
Abstract
Purpose:
To address the safety and feasibility of adjuvant single-dose upper urinary tract instillation of mitomycin (ASDM) immediately after therapeutic ureteroscopy for upper tract urothelial carcinoma (UTUC) and to compare urothelial (ipsilateral or bladder) recurrence rates in the ASDM group and controls.
Materials and Methods:
Between April 2015 and August 2018, 52 patients affected by UTUC were treated by endoscopic ablation, of whom 26 were selected for ASDM. Clinical and perioperative data and 30-day complications were recorded. Urothelial recurrence-free survival (URFS) was evaluated with second-look ureteroscopy (URS) and CT scan/URS every 6 months.
Results:
ASDM was administered through a Single-J (19/25, 76%) or a Double-J (6/25, 24%) in 25/26 (96%) patients. Median follow-up was 18 months (IQR 10–29). The urothelial recurrence rate was 23.5% and 55.5% in the ASDM group and controls, respectively (p = 0.086). Mean URFS was 28.8 months in the ASDM group vs 18.8 months in controls (log-rank p = 0.067). On multivariate Cox regression, ASDM was associated with a 7.7-fold lower risk of urothelial recurrence (HR = 0.13; 95% CI 0.03–0.65; p = 0.01). Clavien grade ≤II complications occurred in 32% (8/25) and 30.7% (8/26) of the ASDM and control group, respectively (p = 0.9). Two Clavien III complications occurred in the ASDM group: bladder hematuria after concomitant transurethral resection of bladder and obstructive kidney failure in a single-kidney patient.
Conclusions:
ASDM was well tolerated after therapeutic URS. It appears to reduce the risk of urothelial recurrence in patients affected by low-grade UTUC without bladder tumor. Therefore, its use should be evaluated.
Introduction
Upper tract urothelial carcinoma (UTUC) accounts for 5%–10% of urothelial carcinomas, with a rising incidence in recent decades. 1 Radical nephroureterectomy is considered the gold standard for treatment of UTUC. However, endoscopic management of noninvasive UTUC is increasingly considered a valuable option for selected patients, given that it reduces morbidity and the risk of dialysis and that it has been proven that survival outcomes are not adversely affected. Currently, the European Association of Urology (EAU) Guidelines recommend kidney-sparing surgery in elective cases of low-risk UTUC, such as noninvasive and unifocal disease, tumors less than 2 cm and low-grade tumors, and imperative cases. 1
Nevertheless, a recurrence may occur in up to 60% of these patients. 2 The implantation of floating neoplastic cells after endoscopic resection may explain the high risk of early recurrence, either in the bladder or in the upper urinary tract. 3 In this setting, the search for adjuvant treatments to reduce recurrences is of the utmost importance. Few studies have reported on the use of mitomycin C for UTUC, with variations in the form of application and the timing of the procedure, and its utility remains controversial. Therefore, the aims of this study were: (a) to address the safety and feasibility of adjuvant single-dose upper urinary tract instillation of mitomycin (ASDM) immediately after therapeutic ureteroscopy (URS) and (b) to assess urothelial recurrence rates, that is, ipsilateral local or bladder recurrences, in the ASDM group compared with a population treated conventionally.
Materials and Methods
Between 1 April 2015 and 31 August 2018, 52 patients affected by UTUC were treated by therapeutic URS with laser ablation. Although postoperative instillation of mitomycin has been proven to reduce the risk of recurrence in nonmuscle invasive bladder cancer, the Institutional Committee did not consider randomization ethics given the lack of phase 2 trials in the upper urinary tract; however, it validated the use of mitomycin in the upper tract based on proof of efficacy and tolerance in bladder. 4 –6 Patients with (a) concomitant multifocal or sessile/flat or >3 cm bladder lesion or (b) incomplete upper tract ablation were excluded from this prospective phase 2a trial. ASDM was offered to patients with a preoperative CT scan showing a clear diagnosis of papillary UTUCs with no signs of ≥T2 and in whom complete endoscopic ablation appeared technically feasible based on the shape, size, and number of lesions.
