
Abstract
Objective:
To determine possible risk factors for accidental nephrostomy tube dislodgement and compare two different tube types in this context in patients with chronic catheters.
Materials and Methods:
We conducted a retrospective study of long-term patients with nephrostomy tube. We performed a comparative analysis, studying the possible variables that were related to catheter dislodgement. In addition, a subanalysis was also carried out comparing different catheter designs (Pigtail and Foley) in case this could be related to the dislodgement.
Results:
Two hundred five cases were collected. A total of 51.2% of cases had a pigtail nephrostomy and 48.8% Foley type, and accidental dislodgement occurred in 26.3% of cases.
In multivariate analysis, we observed that first time nephrostomy tube placement entailed higher risk of accidental dislodgement than successive placements (odds ratio [OR] 1.95, confidence interval [CI] 1.01–3.74, p = 0.04). In the pigtail-type catheter patient subgroup, tubes placed by a resident were more prone to accidental dislodgement than those placed by an attending physician (OR 3.39, CI 1.29–8.91, p = 0.01), while first episode cases were more likely to have become dislodged than in a subsequent event (OR 3.17, CI 1.17–8.57, p = 0.02).
In addition, the mean (in days) until nephrostomy tube dislodgement in cases where this occurred was 20.32 ± 3.52 for pigtail and 60.92 ± 5.15 for Foley (p < 0.01 in Kaplan–Meier's test).
Conclusion:
Nephrostomy tube displacement in long-term patients is a common problem. Some factors associated with the catheter could increase the risk of involuntary displacement, such as being a first event or being inserted by less experienced resident doctors. In addition, pigtail type nephrostomies tend toward accidental dislodgement earlier than Foley ones.
Introduction
The use of percutaneous nephrostomy tubes is common practice in urology for upper urinary tract drainage, in different clinical contexts. Since the first designs in the 1950s, when polyethylene tubes were used through 10- to 14-gauge needles, different types and materials of nephrostomies have continued to evolve. 1 Each drainage design has specific differentiating characteristics, and urologists, who must be familiar with the different types, can choose the most appropriate one depending on patient characteristics or underlying disease. Defining characteristics of the ideal nephrostomy tube include good biocompatibility and strength, correct patient tolerability, acceptable resistance to obstruction or dislodgement, and great ease of insertion and replacement. 2
Two of the most commonly used designs are pigtail catheters and Foley catheters with a retention balloon. The pigtail types have a pigtail-shaped end that is positioned in the urinary tract to prevent accidental dislodgement. They are frequently used in pediatric patients due to the small diameters available on the market, with nephrostomy tubes ranging from 5F to 14F. 3 Some pigtail designs incorporate a self-retentive system, consisting of a nylon thread placed between the last side hole of the pigtail and the mouth of the catheter. By tightening this thread, the pigtail end remains fixed, preventing the curvature from falling apart, and theoretically decreasing inadvertent dislodgement of the catheter. Designs that do not incorporate this self-retentive system should be stitched to the skin. 4 Disadvantages reported with these nephrostomy tubes are that the pigtail is difficult to position in poorly dilated systems, and that small-diameter designs can easily become blocked due to clots or waste. 2
The other design considered in this study is the Foley catheter with balloon tube, whose diameters range between 12F and 32F, depending on the manufacturer. These nephrostomy tubes, similar to a urethral catheter, have an open tip to be inserted using a guidewire and a balloon at the end, usually with a capacity of about 3 mL, to be positioned in the urinary tract. Their main advantage is their diameter, which makes it easier to drain clots or thicker liquid with sediment, while the drawbacks reported are the possibility of obscuring a calix with the balloon, or patient discomfort in the event of excessive balloon swelling. 2,5
Although nephrostomy tubes are widely used due to their high placement success rate (around 97%), rapid resolution of urinary tract obstruction, and possibility of placement under local anesthesia, the main drawback of these drainage systems is accidental dislodgement. 6 Nephrostomy tube dislodgement increases the risk of infection and bleeding, as well as the need for surgical reinterventions for nephrostomy tube reinsertion. Although it is suspected that factors such as obesity, reduced mobility, or the patient cognitive state may have a role in dislodgement of the nephrostomy tube, no studies with strict design and large samples can be found in the literature that have examined predictive factors in patients with long-term catheters. 7
The objective of this study was to determine possible risk factors for accidental nephrostomy tube dislodgement and compare two different tube types in this context in patients with chronic catheters.
Materials and Methods
Study design and population
We conducted a retrospective, comparative, observational study in a single center. All surgical events of nephrostomy placement in our center were collected, including in the study only patients who had worn the nephrostomy tube for over a month. The first episodes were all to solve an acute obstruction, and none of the first episodes was placed after surgery. Electronic medical records were accessed to check follow-up and record variables. Exclusion criteria were cases of transient nephrostomy tube placement for events such as urgent antegrade flexible ureteroscopy or antegrade ureteral catheterization. The time frame was between May 2015 and December 2018. Cases before May 2015 were not collected due to the use of paper records at that time.
