
Abstract
Background:
To examine the impact of the Mayo adhesive probability (MAP) score on the surgical complexity of exposing the tumor during laparoscopic partial nephrectomy (LPN).
Patients and Methods:
Our study included 318 patients who underwent LPN from January 2017 to December 2018 at our institution. Patients were divided into a lower MAP score group (≤2, n = 172) and a higher MAP score group (≥3, n = 146). Perioperative outcomes were compared between the groups. The operative time was predominantly occupied by the dissection time and the warm ischemia time (WIT).
Results:
A higher MAP score was associated with a longer operative time (131 vs 110 minutes, p < 0.001) and longer dissection time (71 vs 54 minutes, p < 0.001), respectively. The estimated blood loss (EBL) increased in patients with a higher MAP score (50 vs 20 mL, p < 0.001). No significant difference was found with respect to the WIT (21 vs 20 minutes, p = 0.370). In the multivariate linear regression model, male gender (β = 11.199, p = 0.001), body mass index (β = 1.197, p = 0.008), and MAP score (β = 9.958, p = 0.002) were significantly associated with the prolongation of dissection time.
Conclusions:
The MAP score was significantly associated with the prolongation of dissection time during LPN. In addition, the EBL increased in patients with a higher MAP score. Therefore, the MAP score can predict surgical complexity of exposing the tumor in patients undergoing LPN.
Introduction
Partial nephrectomy (PN) is considered the optimal therapy for small renal tumors. 1 Laparoscopic partial nephrectomy (LPN) can achieve comparable oncologic control to open partial nephrectomy and can improve perioperative outcomes. 2,3 The advent of the DaVinci surgical system facilitates an increasing trend to robot-assisted partial nephrectomy (RAPN) during the past decades worldwide, especially for the treatment of complex renal malignancies. 4,5 However, LPN still serves as an important alternative when robot platform is not available in some centers.
Adherent perinephric fat (APF) is sticky visceral fat between the Gerota's fascia and the kidney parenchyma, the presence of which increases the difficulty of mobilizing the kidney and exposing the tumor during PN. Several studies have shown that APF increases the operative time but has no impact on the warm ischemia time (WIT) during RAPN. 6,7 Nevertheless, corresponding studies in LPN are rare. The Mayo adhesive probability (MAP) score, developed by Davidiuk and colleagues, is an image-based scoring system used to predict the presence of APF. 8 Growing evidence suggests that the MAP score is a reliable and accurate indicator for APF. 9,10 The primary objective of our article was to examine the impact of the MAP score representing APF before LPN on perioperative outcomes.
Patients and Methods
The retrospective study was approved by the institutional review board and the local ethics committee. Bilateral synchronous tumors, multifocal tumors, complicated tumors needing renal artery cold perfusion, and patients without complete clinical or radiographic data were excluded. A total of 318 patients who underwent LPN from January 2017 to December 2018 were included. Clinical data were obtained from our prospectively maintained database, including gender, age, body mass index (BMI), American Society of Anesthesiologists (ASA) score, Charlson comorbidity index (CCI), history of hypertension and diabetes, surgical approach, tumor size, and tumor side. Radiographic data were acquired to calculate the R.E.N.A.L. score and MAP score using preoperative CT or MRI as previously described. Two authors conducted the scoring process in an independent blinded (to each other) manner. The MAP score was calculated as previously described. 8 In brief, the length between the posterior renal capsule and the posterior abdominal wall at the level of the renal vein was scored (<1.0 cm = 0 points, 1.0–1.9 cm = 1 point, and ≥2.0 cm = 2 points) (Fig. 1). The stranding was measured using CT or T2-weighted fat-suppressed MRI (none = 0 points, mild/moderate stranding = 2 points, and severe stranding = 3 points) (Fig. 2). As the surgical technique has been described and validated previously, LPN was performed by two senior laparoscopic surgeons through either the transperitoneal approach or the retroperitoneal approach.

At the level of the RV, measuring the length between the renal capsule and the abdominal wall as the thickness of posterior perinephric fat. P = posterior; RV = renal vein.