The controls were patients submitted to complete tumor ablation who (a) had no diagnosis of papillary lesions on CT, a suspicious imaging that required a URS or no recent (within 3 months) CT scan, (b) were intolerant to mitomycin, or (c) declined ASDM. The study was conducted in accordance with the Declaration of Helsinki (1964) and its later amendments. All patients signed an informed consent at the time of hospitalization. Ethics approval was obtained from the Institutional Board Committee of Fundació Puigvert (2014/17). To evaluate oncological outcomes, patients submitted to induction upper tract/intravesical instillations following URS were excluded from group comparison.
Technique
Second-generation cephalosporins or targeted antibiotics on the basis of urine culture were administered 30 minutes before the surgery.
An initial cystoscopy was conducted. If a vesical lesion was observed, a transurethral resection of bladder (TURB) was performed after URS.
The distal ureter was explored with semirigid ureteroscope while flexible ureteroscope (Storz Flex XC) was used in all cases for mid/upper ureter, renal pelvis, and calyx inspection. URS was usually performed according to the “no-touch technique” to increase the detection of erythematous lesions. 7 The urinary tract was explored with white light and Clara + Chroma/Spectra B technology (IMAGE1 S, Karl Storz, Tuttlingen, GE) to increase the diagnostic accuracy of the procedure. 8 Selective urine samples were collected for cytology. For each tumor, biopsies were carried out using a 2.2F Nitinol basket, 3F reusable biopsy forceps, and/or BIGopsy forceps (Cook, Bloomington, IN). 9 In cases of ablation with a flexible ureteroscope, a 12/14 Flexor Parallel (Cook) access sheath was inserted. The lesions were ablated with a holmium (10–12 Hz × 0.8–1.2 J) and/or thulium laser (setting: 18–22 W). At the end of the ablation, a retrograde pyelography was performed. Drainage consisted in an open-ended 6French ureteral catheter left in the pelvicalyceal system if no sign of ureteral damage was found; otherwise, at the surgeon's choice, a Double-J stent (7F, 26/28 cm) was placed.
Immediate postoperative upper urinary tract instillation of mitomycin
A single-dose upper urinary tract instillation of 40 mg/40 mL mitomycin C diluted in 20 mL saline solution was administered in 1 hour through a Single-J catheter. In cases of instillation through a bladder catheter and Double-J stent, 40 mg/40 mL mitomycin C diluted in 100 mL saline solution was administered in 1 hour. All the instillations were performed within 6 hours after the surgery. The ureteral catheter was removed on postoperative day 2, while the Double-J stent was removed after 7–14 days. Patients were usually discharged on postoperative day 2.
Endpoints
Clinical and perioperative data and 30-day complications (according to the Clavien/Dindo scale) were prospectively collected. 10 The primary endpoint was the safety and feasibility of ASDM. The secondary endpoint was urothelial recurrence, defined as a recurrence in the ipsilateral upper urinary tract and/or bladder. Follow-up consisted in a second-look URS within 3 months and CT scan/URS every 6 months for 2 years. Cystoscopies were scheduled according to the risk category of the patients. 1 Tumor grading was assessed according to the 2004 World Health Organization classification system.
Statistics
Absolute frequencies and percentages were used to describe the qualitative variables. Quantitative variables were described as mean, standard deviation (SD), median, and quartiles. Student's t-test (Mann–Whitney U-test if normality was not assumed) was used for comparison of quantitative variables. The chi-square test (Fisher test for frequencies <5) was employed for the comparison of categorical variables. A Kaplan–Meier curve was generated for cancer-specific survival outcomes.
Backward stepwise Cox regression analysis was performed for urothelial recurrence-free survival. p values <0.05 were considered statistically significant. The statistical packages R Studio V 3.1 and SPSS V 25 were used for the statistical analyses.
