
Abstract
Introduction:
The purpose of this study was to evaluate factors during ureteroscopy that can potentially impact procedure cost.
Materials and Methods:
A retrospective review of 129 consecutive elective ureteroscopy cases was performed to determine direct procedure cost. Direct cost was defined as cost incurred because of operating room expenses, including operating room time, staffing expenses, equipment, and supply costs. Data regarding patient, procedural, and operating room staffing characteristics were compared between the most and least expensive cases. Univariate and logistic regression analysis were performed to identify factors predictive of higher costs.
Results:
The average direct ureteroscopy cost was $3298/case. On univariate analysis, ureteroscopies in the highest 50th cost percentile had larger stone burden (170.1 vs 146 mm2; p = 0.03) and longer operative times (95.3 vs 49.9 minutes; p < 0.01), were more likely performed for non-stone indications (21.4% vs 7.2%; p = 0.03), more likely to include a resident (65.5% vs 43.6%; p = 0.02), and less likely to have a dedicated urology scrub technician (38.2% vs 61.8%; p = 0.01) compared to cases in the lowest 50th percentile. The presence of a resident, larger stone burden, absence of a dedicated scrub technician, and longer operative time were associated with an average cost increase of $516, $700, $1122, and $1401, respectively. Logistic regression analysis showed that operating room time was the only factor predicting higher cost (OR [odds ratio] 12.8, 95% confidence interval [CI] 2.0–84.0). A post-hoc logistic regression analysis demonstrated that the presence of a resident during ureteroscopy (OR 2.9, 95% CI 1.1–8.0) and larger stone burden (OR 1.01, 95% CI 1.0–1.013) were significantly associated with longer operative times.
Conclusion:
Operating room time is the primary determinant of ureteroscopy case cost. All efforts should be made to decrease operative time, although balancing patient safety and maintaining a quality training environment.
Introduction
The annual cost of treating urolithiasis in the United States is estimated to be $3.79 billion in 2014. 1 The rising prevalence of stone disease and the increasing costs associated with the diagnosis and treatment of stones suggest that these costs will continue to rise. 2 –4 Recent studies have demonstrated that ureteroscopy has become the most common method of treating nephrolithiasis in the United States. 5 The widespread adoption of this modality is largely attributed to rapid advances in endourologic technology and techniques that have made ureteroscopy a safe and effective option for patients.
Despite the advantages of ureteroscopy over other stone treatment options, there remains a potential for high financial burden for surgeons unaware of factors that may influence case cost. Global estimates of case cost have shown that the average cost of a ureteroscopic procedure in the United States is 3-fold higher than the cost in Europe, 10-fold higher than the cost in Canada, and approximately 16-fold higher than in Turkey. 6 Previous studies have identified variables that can impact cost during ureteroscopy, including the type of ureteroscope used (disposable vs reusable), reusability of laser fibers, equipment repairs, and method of stone treatment (dusting vs basketing). 7 –10 These factors can have synergistic or antagonistic affects and can interplay with additional factors in the operating room environment to influence procedural costs. The individual findings of these studies demonstrate that there are multiple factors that can impact cost in the operating room and suggest that there are likely additional arcane variables yet to be identified.
The purpose of this study was to evaluate the overall impact of patient, surgical, and staffing-related factors upon the cost of ureteroscopy.
Materials and Methods
After institutional review board approval, a retrospective review of 129 consecutive elective ureteroscopy cases in a single tertiary care academic medical center between June, 2017, and May, 2018, was performed. Included patients were 18 years of age or older, those who underwent elective ureteroscopy for stone and non-stone diagnoses, and those having available information relating to case cost. Exclusion criteria were pediatric cases, cases performed in a nonelective setting, bilateral ureteroscopy cases, and cases with no available cost data.
All ureteroscopy procedures were performed in a conventional academic tertiary care hospital operating room platform with seven operating rooms that allow for performance of both inpatient and outpatient surgeries. In general, semirigid ureteroscopy was used for stones located below the iliac vessels in males and for some proximal ureteral stones in females. Flexible ureteroscopy was used for proximal ureteral stones in men and all renal stones. Intermittent irrigation was provided using two 60 mL syringes with saline. Dusting vs basketing was selected based on surgeon preference.