This study was approved by the Ethics and Scientific Committees of the University Hospital of Valencia Health Research Institute (INCLIVA).
Catheter designs
The study examined the two catheter types used in our center for percutaneous drainage of the upper urinary tract: pigtail-type catheters without self-retentive mechanism and Foley catheters. The Pigtail tubes were 8F to 10F, Percuflex® (Boston Scientific), while the Foley type was 12F, Superglide® (Teleflex). The placement methods were the same in all cases, with the patient in Valdivia position, and with ultrasound-guided puncture and supported by intraoperative X-rays. In all cases a skin dressing was used to help fix the catheter. The pigtail-type tubes were stitched to the patient's skin, while in the Foley type, 3 mL of distilled water was used in the balloon as a retention mechanism. Choice of design was completely at the urologist's discretion, according to preference and personalized to each case. Also, all catheters were placed by an urologist.
Recorded variables
Age, gender, and body mass index (BMI) were recorded as the subjects' baseline characteristics in all cases included in the study.
It was also noted whether or not the patient was oncologic, defined as requiring nephrostomy placement to resolve obstructive uropathy caused by a neoplasm, regardless of tumor origin. The nephrostomy tube design used (pigtail or Foley) was also registered in each case, together with the placement side (right or left).
Each nephrostomy tube event was recorded, noting whether or not dislodgement had occurred, if the patient had reached the scheduled replacement date with the tube in place, number of days elapsed until dislodgement or scheduled replacement, and if the catheter had needed changing due to obstruction or infection. Also recorded were whether this was the patient's first nephrostomy or a successive event, and finally, the status of the surgeon who placed the nephrostomy (attending or resident physician).
Statistical analysis
For the statistical analysis, each nephrostomy placement counted as a different case, so if the same patient had more than one nephrostomy tube inserted (due to replacements or dislodgements), several events were recorded in the same patient, one event per catheter placed.
We first performed descriptive analysis to show the baseline characteristics of the sample in percentages and means. Univariate and multivariate analyses were carried out to perform comparative analysis, first seeking to associate possible risk factors with inadvertent nephrostomy tube dislodgement, without differentiating the tube design used. Next, two subanalyses were carried out to establish the risk factors for accidental nephrostomy tube dislodgement, this time separating the sample according to tube design. In the case of pigtail catheters, the possible influence of catheter size was studied within the subanalysis, but not within the Foley, as they were all the same size. Variables with a tendency to statistical significance (p < 0.3) in the univariate analysis were included to carry out the multivariate analysis. The Mann–Whitney U test was used to compare means in the univariate analysis, and to compare percentages, the chi-square test was used, while binary logistic regression was used for multivariate analysis. In some cases, a Fisher's exact test was used to compare percentages that came from an absolute value of <5.
Finally, survival analysis (Kaplan–Meier's test) was carried out, recording the days elapsed until nephrostomy tube dislodgement (where applicable), dividing the sample according to tube design (pigtail type or Foley). Differences of p < 0.05 were considered statistically significant.
Results
A total of 205 cases in 70 patients were collected, with a mean age of 67.11 ± 10.21 years. Baseline characteristics of the sample are shown in Table 1; the majority of patients were male (61.4%) and with underlying oncologic disease (80.9%). The number of patients with each nephrostomy tube design was similar, with 51.2% of cases pigtail-type nephrostomy tube and 48.8% Foley type, and accidental dislodgement occurred in more than a quarter of cases (26.3%). There was no difference in criteria for choosing the catheter design depending on whether it was an oncologic patient or not. Of the 105 cases of pigtail, 84 (80%) are placed in oncologic patients. On the contrary, of the 100 cases with Foley catheters, 82 (82%) were used in cancer patients.
Basal Characteristics of the Studied Sample
Five pigtail and five Foley.
Four pigtail and four Foley.
SD = standard deviation.
Tables 2 and 3 show comparative analysis of the possible factors influencing nephrostomy tube dislodgement, without differentiating nephrostomy tube type. Being an oncologic patient and experiencing a first nephrostomy event were pinpointed as variables with a tendency to statistical significance in the univariate analysis. Finally, in the multivariate analysis it was concluded that first-time nephrostomy tube placement entailed 1.95 times higher risk of accidental dislodgement than successive placements (odds ratio [OR] 1.95, p = 0.04).
Univariate Analysis
Chi-squared.
Mann–Whitney U.
BMI = body mass index.
Multivariate Analysis
Binary logistical regression.
CI = confidence interval; OR = odds ratio.
