
Abstract
Objectives:
To assess the association of skin-to-stone distance (SSD) and stone-free rates following extracorporeal shockwave lithotripsy (SWL) using two statistical methods: logistic regression and a matched-pair analysis approach.
Patients and Methods:
Patients with a solitary radio-opaque upper ureteral calculus diagnosed on noncontrast computed tomography were included. Patients were treated with a Sonolith I-Sys Lithotripter (focal depth 17 cm). Stone treatment success was defined as stone free (fragments ≤3 mm) at 3 months. Failure was defined as persistent fragments beyond 3 months or requirement for intervention with ureteroscopy. The outcome was assessed by a plain kidney, ureter, and bladder radiograph (KUB) at 2 weeks. Logistic regression was used to determine association of patient and stone factors with treatment failure. The patient cohort was divided into tertiles by SSD, and matched-pair analysis was undertaken between individuals from the top and bottom tertiles (SSD ≤12 cm and SSD ≥14 cm). Matching criteria consisted of age, sex, maximum stone diameter (±2 mm), and stone density (±250 HU).
Results:
From a database of 2849 patients who underwent SWL, 397 patients were identified who had treatment of a single upper ureteral stone. Age (odds ratio [OR]: 1.03, 95% confidence interval [CI]: 1.01–1.04, p = 0.007), SSD (OR: 1.16, 95% CI: 1.03–1.32, p = 0.02), stone side (OR: 1.65, 95% CI 1.01–2.73, p = 0.05), stone diameter (OR: 1.09, 95% CI: 1.00–1.19, p = 0.05), and multiple sessions (OR: 4.65, 95% CI: 2.61–8.29, p < 0.001) were significantly associated with treatment failure by logistic regression univariable analysis. Multiple sessions was the only factor significantly associated with treatment failure on multivariable analysis (OR: 4.03, 95% CI: 2.18–7.42, p < 0.001). From a cohort of 141 patients with SSD ≥14 cm and 174 patients with a SSD ≤12 cm, 66 matches were identified (132 patients). Forty-nine patients (74.2%) with SSD ≥14 cm were deemed stone free at follow-up vs 51 patients (77.3%) with SSD ≤12 cm (p = 0.85).
Conclusion:
This study demonstrates by two statistical methods that SWL can provide efficacious treatment of upper ureteral stones in obese patients and that the upper threshold of SSD for SWL with Sonolith I-SYS could be revised to allow these patients the benefits of SWL.
Introduction
The worldwide epidemic of obesity, currently affecting over 650 million people, presents challenges to the effective treatment of urolithiasis. 1 The likelihood and recurrence rate of stone formation display a positive correlation with obesity, with a specifically increased risk of uric acid and calcium oxalate stones. 2 The management of urolithiasis can be influenced by patient obesity, in terms of diagnostic imaging and treatment modality selected, with adverse effects on treatment efficacy and perioperative morbidity risk. 3
The success of extracorporeal shockwave lithotripsy (SWL) has been linked to a number of factors, including stone size, location, and HU, as well as technique and patient body habitus. 4 Skin-to-stone distance (SSD) has been shown to be a stronger predictor of SWL success than body mass index (BMI). SSD is influenced by the amount of subcutaneous and visceral fat, as well as the renal parenchymal thickness and position of the stone. 5 The SSD has been found to be a strong predictor of treatment failure during the use of SWL for intrarenal stones by a number of studies. SSD of ≥7.9 cm, ≥9 cm, and ≥10 cm has variously been demonstrated as predictive of treatment outcome. 6 –8
Park and colleagues reported that SSD >7.8 cm was associated with failure in a cohort of 43 patients with renal stones treated with a Sonolith Praktis electroconductive lithotripter (EDAP TMS, Vaulx-en-Velin, France). 6 Perks and coworkers reported greater SWL treatment success rates of 79% where SSD <9 cm, vs 57% for those with SSD ≥9 cm, for renal stones using an electrohydraulic lithotripter (LithoTron Ultra; Phillips Medical Systems, Hamburg, Germany). 7 Pareek and associates reported stone-free rates of only 20% following SWL for lower pole renal calculi in patients with an SSD of 10 cm or greater, using a Medstone electrohydraulic lithotripter (Medstone, Inc., Aliso Viejo, CA). 8
The relationship between SSD and SWL success is less well established for ureteral stones. Given the anatomical location of the ureters and the angle of delivery of the shock wave, it would be expected that the SSD will be longer for ureteral stones relative to renal stones. Increased distance leads to attenuation of the shock wave, a feature exacerbated by increased amount of intra-abdominal fat. 8 Indeed Wiesenthal and coworkers confirmed a longer SSD for ureteral stones in their work analyzing predictive factors for SWL success, using a Phillips Lithotron Ultra electrohydraulic lithotripter (Phillips Medical Systems). 9 In addition, they reported that SSD was not an independent predicting factor for ureteral stones, a finding supported elsewhere. 9,10 Cho and colleagues recently reported a SSD of 10 cm as being optimum for SWL treatment success in ureteral stones. 11 They initially used an electroconductive lithotripter (EDAP Sonolith Praktis; Technomed, Lyon, France), switching to an electromagnetic generative lithotripter (Dornier Compact Delta II lithotripter; Dornier MedTech, Wessling, Germany) during the study period.