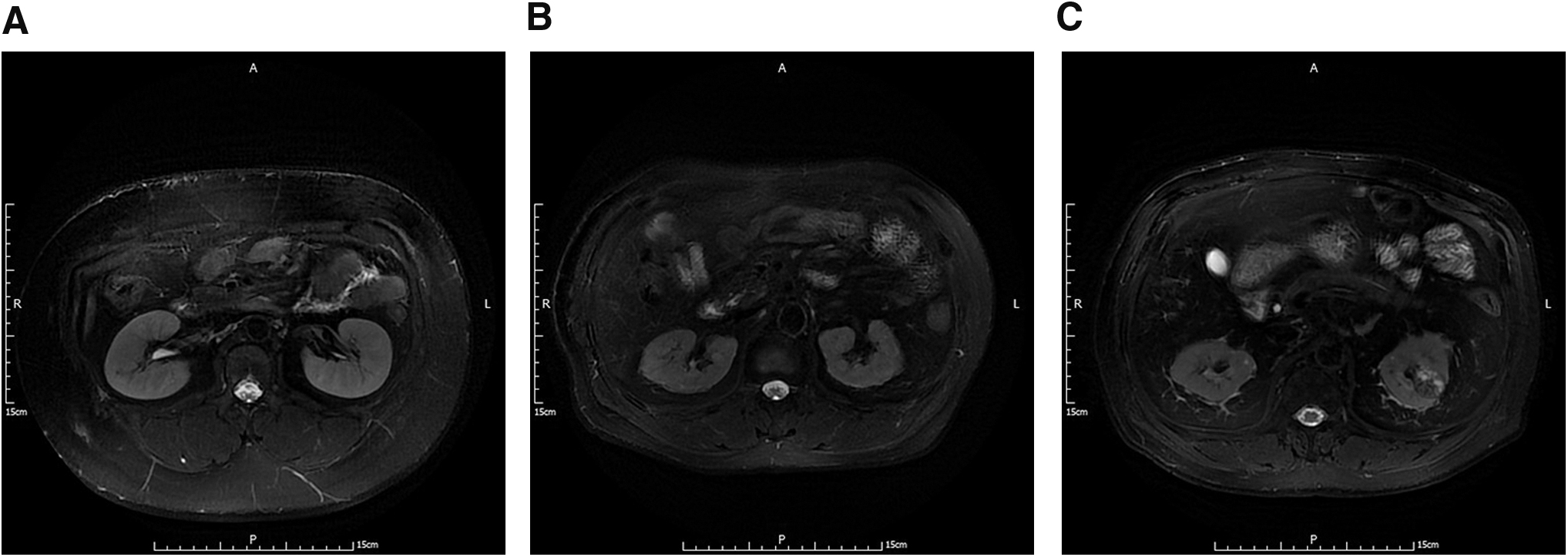
Grading of perinephric fat stranding.
Surgical data were collected from the operation records, including operative time, dissection time, estimated blood loss (EBL), WIT, blood transfusion, positive surgical margin, conversion to radical or open surgery, postoperative hospital stay, and postoperative complications. Dissection time was defined as the surgical duration from opening Gerota's fascia to artery clamping.
For statistical analysis, the median and interquartile range were applied for continuous data with a non-normal distribution. The Wilcoxon rank-sum test was used to compare the continuous variables, and Pearson's chi-square and Fisher's exact tests were used to compare categorical variables. Multiple linear regression was established and only the factors in the univariate analysis with a p-value <0.05 were included. SPSS 20.0 statistical software (SPSS, Inc., Chicago, IL) was applied in the analysis, and statistical significance was deemed to be a two-sided p-value of <0.05.
Results
The baseline characteristics of the cohort are presented in Table 1. A total of 318 patients were included in the study, among whom 146 patients had a higher MAP score (≥3). In accordance with multiple earlier studies, including ours, 11,12 male gender showed a predominant prevalence in the patients with a higher MAP score (88.4% vs 58.7%, p < 0.001). Both median age (54 vs 51 years, p = 0.003) and BMI (26.2 vs 25.0 kg/m2, p < 0.001) were higher in patients with a MAP score ≥3. In addition, the morbidity rate of diabetes was higher in the patients with a MAP score ≥3 (19.2% vs 9.3%, p = 0.011).
Baseline Demographic and Tumor Characteristics
ASA = American Society of Anesthesiologists; BMI = body mass index; IQR = interquartile range; MAP = Mayo adhesive probability.
Table 2 lists the perioperative outcomes of the groups. The operative time was significantly longer in patients with a higher MAP score (131 vs 110 minutes, p < 0.001). Similarly, the dissection time was 17 minutes longer in patients with a higher MAP score (71 vs 54 minutes, p < 0.001). A higher MAP score was associated with greater EBL (50 vs 20 mL, p < 0.001). No significant difference was found with regard to WIT or blood transfusion.
