenever it was technically possible (Fig. 4D). A quarter of the physicians (23.8%, n = 50) applied this technique rarely and only 12.8% (n = 27) not at all. No significant differences were found within the subgroups.
The most widely used drug for immediate intravesical instillation of chemotherapy was Mitomycin-C (70.4%, n = 145) followed by epirubicin (13.6%, n = 28). Immediate instillation was most frequently performed after resection of small tumors (<3 cm) (50.2%, n = 107) or when NMIBC was suspected (43.2%, n = 92).
Discussion
Due to high recurrence and progression rates, NMIBC is a major threat to the individual patient and an enormous socioeconomic burden to society. 2,10 Therefore, urologists should seek to optimize NMIBC management according to evidence-based guidelines. 11 Little is known about the actual deployment and diffusion of EAU guidelines. Therefore, we conducted a comprehensive survey to obtain a current view of European standards in NMIBC management.
Generally, NMIBC management involves repeated endoscopic treatments and follow-up cystoscopies. In this study, the knowledge of the patient's history and previous findings is essential, and this has been emphasized by the results of this survey. Our data show that nearly 4 out of 5 urological surgeons actively examine previous reports before a subsequent bladder intervention. Remarkably, the majority of urologists in this study relied on written reports only when documenting their diagnostic findings. Less than a quarter of physicians reported adding additional endoscopic images to their reports, despite the advanced technical assistance currently available. While other disciplines such as radiology or gastroenterology routinely complete their medical reports with the corresponding images, 12 the surveyed population of urologists seems to be lagging behind. Perhaps a universal text template for reporting on WLC/TURBT would contribute significantly to improving the quality of documentation. 13 An optimized documentation protocol might have therapeutic impacts. A recent gastroenterological study showed that 1 in 4 endoscopic mucosal resections had to be abandoned because of inadequate reporting and management by the referring endoscopist. 14 Image-based documentation could potentially support second opinion reviews by subspecialists, which has been shown to result in a significant number of interpretation changes and a reduction of interventions in other disciplines. 15,16
In addition to improved documentation, future technical assistance such as panoramic CY or three-dimensional reconstruction of the bladder 17,18 could support the physician in terms of a complete bladder examination. Interestingly, our data suggest that only 1 in 5 urologists assumes that they visualize the whole bladder surface in an ordinary WLC, and the majority of physicians estimate they miss at least 10% of the bladder surface. Although assumed completeness of the WLC seems to improve with experience, technical assistance in terms of an automated bladder scan could certainly improve detection of pathological findings.
An optimized tumor visualization is crucial to identify and resect all cancerous lesions. The gold standard for WLC and TURBT is white light imaging, which offers an excellent detection rate for papillary lesions. 19 However, its sensitivity for flat lesions is limited. PDD is probably the best examined and established aTVM. Numerous studies have shown an increased tumor detection rate and decreased tumor residual rate for PDD. 3,20 Other common aTVMs are NBI or SPIES. The EAU guideline recommends the use of aTVMs when they are available. Half of the survey participants regularly use aTVMs. Generally, aTVMs are utilized more in AMC compared with the private sector. This might partly be explained by the scientific interest of WLC improvement, but also by the unequal reimbursement for aTVMs. Additional costs could also explain the differences in aTVM employment for Western vs newly industrialized countries. Although studies were able to show long-term cost reductions for aTVM use compared with WLC, 21 there is still an ongoing debate on the general benefit of aTVMs, 22 which mirrors the inconsistent use of aTVMs in the study cohort.