The outpatient treatment of ureteral stones using SWL brings significant potential benefit to obese patients, in particular reducing their exposure to general anesthetic procedures with resultant reduction in the associated risks. Ambulatory treatment, using sedo-analgesia, also has the benefit of reducing demand on in-patient surgical beds and surgical waiting times.
Objectives
To assess whether SWL can be used to achieve comparable stone-free rates in obese and nonobese populations with ureteral stones, using logistic regression to assess the impact of patient and stone factors on treatment success. To further assess for any association between SSD and treatment outcome using a matched-pair analysis approach.
Patients and Methods
Consecutive patients who had undergone SWL for solitary, radio-opaque upper ureteral calculi diagnosed on noncontrast computed tomography (NCCT) were selected from a prospectively-maintained database. Upper ureteral stones were defined as those located in the ureter superior to the upper border of the sacroiliac joint. Patients underwent treatment between August 2012 and February 2017. SSD was determined before treatment, using the method described by Pareek and colleagues: calculating a mean of three measurements at 0-, 45-, and 90-degrees from skin-to-stone center on the pretreatment NCCT. 8 Patients were treated using the Sonolith I-SYS electroconductive lithotripter (EDAP TMS), with a maximum focal depth of 17 cm.
Treatment is undertaken by standard operating procedure: before treatment, nursing staff undertake clinical assessment to determine if treatment is safe to go ahead. Appropriate analgesia is then administered (usually 100 mg Diclofenac per rectum). Immediately before treatment, a surgical pause is carried out to ensure that safety checks are complete.
Treatment is provided by radiographer with the aid of ultrasound and fluoroscopy for stone localization and monitoring. Nursing staff monitor the patient's comfort, blood pressure, heart rate, and oxygen saturation throughout treatment. For treatment of ureteral stones, power is started at 10%–25% for the first 300 shocks and then increased every 50 shocks in 5% increments to 100% or to the maximum power tolerated by the patient. The standard shock frequency is 2 Hz in our unit. Treatment is terminated when maximum energy is reached (1400 J), fragmentation of the stone is achieved (as assessed by radiographer performing treatment), or the patient is no longer able to tolerate the procedure.
Patients underwent a plain kidney, ureter, and bladder radiograph (KUB) at 2 weeks following treatment to assess initial response to treatment. NCCT is not routinely used in our center to assess treatment response to limit radiation exposure.
Overall treatment success was defined as the absence of stones on KUB or the presence of clinically insignificant residual fragments (3 mm or less in the absence of symptoms as per Cho and colleagues) 11 at 3 months following a completion of a course of SWL treatment. The number of SWL sessions required to produce an effective outcome was recorded. Treatment failure was defined as the persistence of fragments greater than 3 mm beyond 3 months, inability to tolerate SWL, or the need for intervention in the form of ureteroscopy. If calculi persisted at 2 weeks following the first session of SWL, patients were offered a second and then third session if required. If calculi persisted following a third treatment, patients were listed for ureteroscopy, as per the standard practice of our center.
Logistic regression was used to determine association of patient and stone factors with treatment failure. We then tested the association of SSD with treatment failure using a second statistical method: matched-pair analysis. This method was chosen in preference to propensity scoring as the latter is derived from logistic regression modeling. The cohort was divided into tertiles according to SSD, and matches were selected between the top and bottom tertiles.