Direct procedural cost to the hospital for each case was obtained from the billing department. This was the cost incurred by the hospital because of operating room expenses and included operating time costs, operating room staffing costs, equipment costs, and disposable supply costs.
The dependent variables were categorized into patient-related factors, procedure-related factors, and staffing-related factors. Patient-related factors included patient demographics (age, body mass index [BMI], and American Society of Anesthesiologists [ASA] score) and total stone burden. Total stone burden was calculated by multiplying the length and width of the stone(s), resulting in the stone surface area. For patients with more than one urinary stone treated, the sum of each stone's surface area was used as the total stone burden.
Procedure-related factors included indication for ureteroscopy (stone vs other), stone treatment technique (dusting vs basketing), ureteroscope type (semirigid vs flexible), stone location (lower pole vs other and kidney vs ureter), use of access sheaths, preexisting stent before ureteroscopy, use of pigtail stents at the conclusion of case, and average operating room time.
Staffing-related factors included the level of training of the attending staff (urologist vs all other), years of attending staff experience (≥10 years of practice vs <10), presence of trainees in the case (residents/fellows), presence of a dedicated urology scrub technician, and presence of a dedicated circulating nurse. All ureteroscopy cases included a dedicated radiology technician to operate the c-arm, so this was not included as a variable in the analysis.
Cases were stratified by average direct cost into the highest and lowest 50th percentile for cost. Univariate analysis was performed using both the Mann–Whitney U (for nonparametric data) and chi-square test (for categorical data) to identify factors associated with higher case cost, with p < 0.05 considered significant. Logistic regression analysis was then performed to identify factors predictive of higher costs. A post-hoc analysis was performed to identify factors predictive of longer operative time.
Results
A total of 108 ureteroscopy cases, including complete data sets, were available for analysis. Table 1 summarizes patient, procedure, and staffing characteristics. The average stone burden was 120 mm2 and average operating room time was 71.5 minutes. The average case cost was $3298, with 76.9% of cases being profitable. The majority of ureteroscopy cases (85.3%) were performed for stone treatment, with 68.5% employing the dusting technique. Access sheaths were used in only 5.6% of cases and a stent was placed at the end of the procedure in 94.5% of cases. In regard to staffing, a fellowship-trained urologist performed 54.6% of the cases, a dedicated urology scrub technician was in the operating room in 47.7% of cases, and a resident scrubbed 54.6% of cases, whereas a fellow was in 26.8% of the cases.
Patient, Procedural, and Staffing Characteristics of Ureteroscopy Cases
BMI = body mass index; URS = ureteroscopy.
Figure 1 illustrates univariate analysis of patient characteristics in cases in the highest 50th percentile for cost compared to cases in the lowest 50th percentile. There were no differences in patient age, BMI, ASA score, or gender (p > 0.05). The average stone burden was significantly higher in cases in the highest 50th percentile for cost (170.1 vs 146.0 mm2; p = 0.03). When stratified by stone burden, the average ureteroscopy cost increased with increasing total stone burden (Fig. 2).