The subanalysis according to tube type is shown in Tables 4–6. Although Table 4 shows that the distribution of the different catheter designs was not homogeneous for the catheter episode, this bias is corrected with the subanalysis of Table 5, showing a different analysis for each catheter design. In the pigtail-type catheter patient subgroup, tubes placed by a resident were 3.39 times more prone to accidental dislodgement than those placed by an attending physician (OR 3.39, p = 0.01), while first episode cases were 3.17 times more likely to have become dislodged than in a subsequent event (OR 3.17, p = 0.02).
Comparative Study of Baseline Characteristics by Dividing the Sample According to Catheter Design
Chi-squared.
Mann–Whitney U.
Univariate Analysis in Subgroups, According to Catheter Model
Chi-squared.
Fisher's exact test.
Mann–Whitney U.
Multivariate Analysis in Subgroups, According to Catheter Model
Binary logistical regression.
Finally, survival analysis is shown in Figure 1. The mean (in days) until nephrostomy tube dislodgement in cases where this occurred was 20.32 ± 3.52 for pigtail and 60.92 ± 5.15 for Foley (p < 0.01 in Kaplan–Meier's test).
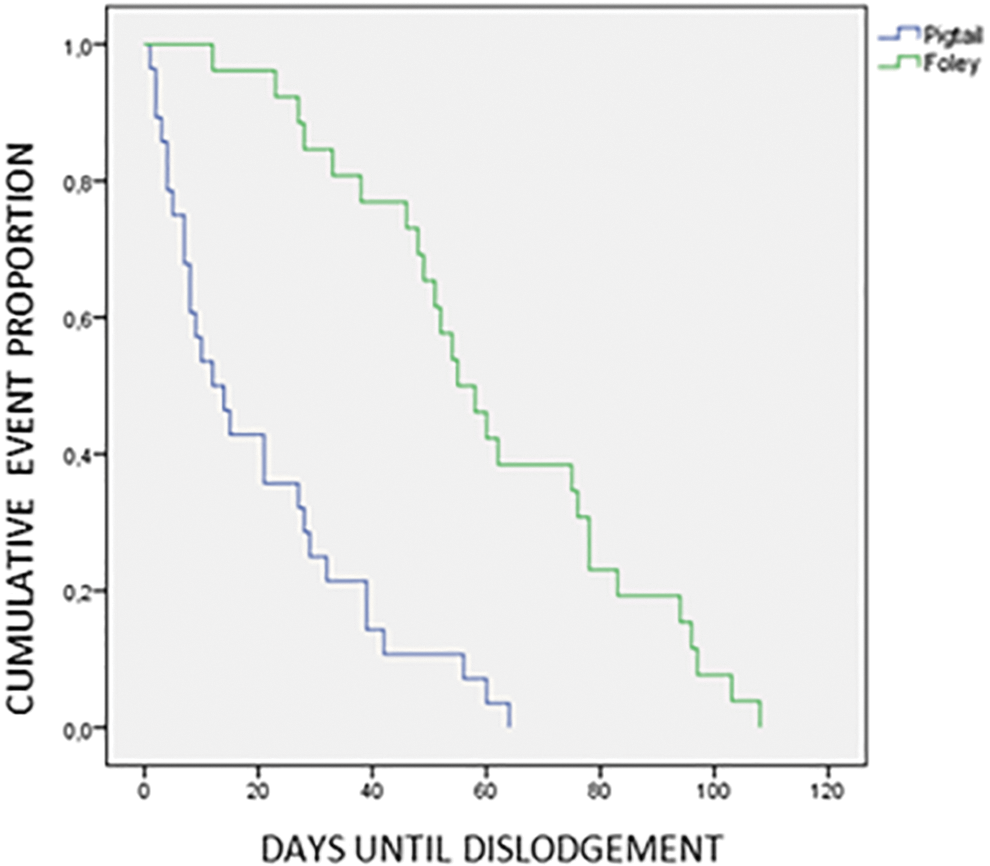
Survival analysis (in days) comparing the dislodgement times between cases with different catheter models. The average (in days) until the loss of catheters, in cases with accidental exit, was 20.32 ± 3.52 for pigtails and 60.92 ± 5.15 for Foley (p < 0.01 in the Kaplan–Meier test).