Identification of pairs utilized six parameters employed in sequence: (1) age (<40, 40–59, ≥60 years); (2) gender; (3) maximum stone diameter (±2 mm); (4) stone density in HU (±250); (5) single or multiple sessions; and (6) presence or absence of a ureteral stent. These variables were selected for matching as they were significant in the multivariable logistic regression analysis or are reported as potential factors affecting the efficacy of SWL. 4,5,10,12 –15 Stone composition was not used as a matching variable as it was not available in all patients. When more than one match was identified, random numbers were assigned to rank potential matches.
Statistical analysis was undertaken using R and RStudio. 16,17 Regression analysis was undertaken using the finalfit package. 18 For matched pair analysis, difference between groups was assessed using McNemar's chi-squared test and paired Student's t-test.
Results
From a database of 2849 unique patients who underwent SWL (corresponding to 4240 treatment episodes), 397 patients were identified who had treatment of a single upper ureteral stone and who had complete follow-up data. Patient, stone, and outcome data of the 397 patients are summarized in Table 1.
Patient, Stone, and Treatment Information for the Total Cohort of 397 Individuals with Upper Ureteral Stones Treated by Extracorporeal Shockwave Lithotripsy
80.4% of patients were effectively treated by an SWL course.
IQR = interquartile range; SSD = skin-to-stone distance; SWL = extracorporeal shockwave lithotripsy.
Table 2 compares the outcomes following a treatment course (whether that involved a single session or multiple sessions). Age, SSD, stone side, stone diameter, and number of sessions were significantly associated with treatment failure on univariable analysis. Multiple sessions was the only factor significantly associated with treatment failure on multivariable analysis.
Univariable and Multivariable Logistic Regression Analysis of Factors Contributing to Treatment Failure in the 397 Patients with Upper Ureteral Stones Treated by Extracorporeal Shockwave Lithotripsy
Given the small number of individuals who underwent three sessions of treatment, they have been combined with the group who underwent two sessions. Significant results in bold (p ≤ 0.05). On univariable analysis, age, SSD, side, stone diameter, and multiple treatments were significantly associated with treatment failure. On multivariable analysis, only multiple treatments were significantly associated with treatment failure.
CI = confidence interval; OR = odds ratio; SD = standard deviation.
Given the dominance of multiple sessions in the model, and given that requirement for a second SWL session represents failure of the first session, we also undertook logistic regression considering treatment failure after a single treatment session (Supplementary Table S1). Age, stone side, stone diameter, and stone density were significantly associated with treatment failure on univariable analysis. Age, stone diameter, and stone density were significantly associated with treatment failure on multivariable analysis (Supplementary Table S2). The mean number of shocks delivered to the 283 patients who had an effective first treatment of SWL was lower than that delivered to the 114 patients whose first treatment was unsuccessful [mean (standard deviation [SD]) number shocks 3343 (1170) vs 3834 (959), p = 2.13e-5].
To increase the confidence in the assessment of association of SSD with SWL failure, we also used the matched-pair analysis statistical method. From a cohort of 141 patients with SSD ≥14 cm (top tertile SSD), and 174 patients with a SSD ≤12 cm (bottom tertile SSD), 66 matches were identified (132 patients). Table 3 illustrates patient and stone characteristics. Table 4 summarizes treatment outcomes following completion of the treatment course. There was no significant difference in treatment success between the two groups (p = 0.85). There was a significantly higher number of total shocks delivered to the cohort with SSD ≥14 cm (p = 0.02) and a significantly higher total energy used in treatment of that group (p = 0.03).
Patient and Stone Characteristics of the 132 Patients Identified as 66 Matched Pairs
Significant results in bold.
Patients with SSD ≥14 cm were matched with patients with SSD ≤12 cm. Matching criteria were: age, gender, stone diameter, stone density, single or multiple sessions, and presence or absence of a ureteral stent.
Summary of Treatment Outcomes of Patients Identified in 66 Matched Pairs
Significant results in bold (p < 0.05). There was no significant difference in treatment success between groups. Patients with SSD ≥14 cm received significantly more total shocks and energy than patients with SSD ≤12 cm.
We did not collect BMI routinely in patients undergoing SWL. To assess the relationship of BMI and SSD, we reviewed the computerized hospital records of the cohort of patients included in the matched-pair analysis. BMI was available for 63 of 132 individuals and was found to be significantly correlated with SSD (Pearson rho 0.64, p = 1.94e-8). This is illustrated by Figure 1.