Results
Fifty-two patients met the inclusion criteria, 26 of whom were selected for ASDM. One (4%) patient was excluded from the study owing to urinary leakage at final pyelography, which contraindicated ASDM.
Overall, the mean age was 72.1 years, with a male-to-female ratio of 3:1. ASA score was I–II, III, IV in 26 (51%), 20 (39%), and 5 (10%) patients, respectively. ASDM and controls did not differ in terms of clinical characteristics (Table 1).
Demographic and Perioperative Data and Tumor Characteristics [Mean (SD) or n (%)]
UTUC = upper tract urothelial carcinoma.
The mean UTUC size was 15.1 mm (SD 11.3 mm). UTUCs were located in the calyx, pelvis, and ureter in 15 (29%), 19 (37%), and 25 (49%) cases, respectively; multifocality was present in 33%. For postoperative drainage, a Single-J stent was used in 19 cases (76%) and a Double-J stent in six (24%), comprising four patients in whom UTUC was located in the ureter and two in whom a grade I/II ureteral injury was observed after removal of the ureteral sheath.
Safety and tolerability
All patients allocated to ASDM received the entire dose of mitomycin and no side effects were reported during the instillation. No systemic side effects were observed. The overall complication rate in ASDM and controls was 40% and 30.7%, respectively (p > 0.7; Table 1). Complications with a Clavien grade ≤II comprised self-limiting hematuria (total/ASDM/controls: 16%/16%/15%), lumbar discomfort (8%/12%/4%), and infection (8%/8%/8%) (all p > 0.9). Two (4%) Clavien grade III complications were reported in the ASDM group. One patient with a functional solitary kidney and moderate chronic kidney disease experienced obstructive renal failure due to blood clots on postoperative day 2, which required substitution of the Single-J and a dialysis session. The second patient experienced postoperative severe hematuria as a complication of a concomitant TURB. Infectious complications were not related to a positive preoperative urine culture (7/52; 13.4%). During follow-up, one patient per group (4.7%) developed a ureteral stenosis.
