
Abstract
Objective:
In recent years, there has been increasing interest in the use of ultrasound guidance for endoscopic and percutaneous procedures. Kidney mockups could be used for training, however, available mockups are normally incompatible with ultrasound imaging. We developed a reproducible method to manufacture an ultrasound-compatible collecting system mockup that can be made at urology laboratories.
Methods:
Positive and negative molding methods were used. A three-dimensional (3D) digital model of a urinary collecting system and the overlying skin surface were segmented from computed tomography. A containment mold (negative) was made following the shape of the skin surface using 3D printing. A collecting system mold (positive) was also 3D printed, but made of a dissolvable material. The containment mold was filled with a gelatin formula with the collecting system mold submersed in situ within. After the gelatin solidified, a solution was used to dissolve the collecting system mold, but not the gelatin, leaving a cavity with the shape of the collecting system. The gelatin was extracted from the container mockup and the collecting system cavity was filled with water. The mockup was imaged with ultrasound to assess echogenicity and suitability for simulating ultrasound-guided procedures.
Results:
A clear shape corresponding to the collecting system was observed inside the gel structure. Structural integrity was maintained with no observable manufacturing marks or separation seams. Ultrasound images of the mockup demonstrated clear differentiation at the gelatin/water interface. A mock stone was placed in the collecting system and needle targeted to simulate percutaneous needle access.
Conclusion:
We developed a simple method to manufacture a personalized mockup of the renal collecting system of a patient that can be used for ultrasound-guided percutaneous needle access. Generic collecting system mockups can be used for training, and patient-specific models can be used to simulate and decide the best access path before a clinical case.
Introduction
Nephrolithiasis has been increasing in both incidence and prevalence, with women gradually bridging the gender gap 1 ; some estimate that almost one-third of a urology department's surgical workload is for the treatment of nephrolithiasis. 2,3 To date, most guidelines suggest percutaneous nephrolithotomy (PCNL) as the treatment of choice for larger stones (>2 cm). 4,5 An essential step of PCNL is achieving percutaneous access to the renal collecting system, which is most commonly performed under fluoroscopic guidance. A consequence of fluoroscopy is exposure of the patient and the operating team to ionizing radiation. Several studies have estimated the amount of radiation exposure and time of fluoroscopy, which, even in experienced hands, ranges from 2 to 8.9 minutes per case. 6 –11
The access can be achieved under ultrasound guidance, without radiation exposure. In expert hands, ultrasound-guided access has a high success rate with rare complications. 12 Several studies and series have described an entire PCNL operation under ultrasound guidance only, 13 –15 and Yu-Hsiang Yang and colleagues recently published the first meta-analysis for comparison of ultrasound-guided PCNL with fluoroscopy-guided PCNL, showing similar efficacy with a superior safety profile for the ultrasound-guided group. 16
The training required for achieving an adequate puncture time, using different techniques, varies between studies and ranges from 30 17 to 120 cases, 18 with ultrasound-guided PCNL having a lengthier learning curve. 12 For training, using ex vivo mockups crafted from fresh animal organs and tissues simulate the most realistic tissue properties, 19 however, these have limited utilization due to time and logistic constraints. Alternatively, synthetic mockups of the renal collecting system are typically limited to training under fluoroscopy guidance. 20
Commercial mockups are made of rubber-based materials that attenuate sound waves, thus rendering the mockups incompatible with the ultrasound. 21,22 Adams and colleagues published in 2017 a laboratory-reproducible ultrasound-compatible mockup of the kidney 23 that can be made using different materials to replicate the kidney tissue surrounding the collecting system. One of these materials is an agarose gel, which is ultrasound compatible. In their approach, the production materials and process included multiple steps, used two different three-dimensional (3D) printers with wax material for one part and ultraviolet curable photopolymer for another. Here, we present a simpler and less expensive option.