Discussion
The present study addresses accidental nephrostomy tube dislodgement, a problem frequently seen in urology services. The incidence study, with the largest sample of 283 patients, found that at 6, 12, 24, and 36 months of placement, 26%, 36%, 53%, and 62% of patients, respectively, had experienced at least one tube dislodgement episode. 8 Nephrostomy tube dislodgement is important not only because of prevalence but also due to associated complications and reinterventions. For example, Meira et al. reported up to 9.5% complications after nephrostomy placement, 36.6% of which needed repositioning in successive interventions. 9 Despite the above statistics, nephrostomy dislodgement is a neglected area of study. As far as we know, ours is the largest sample collected with the objective of establishing predictive factors for nephrostomy tube dislodgement in long-term patients. Most studies of this kind include patients in the percutaneous nephrolithotomy postoperative period where catheters only have to be inserted for short periods of time, and their conclusions cannot be extrapolated to patients with chronic nephrostomy. 10,11 Our study is noteworthy in that almost 81% of the patients had underlying oncologic disease, providing a different clinical profile to patients with short-term nephrostomy tubes after percutaneous lithotripsy surgery. This, combined with our subanalysis of different catheter designs, and the greater number of variables collected than in other studies make these findings of interest to the urologic community.
The study most similar to ours, including patients requiring medium- to long-term nephrostomy tubes, reported 23% inadvertent dislodgement across a sample of 87 patients. Although this percentage is similar to our series (26.3%), Niwa et al. failed to establish predictive variables for nephrostomy tube dislodgement. 7 Our results, however, conclude that patients with first-time nephrostomy are almost twice as likely to experience dislodgement than those with successive events. This finding is logical, taking into account the specific care required for this type of drainage and the fact that the patient's experience contributes toward preventing dislodgement. This fact has not been included in other similar studies, and in our opinion is pivotal to the permanence of catheters. 4,7,9,12 Perhaps information campaigns targeted at nephrostomy patients could be effective and reduce accidental dislodgement rates, especially in first events when patients have little experience. The use of information campaigns in health care professionals has been viewed as an effective tool to reduce infection and complication rates in patients with chronic catheters, and extrapolating these campaigns to patients could be useful in the future to prevent nephrostomy tube dislodgements. 13,14
As previously mentioned, the most numerous studies on nephrostomy center on percutaneous nephrolithotomy, and are hence not comparable with our sample because they are worn only for a few days. Some studies with large samples concluded that certain factors such as obesity are related to dislodgement, although our study revealed no such relationship. Bayne et al., studying 475 cases, report that for every additional BMI unit the probability of dislodgement increases by 6%, putting forward the hypothesis that subcutaneous fat could play a role. In concurrence with our results, they found no relationship with other variables studied such as age or nephrostomy tube type. 10
Another interesting aspect of our findings is the subanalysis by catheter tube type. In the pigtail-type subanalysis, in addition to first events, placement by a resident urologist was found to increase the risk of dislodgement. Other urologic interventions such as transurethral resection have also shown higher complication rates if performed by novice surgeons. This indicates a need for proper supervision by experienced surgeons, even in seemingly simple interventions such as nephrostomy puncture. 15 Although we cannot clearly establish the reasons why pigtail catheters placed by residents have a greater tendency to dislodgment, some aspects related to the poor experience with handling these catheters could be important. In our opinion, factors such as not achieving a “natural” angle of entry of the catheter into the urinary tract, not achieving total deployment of the tip of the pigtail catheter, or poor fixation of the catheter to the skin could be frequent maneuvers in surgeons with less experience in catheter placement. In all cases, the residents were supervised by staff members and performed the same surgical technique to place the catheter. Perhaps the Foley catheter retention system (with balloon swelling) is less dependent on the surgeon's ability to achieve proper fixation.
Regarding survival analysis, it was noteworthy that time until dislodgement was around 20 days in the pigtail group compared with 60 days in the Foley group. This trend has already been described in previous studies. 7 Although no definitive explanation has been found, experience has taught us that Foley tube balloon failure starts to become frequent from the second month onward; during programmed replacements we frequently observe lower liquid levels in the balloon than was instilled during catheter insertion, and in inadvertent dislodgement cases, we repeatedly find the problem to be spontaneously deflated balloon, rather than puncture. In our opinion, replacement before the 60-day mark would probably reduce cases of accidental dislodgement in Foley catheters. Despite the many studies in the literature describing and comparing tube designs, the search for the perfect nephrostomy design remains a future challenge. 2,4,12
This study has various limitations, principally those inherent to its retrospective and observational character, and that the study was carried out exclusively in a single center. Another drawback is that although we analyzed multiple variables, others not studied such as patient cognitive status may be important in catheter maintenance (although only one patient had the diagnosis of dementia). In the specific case of the statistical analysis, we can observe that in Table 4 it could exist in bias, since the distribution of catheter designs is not homogeneous for the variable “episode”; however, this limitation was attempted to correct with the subanalysis shown in Table 5. In addition, the lack of random tube-type selection is significant, since surgeon ability could also influence the results via personal preference for a particular type of nephrostomy tube.
Conclusions
Nephrostomy tube displacement in long-term patients is a common problem. Some factors associated with the catheter could increase the risk of involuntary displacement, such as being a first event or being inserted by less experienced resident doctors. In addition, pigtail-type nephrostomies tend toward accidental dislodgement earlier than Foley ones.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.