Perioperative Variables for the Groups
PSM = positive surgical margin; WIT = warm ischemia time.
The pathologic data are summarized in Table 3. Clear cell was the most common histologic subtype. In addition, there was no significant difference between the groups regarding the Fuhrman grade or pathologic T stage.
Pathologic Variables for the Groups
A multiple linear regression model was established to identify the influencing factors of operative dissection time (Table 4). According to univariate analysis, male gender (β = 16.398, p < 0.001), a higher BMI (β = 1.724, p < 0.001), and a higher MAP score (β = 15.100, p < 0.001) were significantly associated with the dissection time. According to multivariate analysis, male gender (β = 11.199, p = 0.001), BMI (β = 1.197, p = 0.008), and MAP score (β = 9.958, p = 0.002) were risk factors for dissection time.
Examining the Risk Factors Associated with Prolongation of the Dissection Time in a Multivariate Linear Regression Model
CCI = Charlson comorbidity index; CI = confidence interval.
Discussion
Urologists used to evaluate the surgical difficulty based on the tumor-specific factors such as the tumor size and location. 13 –15 However, urologic surgeons who perform LPN are also well aware that the presence of thick adherent fat makes the operation much more troublesome. Bylund and colleagues 6 reported that the operative time of patients with “sticky fat” was much longer than that of control patients. Kawamura and coworkers 16 demonstrated that APF was associated with greater EBL compared with a non-APF group. As shown in Figure 3, compared with normal perinephric fat, it is difficult to peel away APF from the kidney capsule.
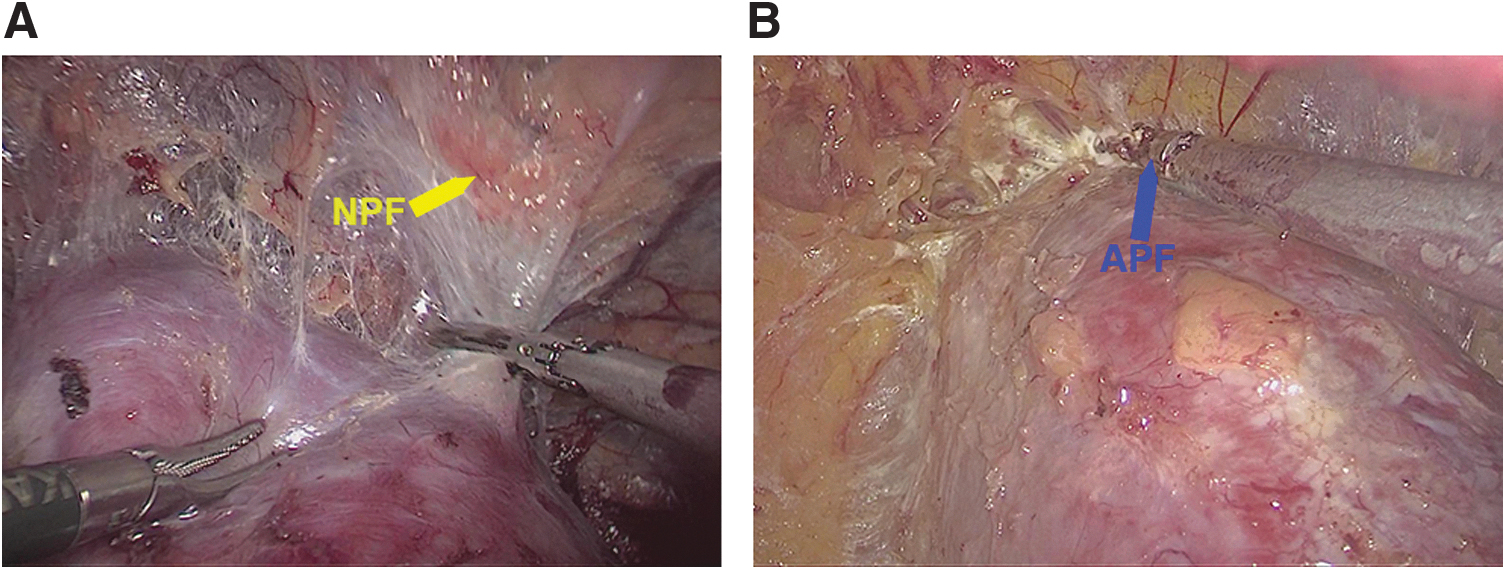
Intraoperative images captured during mobilizing the kidney.