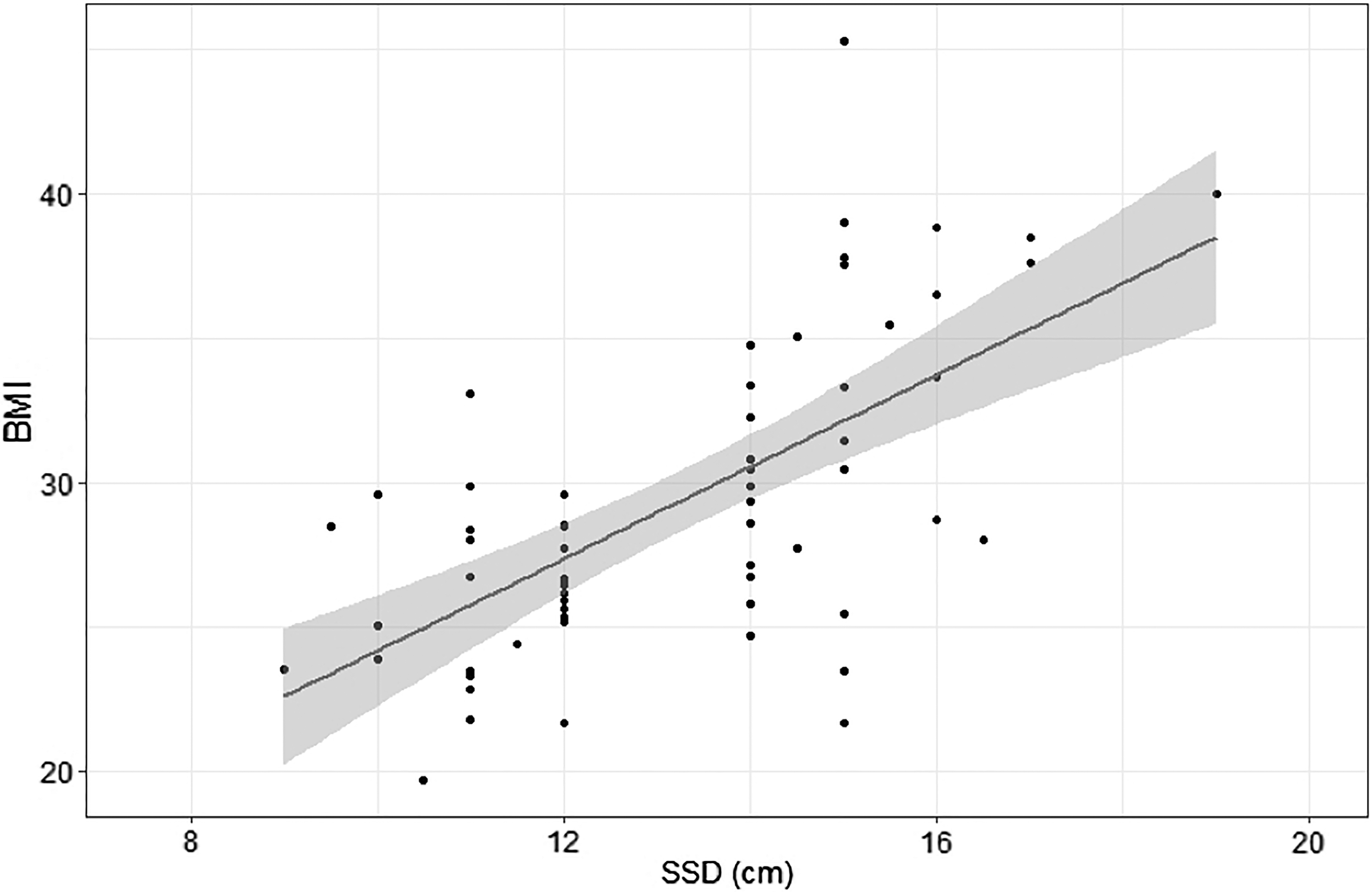
Relationship of SSD and BMI in 63 patients within the matched-pair cohort. BMI = body mass index; SSD = skin-to-stone distance.
Discussion
A wide range of patient and stone characteristics have been implicated as influencing factors in the effective outcome of SWL for treatment of upper ureteral stones. Efforts to establish the relative contributions of these characteristics toward the overall treatment success have yielded mixed and sometimes conflicting results. However, this remains a pertinent field of inquiry as patients could be more effectively triaged into the appropriate management pathway if there is better understanding of the relative contributions of such factors in the overall chance of treatment success. Within our institution, waiting times for SWL are considerably shorter than for surgical interventions, and effective triage of the appropriate patients toward SWL allows them earlier access to treatment.