Our aim was to develop a training mockup for ultrasound-guided percutaneous renal access that can also be personalized to a specific patient. The mockup should be ultrasound-compatible, anatomically accurate, reproducible, inexpensive, and easy to make at a urology laboratory
Materials and Methods
Collecting system representation
An online, publicly available CT urography file was downloaded from the Cancer Imaging Archive. 24 A kidney with normal renal collecting system was chosen. Segmentation of the left-sided collecting system and the skin surface was done using the 3DSlicer free software. 25 The final result was an accurate 3D representation of both the collecting system and its exact relationship to the skin surface in a single file that was exported in a stereolithography (STL) format (Fig. 1a). FreeCAD software (The FreeCAD Team) 26 was used to convert the file into Standard for the Exchange of Product Data (STEP) format, which was used in CREO Parametric software (PTC, Needham, MA) to create a box (Fig. 1c) around the desired skin surface, which became the containment mold (negative). An oval-shaped shaft connecting the collecting system (positive) to the box was added to maintain the exact spatial relationship of the collecting system to the skin surface (Fig. 1b).

3D printing
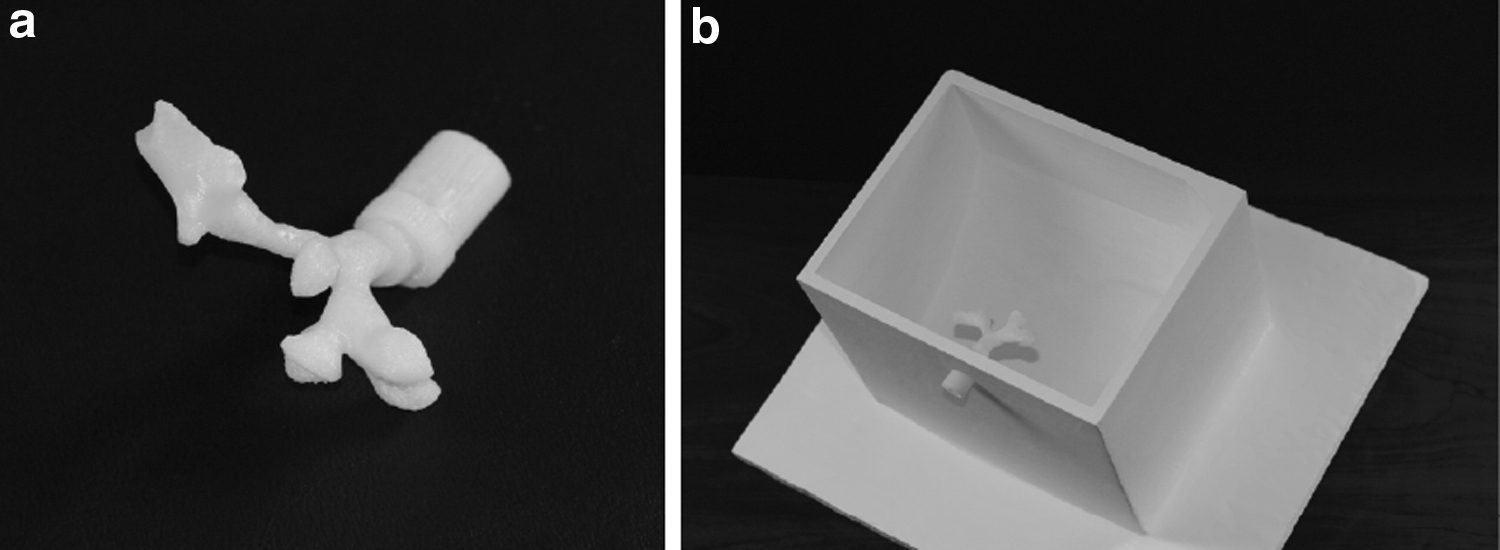
A MakerBot Replicator 2X printer (MakerBot Industries®) was used for 3D printing both the containment and collecting system molds. The containment mold was printed using an acrylonitrile butadiene styrene (ABS) filament (Fig. 2a). It was then mounted on a wooden board and painted to achieve water impermeability. The collecting system mold connected to the designed shaft was printed as a hollow object of a dissolvable filament (MakerBot Dissolvable Filament) (Fig. 2b). This filament is normally used in 3D printing as the secondary filament for support and bridging in complex builds, and is made of material that dissolves in limonene solution, a common citrus-based solvent. The collecting system mold shaft was assembled into its mounting hole of the containment model and filled with water to check watertight connections.