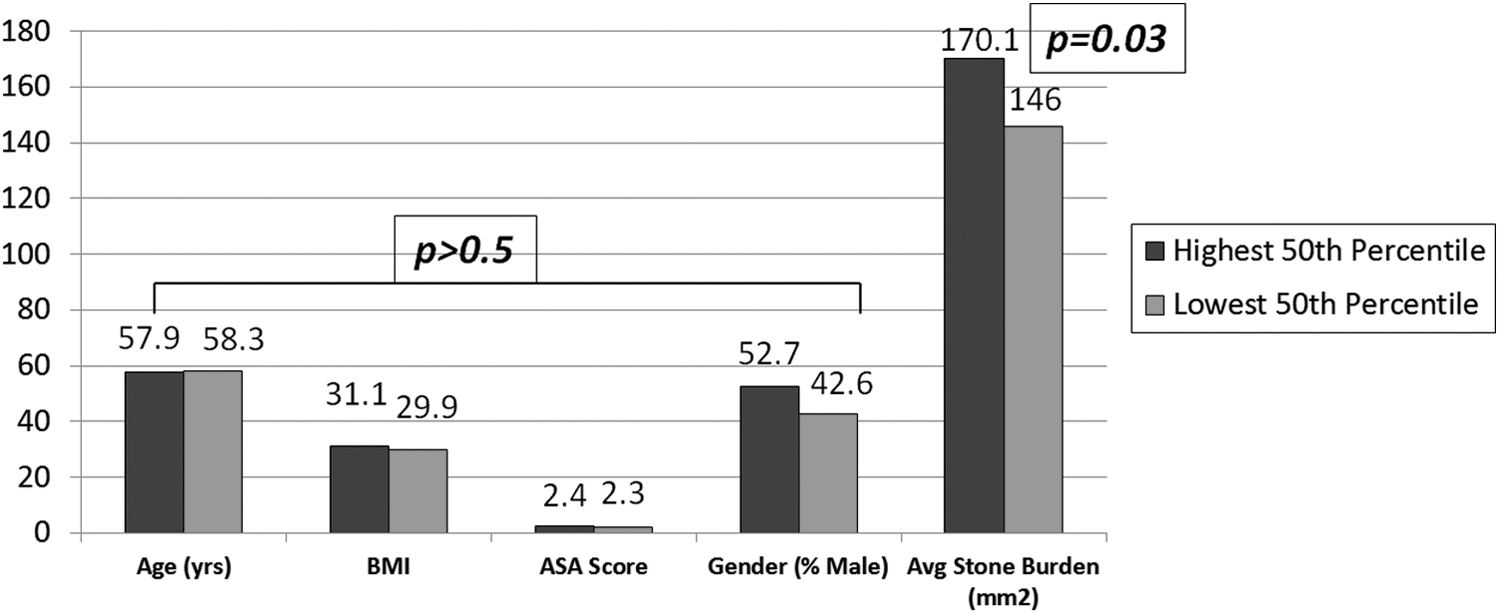
Impact of patient-related factors on ureteroscopy cost.
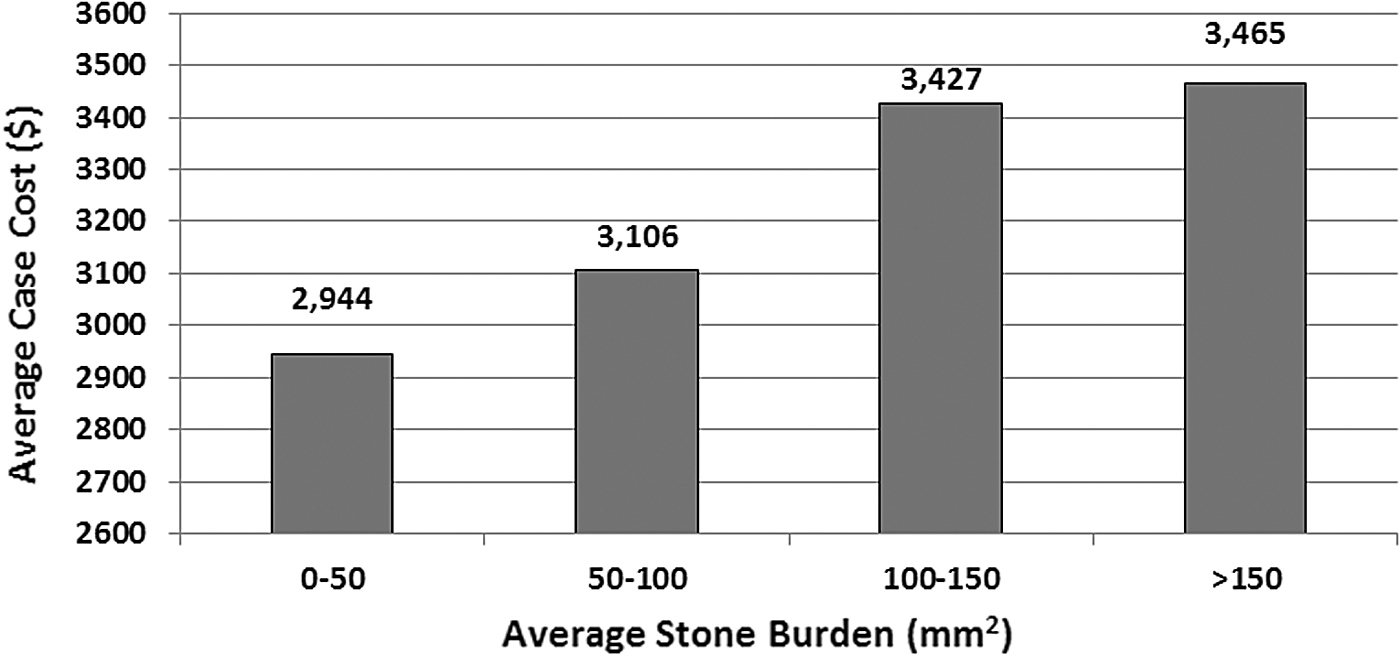
Average ureteroscopy case cost (in U.S. dollars) stratified by average stone burden treated.