The increased prevalence of obesity in the Western world, coupled with the higher propensity of these patients to form stones, means that endourologists frequently encounter obese patients. Aside from the physiologic challenges posed by such patients, obesity has been proposed to reduce the efficacy of SWL, rendering the localization and effective targeting of the stone more difficult.
BMI, when used as a proxy of obesity, has been found to serve as an independent predictor of SWL success. 8 However, BMI is unable to describe the variation in adipose tissue distribution. As a result, SSD has been described as a surrogate of obesity, encoding anatomical information relating to perirenal and ureteral adiposity. While our subgroup analysis showed that BMI was significantly correlated with SSD, the rho was only 0.64 and hence the two measurements are not perfect proxies of each other. This is similar to that observed by Cui and coworkers (r = 0.42). 19
SSD has been reported as outperforming BMI as an independent predictor of SWL failure in renal stones. 8 A number of subsequent studies have suggested an optimal range of SSD within which SWL success is maximal, for both ureteral and renal stones. In an analysis of 492 patients with upper ureteral stones, Cho and colleagues found 10 cm to represent an optimal SSD, with a significant decline in SWL success above and below this distance. 11 Ng and associates found a general decline in success above a SSD of 10 cm in a series of 94 patients with upper ureteral stones, with Wiesenthal and colleagues reporting a decrease in efficacy of SWL above an SSD of 11 cm for renal and ureteral stones. 9,20 In their series of 104 patients with ureteral stones, Müllhaupt and colleagues suggested an SSD of above 11.9 cm as a cutoff predicting treatment failure. 21
Although a large SSD is considered to be a significant adverse predictor of SWL outcome, we have not observed this to be the case at our center, a national referral unit. We are a dedicated stone center treating ∼1000 patients per year with lithotripsy, using a lithotripter with a focal depth of 17 cm. Consequently, patients with SSDs as much as 17 cm are routinely treated as first line with SWL at our institute.
The published SSD thresholds, reflecting relatively poor treatment outcomes for obese patients, did not correspond with the experience in our center. Given the large numbers of patients treated within our unit, logistic regression and a matched-pair analysis approach were chosen to utilize the power of the whole cohort. These data illustrate the utility of SWL in patients with higher SSD, achieving equivalent treatment outcomes to those with a lower SSD.
The European Association of Urology (EAU) guidelines on Urolithiasis describe comparable overall stone-free rates following ureteroscopy and SWL. 22 The guidelines also confirm an increased potential for complications with ureteroscopy, particularly with increasing grades of obesity. SWL performed under sedo-analgesia is a well-tolerated and safe procedure, and if it can be utilized effectively in selected obese patients, then the need for ureteroscopy may be reduced. This may benefit patients by reducing their exposure to the potential risks of a general anesthetic. In addition, there may be benefits in service provision, reducing the demand on day-case and in-patient theater resources.
It should be noted that these results are from a dedicated stone center, with a highly experienced clinical team. The provision of effective SWL in obese patients requires significant expertise in terms of patient positioning, stone targeting, and intrasessional adjustments. In addition, these results were achieved using a lithotripter with a focal depth of 17 cm, and therefore, they may not be applicable to all lithotripters on the market.
Two hertz is the standard frequency used in our center. However, fragmentation rates are noted to be enhanced by lower shock-wave delivery rates with the theoretical advantage of reducing renal injury. 23 1.5 Hz is recommended in the latest EAU guidelines on urolithiasis, although the evidence base is composed of meta-analyses. 24
Li and associates reported in meta-analysis of nine randomized controlled trials that while decreasing the frequency from 2 to 1 Hz increased overall success rates, the treatment duration of 1 Hz was greater than for 2 Hz (difference of 22.63 minutes, 95% confidence interval [CI]: 18.67–26.59, p < 0.001), and there was no difference in success rate for treatment of small stones (p = 0.16). 25 The same result was found in Kang and colleagues' meta-analysis. 26 Three hundred twenty-one patients (80.9%) in our series had stones ≤10 mm. While we have demonstrated effective stone treatment using 2 Hz, a reduction in the standard frequency will be an area of further study within our unit as it may offer additional benefits in terms of stone treatment outcomes.