Gelatin mockup
Once the collecting system mold was secured in its designated location, gelatin was made using a formula of 300 bloom gelatin, glycerin, sorbitol, and water (at a ratio of 300:300:200:2500 g) at 55°C, and then poured into the negative containment mold. Subsequently, the mixture was cooled at room temperature. After the gelatin solidified, high-purity
The gelatin with the collecting system cavity was then extracted from the container mold. The cavity representing the collecting system was filled with water and imaged using an ultrasound probe (EUP-B512; Hitachi, Inc.). A mock stone was inserted to simulate imaging under ultrasound; percutaneous needle access was simulated using an 18-gauge percutaneous access needle (NaviGuide; Boston Scientific, Inc.) without a needle guide.
Results
Full versions of the printable files are available on the Johns Hopkins Urology Robotics Laboratory website (
Shown in Figure 1 are the software-based reconstruction steps of the collecting system and skin contour, Figure 2a shows the final 3D print of the collecting system mold, made from the special dissolvable filament, with the attached oval shaft that preserves the accurate positioning of the collecting system. Figure 2b shows the containment mold with the collecting system mold in place before gelatin was poured.
Once dissolved, the negative imprint of the mockup remained in the gelatin, the D-Limonene solution did not dissolve any of the gel elements, resulting in a clear-shaped cavity of the collecting system observed inside the gel structure. Structural integrity was preserved, and there were no observable manufacturing marks or separation seams (Fig. 3). The cavity representing the collecting system is accessible from the outside through what used to be the shaft of the construct, allowing for filling of water or insertion of stones in the collecting system.
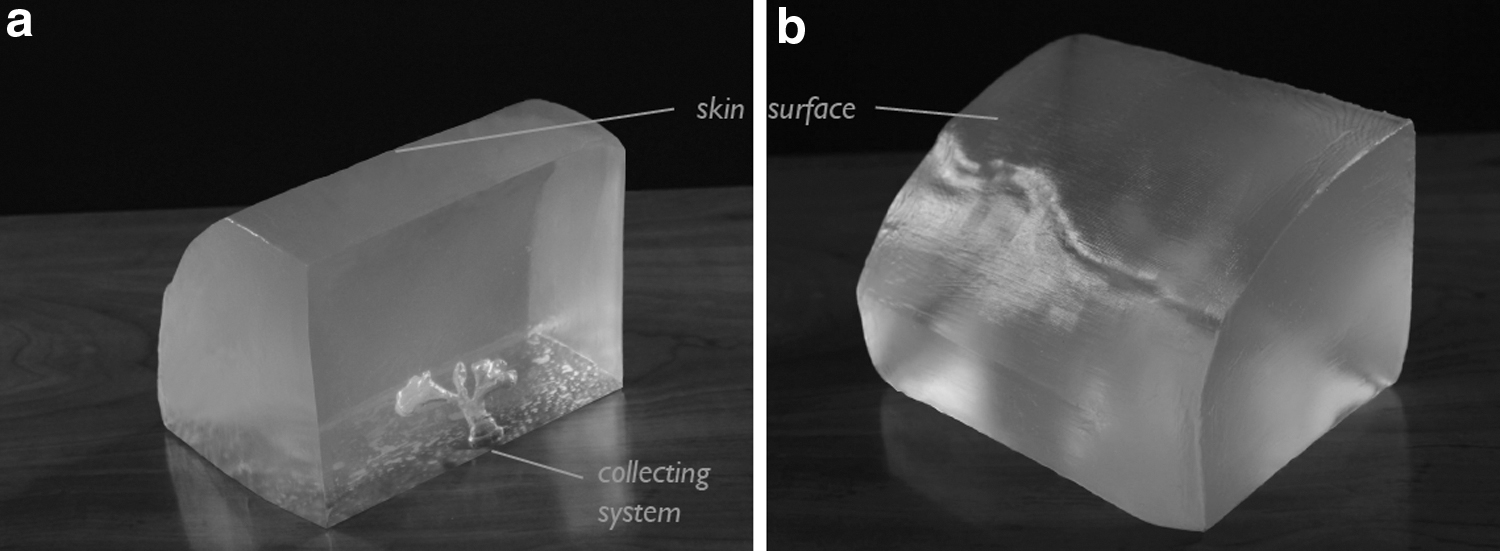
Gelatin mockup after dissolving the collecting system negative;
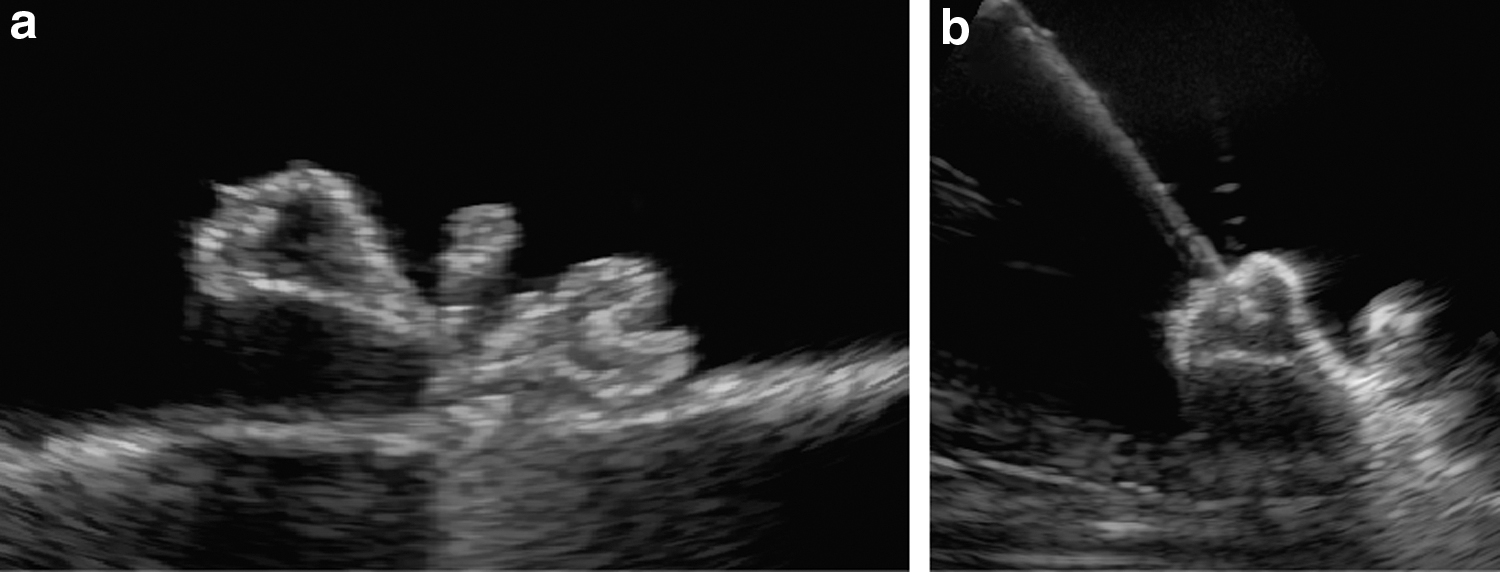