In regard to procedure characteristics (Fig. 3), the percentage of ureteroscopy cases performed for non-stone indications and the average operating room time were both significantly higher in cases in the highest 50th percentile for cost, whereas the stone location (lower pole vs other and kidney vs ureter), stone treatment technique, type of ureteroscope used (semirigid vs flexible), and the use of access sheaths or stents were not significantly different.

Impact of surgical-related factors on ureteroscopy cost.
In regard to staffing characteristics (Fig. 4), the factors that were significantly higher in cases in the highest 50th percentile for cost were the presence of a resident in the case (65.5% vs 43.6%, p = 0.02) and the absence of a dedicated urology scrub technician (61.8% vs 38.2%, p = 0.01). When stratified by resident training year (junior [Uro-1 and Uro-2] vs senior [Uro-3 and Uro-4]), there was no difference between highest and lowest percentile for cost (senior scrubbed in 87.1% vs 94.1%, p = 0.45). The presence of a fellow, the presence of fellowship trained endourologist, the years of attending practice (≥10 years), or the presence of a dedicated circulating nurse had no effect on cost. Similar trends were found when cases were stratified by highest and lowest tertile for cost (Table 2).
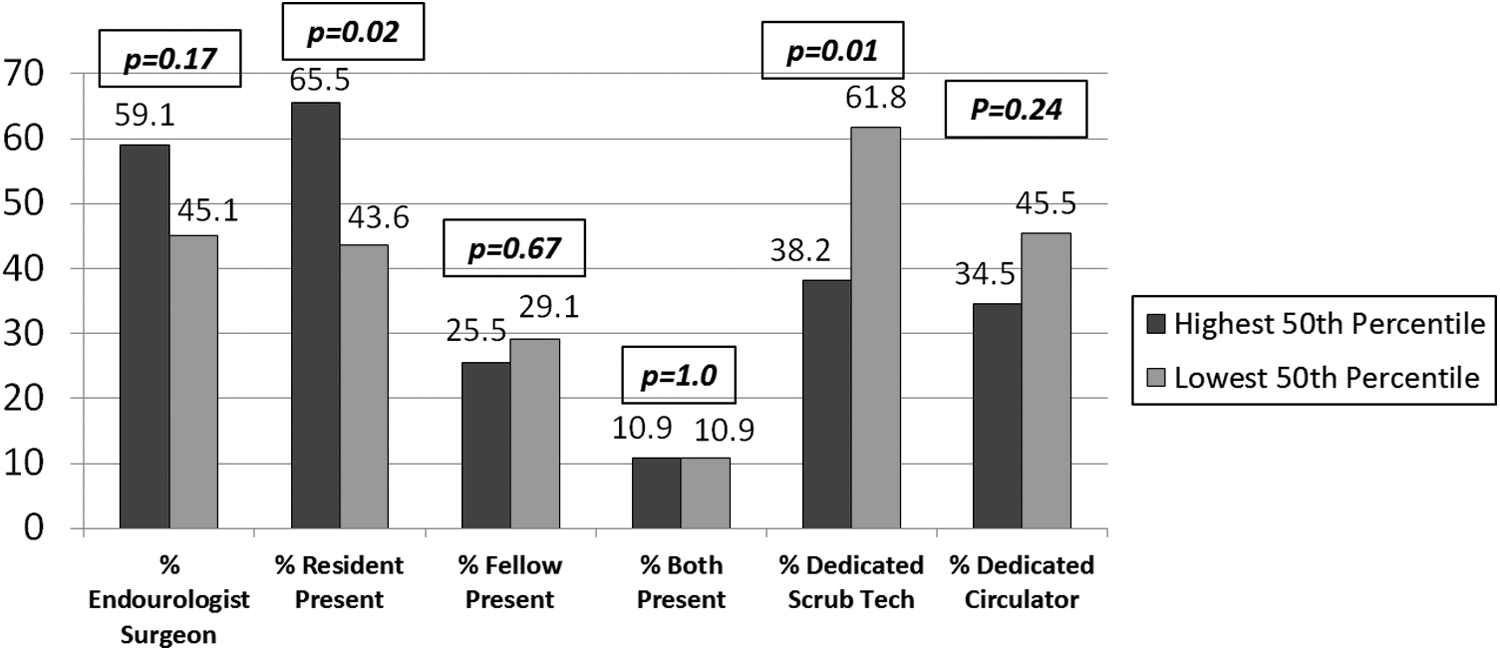
Impact of surgical staffing on ureteroscopy cost.