The MAP score is a quantitative method for predicting the probability of encountering APF preoperatively. 8 The authors established a model with the highest area under the curve of 0.89, including posterior perinephric fat thickness and stranding. A comprehensive review summarized the publications discussing the factors associated with APF, and the results showed that the MAP score was a reliable indicator of APF across the different centers. 17
To date, existing evidence has focused on the relationship between APF and perioperative outcomes during RAPN. The impact of the MAP score on the surgical complexity during LPN remains unclear. Bier and coworkers 18 was one of the few to find that surgical time during LPN was significantly prolonged in the individuals with a higher MAP score; however, no significant correlation between MAP score and complications or WIT was observed. This study compared the perioperative outcomes in patients whose MAP score ≥3 with those in patients with a MAP score ≤2. The results showed that a higher MAP score was associated with a longer operative time (131 vs 110 minutes, p < 0.001) and dissection time (71 vs 54 minutes, p < 0.001) as well as increasing EBL (50 vs 20 mL, p < 0.001). On multivariate analysis, we found that male gender (β = 11.199, p = 0.001), BMI (β = 1.197, p = 0.008), and MAP score (β = 9.958, p = 0.002) were predictors of prolonged dissection time. Recent studies have indicated that men are more subject to developing APF than women. 10,16 Eisner and colleagues reported that male gender contributed to adipose tissue redistribution, from subcutaneous tissue to perinephric tissue. 19 The increased perinephric fat would lead to a chronic and systemic inflammation state called metaflammation. 20 Moreover, this increase also accelerates adipose tissue fibrosis and induces angiogenesis. 21 BMI has been proven to be significantly correlated with APF. 7,8 Our previous research found that BMI was associated with the thickness of posterior perinephric fat. 11 Therefore, the dissection time increased in the patients with a higher BMI. Taken together, we conclude that the MAP score representing APF is an indicator of the difficulty of peeling off the perinephric fat during LPN.
Ishiyama and coworkers discussed the relationship between the MAP score and the perioperative outcomes during RAPN. 22 They found that the total surgical time and dissection time in subjects with a higher MAP score were significantly longer than those with a lower MAP score, which was similar to our findings. However, some differences do exist between theirs results and ours. First, no significant difference was found with respect to the WIT (21 vs 20 minutes, p = 0.370) in our study. LPN was classified into two major phases: dissection time and WIT. The dissection time is the “first half” of the LPN (from opening the Gerota's fascia to artery clamping), during which surgeons dissect the perinephric fat to mobilize the kidney and expose the tumor. Obviously, a higher MAP score representing APF prolonged the duration of dissection time. The second half of the LPN (WIT) procedure starts when hilar artery is clamped. Since the perinephric fat has been peeled off, it is reasonable that the MAP score has no impact on the resection of the tumor. Second, EBL increased in the patients with a higher MAP score in our study, in concordance with the results of Khene and colleagues. 7 Their results showed that the presence of APF doubled the bleeding volume.
This study provides the first data on the relationship between the MAP score representing APF and perioperative outcomes in patients undergoing LPN. The results showed that the MAP score could serve as an indicator for surgical difficulty to make preoperative planning.
There were several inherent limitations in the study. First, it is possible that underlying selection bias existed because of the retrospective nature. For instance, the possible effect of smoking on the stickiness of the perinephric fat was not determined. In addition, the analysis was restricted to the patients with complete clinical and radiographic data available for review. Second, ranking the stranding of the perinephric fat in certain individuals is subjective in nature, especially for the mild (2 points) and the severe (3 points). Besides, the MAP score was calculated utilizing preoperative MRI or CT data. Because of different imaging principles, it is reasonable that discrepancies may exist in detecting the severity of perinephric stranding. Finally, this was a single-center study and further efforts from other institutions are necessary to validate our findings.
Conclusion
The MAP score was significantly associated with the surgical complexity of exposing the tumors, and it could predict the prolongation of dissection time during LPN. Preoperative planning can be made according to the MAP score.
Ethical Standards
Written informed consent was obtained from all patients. This study was approved by the protection of human subject committee, Chinese People's Liberation Army (PLA) General Hospital.
Footnotes
Authors' Contributions
Y.Y. did the data collection and article writing; Y.X. and P.L. were in charge of data management; L.G. performed the data analysis; K.L. did the data collection; Y.X. did article editing; Y.G. and X.Z. were in charge of project development.
Author Disclosure Statement
We have no potential conflict of interest.
Funding Information
This work was financially supported by the National Natural Science Foundation of China (No. 81702494).