To assess the appearance and utility of the mockup in an ultrasound guidance system, an ultrasound probe and percutaneous access needle were used to simulate renal puncture. Ultrasound images of the mockup demonstrated clear differentiation at the gelatin/water interface (Fig. 4). A mock stone and needle were inserted into the cavity representing the collecting system to simulate percutaneous needle access, and both were visible under ultrasound.
The 3D printing and painting of the containment mold are a time-consuming step of the process, although most of the time is the 3D printing and waiting for the paint to dry, and the actual manual work is short. The time is ∼1 day in total. The production process of the rest of the mockup is 2 days; the 3D printing of the collecting system mold can be done in the same day as the containment mold, gel submersion takes 1 day, and dissolving the collecting system material is shortened to 1 to 2 days using the continuous pump.
The cost of the mockup varies depending mostly on the amount of gel used for the personalized model. The mockup shown in this article costs ∼$38. This includes 450 g of filament for the containment mold costing $21, the rest is for <10 g of dissolvable filament, 240 mL of
Discussion
Effectively achieving a percutaneous access to the renal collecting systems is one of the most important steps in PCNL surgery, and arguably the one requiring the most training and experience. Among the different methods for such access, there is a growing interest and literature support to the use of ultrasound guidance over fluoroscopy guidance. 16 However, teaching and training in ultrasound-guided access are currently limited by the lack of available mockups that accurately simulate the renal collecting system under ultrasound guidance. We have developed a novel method for quickly and inexpensively producing a 3D-printed mockup of an ultrasound-compatible collecting system using common laboratory materials, which can perfectly mirror a personalized patient body habitus and skin contour in relation to his/her collecting system.