Significant Factors on Univariate Analysis When Case Cost Was Stratified by 50th Percentile and by Tertile
The influences of significant factors affecting cost on univariate analysis are demonstrated in Figure 5. The presence of a resident in a case, larger stone burden (>100 mm2), absence of a dedicated urology scrub technician, and longer operative time (>1 hour) were associated with an average increase in case cost of $516, $700, $1122, and $1401, respectively. On multiple logistic regression analysis, operating room time was the only factor to remain significantly associated with higher case cost (OR [odds ratio] 12.8, 95% confidence interval [CI] 2.0–84.0) (Table 3).
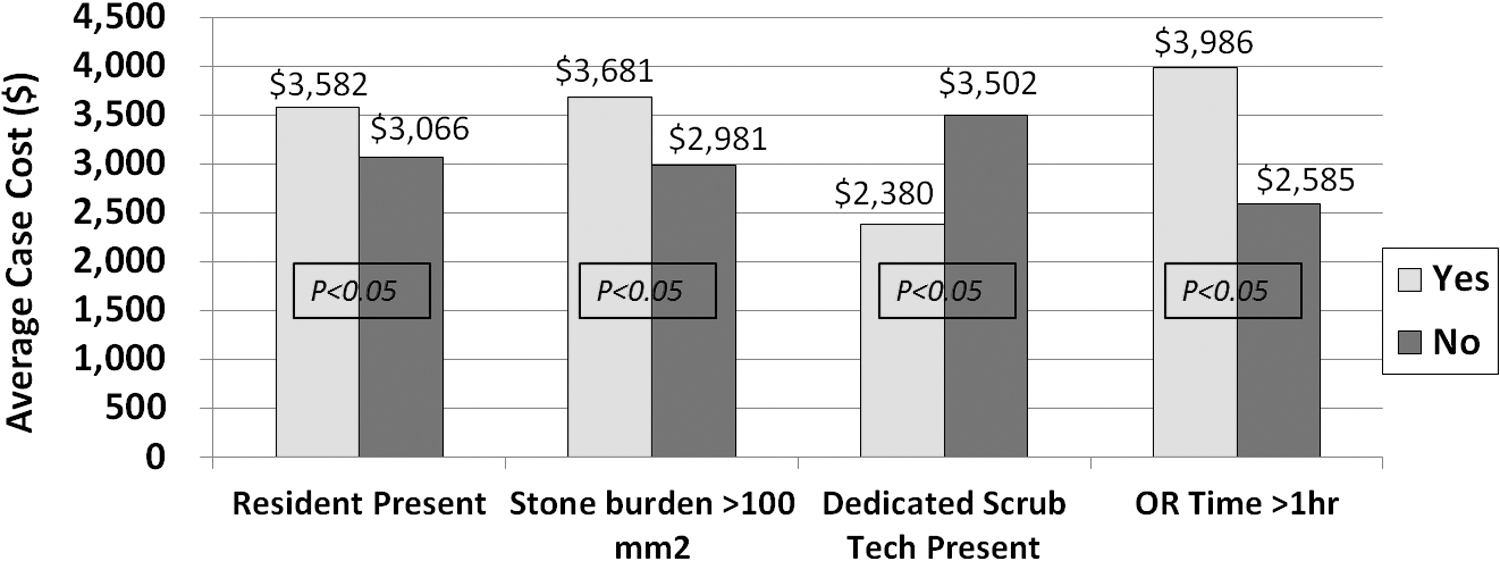
Difference in average case cost stratified by variables significant in univariate analysis.