The most frequently applied resection modality in TURBT is bipolar current (47%), followed by monopolar current (35%). Controversial studies suggest that bipolar current facilitates pathological staging but seems to have no impact on hemostasis or resection time. 23 Moreover, recently no differences between recurrence rate or perioperative complications could be found between mono- and bipolar current. 24
The EAU NMIBC guidelines strongly recommend specific TURBT resection techniques to remove tumors completely and ameliorate pathological staging. 22 One approach is the so called EBR, in which tumors are extracted in one piece by excising the exophytic portion from the mucosa without cutting the tumor itself. Recent findings show that EBR increases detrusor presence in specimen and that laser EBR reduces the rate of obturator nerve-related bladder perforation. 25 Recently, the use of a polypectomy snare to perform EBR was shown to be more time efficient than electric current. 26 Of survey participants, 35% attempted to perform EBR whenever possible, and another 28% did so for small tumors. Only 13% would never resect en bloc. A different technical TURBT approach is the fractioned resection of the exophytic part of BC, the underlying bladder wall, and the tumor margins (RiF). This gradual resection delivers good information of tumor extension as well as high-quality specimens. 5 Overall, 53% of the surveyed population resected in fractions when tumors were >3 cm. Our data suggest that the decision to use RiF depends on practical experience level, since surgeons performing <50 TURBTs a year are less likely to apply RiF. In this study, improvements in training and guideline diffusion could meaningfully improve NMIBC management.
Along with improvements in initial tumor visualization and resection techniques come specific indications for early repeated TURBT. EAU guidelines suggest a repeated TURBT for patients where no muscle was found in specimen (except for pTa, low grade [LG], and primary carcinoma in situ [CIS]), as well as in cases where the tumor is stage pT1. 22 Other guidelines, such as from the American Urological Association, also recommend a repeated TURBT for HG tumors. Previous studies have demonstrated that the aforementioned constellations are risk factors for disease persistence or tumor understaging, and that a second TURBT can increase RFS. 11,27,28 Repeated TURBTs are suggested by survey participants in 71% (no muscle found), 72% (pT1 tumor), and 63% (HG tumor) of BC cases. These results are encouraging, but leave considerable room for improvement. Previous studies have shown higher rates of repeated TURBT in high-risk NMIBC patients (76%–98%) in accordance with guidelines. 9
The present study attempts to present current TURBT practices across Europe. However, there are limitations, including the low response rate of around 2% and the corresponding small cohort size. Therefore, despite its wide distribution, the survey cannot claim to be representative of the whole of Europe. However, previous studies are in agreement with our derived results. 9 Additionally, since urologists were not incentized and agreed to participate voluntarily, there may be a selection bias toward including participants with a pre-existing interest in NMIBC management. There might be an additional selection bias for younger urologists who are more interested in surveys and are easier to reach by electronic distribution. Moreover, there were no controls to determine whether responses were correct or embellished, and participants were not specifically asked about their technical equipment. Finally, due to the lack of reliable data, no statement can be made as to whether the participants were acting on their own or in accordance with institutional guidelines.
Conclusion
In conclusion, we demonstrated that different TURBT resection techniques or the use of a second TURBT are typically applied in accordance with EAU guideline suggestions on NMIBC management. Modern imaging technologies were employed by only half of the participants in this study, possibly due to questionable oncological benefit and financial barriers. Endoscopic documentation of CY findings was considered important by the majority of urological surgeons. Standardization of endoscopic documentation and transfer of endoscopic video footage offer opportunities for improvement.
Footnotes
Acknowledgments
The authors would like to acknowledge the European Association of Urology as well as the EAU Section of Uro-Technology and the EAU Section of Urological Imaging (ESUI) as supporters of this project. The authors owe profound gratitude for their assistance and survey distribution to their members.
Author Contributions
F.W.: data collection, figure editing, and article drafting; S.H., B.G., and R.S.-I.: article editing; E.L. and G.S.: survey distribution; A.R. and C.G.: project supervision; M.C.K.: statistical guidance, figure, and article editing; A.M. and M.R.: project development and supervision.
Author Disclosure Statement
The authors declare that no competing financial interests exist.
Ethics Standards
No patients were included in this study. Participation was voluntary and anonymous.
Funding Information
The work was supported by the German Federal Ministry of Education and Research (BMBF). Project 13GW0203A: “Digitale Plattform mit 4PI-Echtzeit-Endoimaging zur endoskopischen 3D-Rekonstruktion, Visualisierung und Nachsorgeunterstützung in der Gesundheitsversorgung von Patienten mit Harnblasenkarzinom.”