Stone-free rates at 3 months after SWL have been reported as 68% in obese patients and between 80% and 85% in nonobese patients. 27 –30 The proposed mechanism for this discrepancy is the increase in intervening adipose tissue, leading to a higher SSD, which attenuates the shock waves. In addition, stone localization and treatment focusing are rendered more challenging in the obese patient. 31
Treatment success rates in our center for a course of SWL were 80.4% for whole cohort of 397 patients (and 71.2% at first SWL treatment). Treatment success of a course of SWL in the matched cohort was 77.3% and 74.2% for individuals with SSD ≤12 cm and SSD ≥14 cm, respectively. The 2007 EAU/American Urological Association (AUA) meta-analysis noted an 82% stone-free rate following SWL for stones in the proximal ureter (41 studies with 6428 patients). That is broken down further as 90% if stones are under 1 cm in diameter (14 studies and 886 patients) and 68% if the stone diameter was over 1 cm (11 studies and 293 patients). 32
Perks and colleagues studied outcomes for renal calculi following SWL in cohorts divided by SSD and stone density (HU). They described stone-free rates of 91% if SSD <9 cm and HU <900, but 41% if SD >9 cm and HU >900. 7 In our cohort, 320 patients (80.6%) had stones HU >900, and 112 patients (28.2%) had stones with diameter ≥1 cm; the stone-free rate in our cohort therefore compares favorably.
There was a considerable range in number of shocks delivered in our series. This likely reflects that this is a “real-life” series, and hence, number of shocks delivered was affected by patient tolerance and the treatment being terminated when effective (not being artificially prolonged to reach a preset total number of shocks). This is illustrated by the lower mean number of shocks delivered to the patients who had an effective first treatment vs the mean number of shocks delivered to the patients whose first treatment was unsuccessful.
It is interesting that in the matched pair analysis, there were significantly more shocks delivered to the ≥14 cm group, especially given that single/multiple sessions were included in matching criteria (and few required multiple sessions). We speculate that the larger interquartile range of shock number and energy for those individuals with a SSD ≤12 cm may reflect greater likelihood that a stone was treated more quickly without the requirement for a full treatment session, whereas the group with SSD ≥14 cm was more likely to require a full treatment session. While this is likely to be related to obesity, the treatment was tolerated well in this real-life situation and there was no observed difference in outcome.
Much of the criticism of SWL has focused on retreatment rates, with a need for repeated sessions to clear stones in comparison with a single ureteroscopy procedure. Most patients in this series required only a single session. In addition, there was no significant difference in treatment number between the groups (SSD ≤12 cm multiple session n = 25 vs SSD ≥14 cm multiple sessions n = 29, odds ratio [OR]: 1.54 [95% CI: 0.86–2.80], p = 0.25). These results compare favorably with published series, with good stone-treatment outcomes for both groups. It is also worth noting that the recent National Institute for Health and Care Excellence (NICE) economic analysis reported a National Health Service (NHS) reference cost of £452 for a single SWL session vs £2172 for ureteroscopy. 33
The correlation between SSD and BMI requires further evaluation, to consider the variations in adipose distribution between individuals. Neither parameter represents a perfect measure of obesity, and further work to model the relationship between SSD and BMI may have the benefit of improving the prediction of stone-free rates. We plan to include the prospective collection of BMI data in addition to SSD, as part of the standard data set for SWL patients. Given that this study is based on a retrospective analysis of prospectively collected data, there remains the potential for bias. However with eight variables in the multivariable regression model (Table 2), a model R 2 of 0.10, and significance level of 0.05, the post hoc power to detect association of variables with stone-free rate is 0.99. 34
Among the variables influencing treatment success, the type of lithotripter is likely to have an effect. Across the literature, the Dornier HM-3 was regarded as the reference standard with the highest reported stone-free rates; however, the newer generation machines have lower reported analgesia requirements and lower overall morbidity. 35 A 2007 study using an electroconductive lithotripter, the Sonolith Vision (EDAP TMS), reported stone-free rate which were comparable with those of the HM-3. 36 There are few data comparing results from different generating machines; however, Cho and colleagues reported that there was no statistically significant difference in treatment outcomes during the use of the electroconductive machine compared with the electromagnetic lithotripter. 11 This would be an interesting area for future study.
In summary, we have demonstrated in the largest single series reviewed in the literature so far that SWL can be deployed in the effective and efficient treatment of upper ureteral stones in obese patients, a group for whom general anesthetic procedures carry a higher risk of perioperative morbidity.
Footnotes
Acknowledgments
The authors thank the staff of the Scottish Lithotriptor Centre, Western General Hospital, Edinburgh for their assistance in data collection.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.