Logistic Regression Analysis of Factors Predictive of Higher Ureteroscopy Case Cost
CI = confidence interval.
A post-hoc multiple logistic regression analysis was performed to identify factors associated with longer operative times. The presence of a resident during ureteroscopy (OR 2.9, 95% CI 1.1–8.0) and larger stone burden (OR 1.01, 95% CI 1.0–1.013) were significantly associated with longer operative times.
Discussion
In this analysis of 108 ureteroscopies, we found that operative time was the only factor to remain predictive of higher case cost on multivariate analysis. Our data support a similar finding by Litwin et al., who estimated that 74% of ureteroscopic procedure resources are dependent on operative time. 11 The significant impact of time in the operating room on the financial burden of this procedure does not come as a surprise. In a study by Childers and Maggard-Gibbons evaluating the cost of care in the operating room, the average cost of one minute was estimated to be $36. 12 Moreover, the same study demonstrated that the cost per minute in the operating room has steadily increased over the last decade. These data are consistent with the findings of our study, which highlight the significant contribution of operating room time on overall case cost. The high cost of additional operating room time, even if just a few minutes, trumps the disposable cost in determining the ultimate cost of the ureteroscopic procedure. For example, if the surgeon did not open a $63 glidewire to get past an impacted stone, but spent an additional 3 minutes trying to get a standard wire past the stone, then that equates to a net additional cost of $45 ([cost of 1 minute in operating room ($36) × 3 minutes] − cost of guidewire ($63) = $45).
Although operating room time was the only predictor on multivariate analysis, we sought to evaluate additional factors that may impact operating room time and subsequently influence cost. A larger stone burden, the presence of a resident in the case, and absence of a dedicated surgical assistant were all factors significant on univariate analysis when cases were stratified by 50th percentile for cost. Similar trends were also found using a more stringent comparison of top tertile for cost vs lower tertile for cost, except for cases performed for non-stone-related indications (Table 2). Although these factors were not predictive of cost on multivariate analysis, a post-hoc analysis of factors impacting operative time as an indirect surrogate for cost demonstrated that the presence of a resident and a larger stone burden were both predictive of longer operative times. This corroborates the hypothesis that factors impacting operating room time likely contribute to higher case cost.
An additional interesting finding on univariate analysis was that ureteroscopy cases in the highest percentile for cost were more likely to have been performed for non-stone indications. A subgroup analysis comparing ureteroscopies performed for non-stones to ureteroscopies performed for stones did not demonstrate any difference between operative time, presence of a resident, or presence of a scrub technician. We hypothesize this difference in cost may be related to the additional surgical equipment and supplies necessary for performing endoscopic tumor resections and ureteral stricture dilations. However, because of the small number of patients who underwent ureteroscopy for non-stone indications, future studies to examine this cost difference are necessary.