This easy-to-manufacture gel mockup reproduces an exact cavity of the collecting system, shows great visibility under ultrasound imaging, and is based on a commonly available 3D printer in many laboratories nowadays. Once the staff is familiar with the technique, it is possible to repeatedly print a single standard training module or a specific patient's anatomy, which may be effective for preoperating planning in challenging cases. The surrounding gelatin mold can also be cast in any shape desired giving the ability to reproduce the relationship of the collecting system to the overlying skin exterior of the patient. The near-transparency of this gelatin-based model is particularly well suited for training purposes.
Typical PCNL training mockups are based on expensive simulators, 27,28 animal organs and tissues that do not reproduce the desired anatomy accurately and are not readily available, or specifically specialized fluoroscopy-guided trainers that can mimic the anatomy and be manufactured to any desired shape but expose the trainees to ionizing radiation and do not offer the option to train under ultrasound guidance. Even though the ease of fluoroscopy use compared with ultrasound may explain part of the widespread utilization of the technique, the lack of a reliable reproducible ultrasound-compatible renal collecting system mockup for training purposes may contribute to the slow adoption of ultrasound-guided access.
Limitations of this mockup are inherited from the gelatin base, which, even when using preservatives in the mixture, having an expiration date will not hold its integrity longer than several weeks. There may be a method to manufacture a more durable gelatin mixture, which may help to extend the usability of each mockup by using a mixture similar to that used in prostate mockups for ultrasound imaging, such as CIRS Model 053S. 29 A one-time consuming step in our process was the manufacturing of the containment mold based on accurate skin surface and preserving the relation to the collecting system; Nevertheless, we see in this an important step worthy of the time spent as it offers the ability to create not only personalized collecting system mockups but, for the first time, also personalized body habitus and skin contour characteristics for every patient to match his/her own collecting system. Once produced, the containment mold can be repeatedly used for identical models if we only wish to create training models.
This model's texture strength and mimicking real tissue have not been validated yet; this may be better addressed in the future and would be even more important in the case of an obese patient, but the model still offers a close resemblance to tissues for the training purpose it was manufactured for. Another consideration is that dissolving the collecting system mold special filament can prove to take several days if allowed to dissolve on its own with
This study has several implications for training and simulation. In any known mockup, after an initial needle puncture is performed, a visible delicate trace of the tract remains in the mold. In fluoroscopy training mockups, this proves to be a problem since the collecting system is filled with a radio-opaque solution that leaks into those tracts and clouds the image. Since our mockup is used for ultrasound training, the collecting system is filled with water and this leakage phenomenon has no effect on the image quality from the ultrasound transducer. Thus, the maximum number of punctures is only limited by the gelatin integrity, not by the opacity of the mold after multiple uses.
An important consideration for any proposed training mockup is its total cost of production and replacement; available mockups today reach costs of several thousand dollars, and up to $70,000 for some of the virtual reality simulators. 30 Laboratory-produced silicone-based fluoroscopy-only training mockups were described to cost $100 for the consumable parts only. 22 Our mockup has multiple advantages over commercially available trainers for percutaneous renal access. The 3D printer used was an entry-level, relatively inexpensive filament extruding printer that is typically available in most laboratories. The mockup was made of common laboratory materials; the total cost of the consumable materials was less than $20 per unit when identical mockups are produced, and even when fully personalizing it with the containment mold it costs less than $40.
Conclusion
We present a novel method to manufacture an accurate personalized renal collecting system mockup based on a gelatin mixture suitable for ultrasound imaging. This mockup is inexpensive to produce, may be manufactured in a common laboratory setting, and offers the flexibility to recreate any collecting system anatomy based on 3D printing. This provides a new training opportunity that may facilitate more widespread use of ultrasound guidance for percutaneous renal access and personalized patient mockups for practice before challenging cases.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.