Our findings are supported by other studies examining the individual impact of similar factors on operative time. In a study by Babineau and colleagues, introduction of a surgical residency into a hospital significantly increased operative time for multiple surgical procedures, and the study concluded that the added time equated to an increased cost burden to the hospital. 13 Similarly, Allen et al. found that the presence of a resident was significant in determining the operative time and led to increased costs during surgical cases. 14
To improve resident efficiency in the operating room, structured training models aimed at improving proficiency have been proposed. Kim et al. implemented simulation-based training for junior urology residents to overcome the learning curve associated with flexible ureteroscopy. 15 This model consisted of a pretraining assessment, independent practice sessions and post-training assessment with residents receiving expert feedback. The study demonstrated that this method of simulation-based training significantly improved performance scores and reduced task completion times for residents performing ureteroscopy. Similar models have also been implemented in robotic urologic procedures to improve resident proficiency and reduce the impact on operative time. In a study by Rebuck and colleagues, modifications in operating room processes were implemented to determine if the times and costs that are associated with robot-assisted radical prostatectomy in an academic center could be reduced. 16 These modifications included resident adherence to time-oriented surgical goals, use of a dedicated anesthesia team, simultaneous team processing during room turnover, and elimination of unused instruments. By implementing these modifications, operating room costs were reduced by 28%. In a similar study by Rashid and colleagues, a systematic approach of teaching robot-assisted prostatectomy consisting of appropriate supervision, graduated responsibility, real-time feedback, and objective measurement of progress demonstrated both a significant improvement in resident proficiency and a reduction in mean operative time. 17 The findings of our study that residents may impact case cost would advocate that such models may be necessary not only for resident education but also as a tool to reduce case cost. Certainly, resident training is a priority and we are not suggesting that training be sacrificed for cost-effectiveness, but rather would encourage solutions that continue to provide excellent education, although decreasing cost.
Regarding the impact of stone burden, two studies investigating the use of preoperative stents showed that overall, stones >1 cm in size had a significantly longer operative time than stones ≤1 cm in size. 18,19 The cost for treatment of stones >1 cm was higher than the cost for stones ≤1 cm in size, regardless of whether or not the patient had been stented preoperatively. 19 Similarly, our data show that ureteroscopy case cost rises proportionally with increasing stone burden. Perhaps in a manner similar to bladder tumors, stone reimbursement rates should consider the size of the stone.
Another variable found to be associated with more expensive cases in our study was the absence of a dedicated urology scrub technician to assist in the case, whereas a dedicated circulating nurse had no effect. In our institution, the scrub technician has the primary responsibility for pulling and opening the appropriate equipment, assembling and preparing the equipment, and is scrubbed during the case assisting the surgeon. Subsequently it is intuitive that a well-trained scrub technician could reduce operating room time and minimize the impact of the circulating nurse. This is likely related to efficiency as previous studies have shown that utilizing consistent non-physician staffing in the operating room results in improved efficiency and decreases the overall length of operation. 20 To our knowledge, our analysis of ureteroscopy cases is the first to investigate these multiple variables simultaneously and evaluate for interactions that may potentiate or mitigate their significance.
We acknowledge that other factors that were not significant or were not examined in our study could contribute to the cost of ureteroscopic procedures. In a prospective multicenter trial by Humphreys and colleagues that investigated the efficacy of stone dusting vs basketing, it was shown that basketing procedures had significantly longer operative times than dusting procedures. 10 We did not find a similar association; however, the majority of the patients in our cohort underwent dusting, thus limiting the power to detect a difference between those two modalities. There is also evidence that laser fibers have an impact on case cost. Chapman et al. found that despite the initial cost, disposable laser fibers were more cost-effective than reusable laser fibers for ureteroscopic lithotripsy because disposable fibers caused less damage to the ureteroscope and negated resterilization costs. 8 Even though the authors suggested that disposable laser fibers saved time, time was never investigated as an independent variable against cost of ureteroscopy. At our institution, laser fibers were all disposable and subsequently, we were unable to compare the cost-effectiveness of disposable and reusable fibers. In addition, our institution holds a vendor contract that covers the cost of ureteroscope repairs for the duration of the contract. Thus, we were unable to determine the impact of ureteroscope repair on case cost, which other institutions must take into consideration. Furthermore, our institution does not use disposable ureteroscopes, and subsequently, the effect of these disposable ureteroscopes on cost could not be determined. Also, this retrospective analysis was unable to account for the cost of wasted equipment (open/unused supplies) or wasted operating room time (nurse leaving to get equipment not present in the operating room and equipment malfunctions). Future prospective studies designed to evaluate the cost of these factors will be necessary. Despite these limitations, we feel that our novel analysis highlights that operative time is the dominant driver for case cost during ureteroscopy.
Conclusion
Operating room time is the primary determinant of case cost during ureteroscopy. Indirect factors that can increase procedure cost include large stone burden, resident training, and availability of dedicated operating room staff. All efforts should be made to decrease operative time to decrease cost, although balancing patient safety and maintaining resident education.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.