Oncological outcomes
Postoperative follow-up is summarized in Figure 1. In the ASDM group, two patients (8%) were assigned to nephroureterectomy for high-grade or recurrent neoplasia. The overall survival rate was 90.6% (39/43), and the cancer-specific survival rate was 97.6% (42/43). Eight patients (18.6%) had maintenance treatment consisting in weekly upper tract instillations (mitomycin in five and BCG in three).
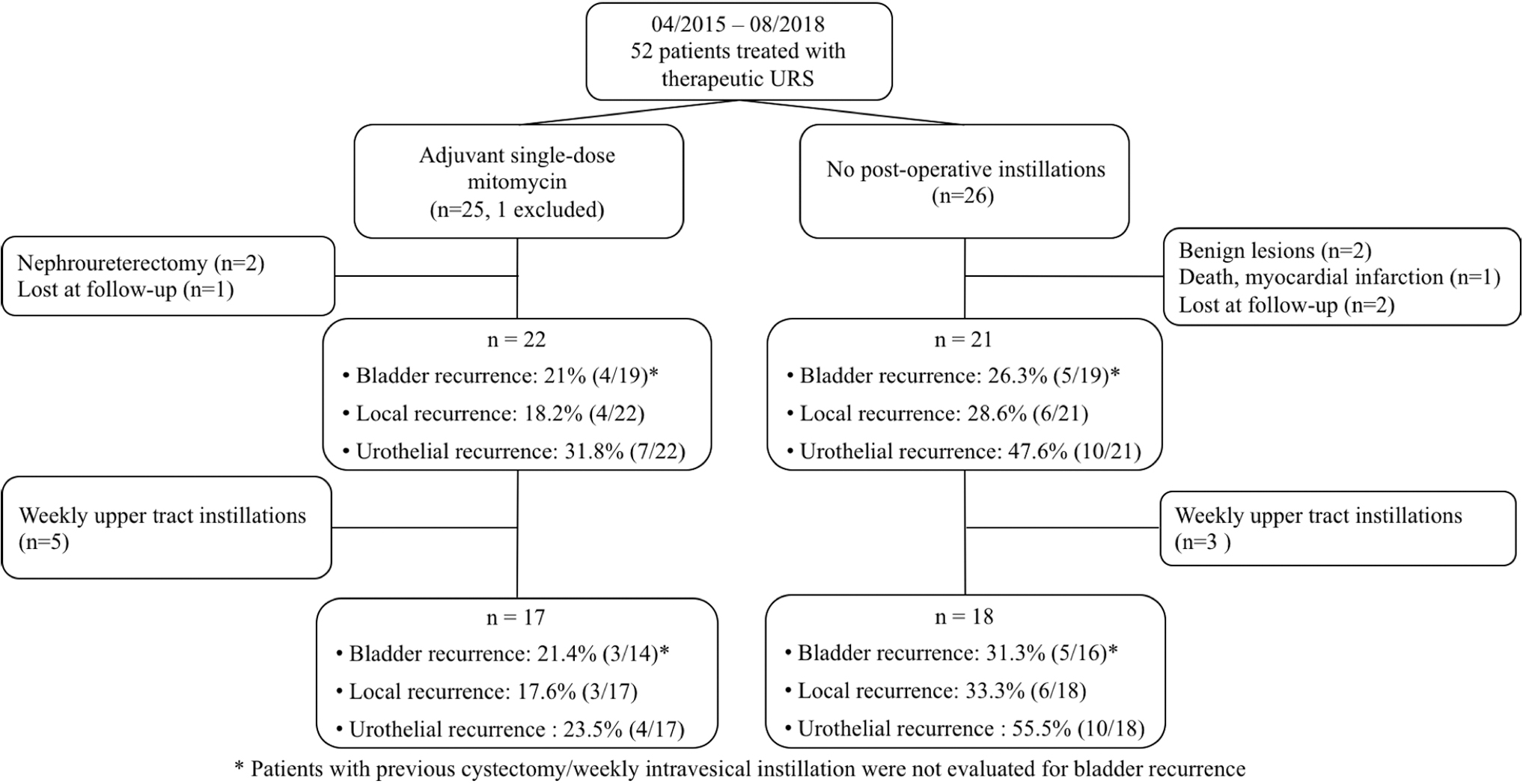
Flowchart for comparison of oncological outcomes between patients treated with and without ASDM. ASDM = adjuvant single-dose mitomycin C.
The oncological outcomes of ASDM were evaluated by comparing 17 ASDM patients (group A) with the 18 patients who did not receive any other adjuvant treatment after therapeutic URS (group B) (Fig. 1). Tumor characteristics are reported in Supplementary Table S1 (all p > 0.4). Median follow-up was 18 months (IQR 10–29). Urothelial recurrence occurred in 23.5% of patients in group A vs 55.5% in group B (p = 0.086) (Fig. 1).
In groups A and B respectively, urothelial recurrence consisted in upper tract recurrence in 17.6% (3/17) vs 33.3% (6/18) and bladder recurrence in 21.4% (3/14) vs 31.3% (5/16). Bladder and local recurrence were metachronous in two patients (11.8%) of group A and synchronous in one patient (5.5%) of group B.
Mean urothelial recurrence-free survival was 28.8 months in group A and 18.8 months in group B (log-rank p = 0.067; Fig. 2). Multivariate Cox regression included age, tumor grade, dimensions, multifocality, history of UTUC, UTUC risk stratification and primary/synchronous bladder tumor; the best model selected the variables age, tumor grade, ASDM, and primary/synchronous bladder tumor (-2log likelihood = 42.15; Hosmer/Lemeshow p = 0.25). The risk of urothelial recurrence was significantly higher in patients with high-grade UTUC (95% CI 2.19–127.67; HR = 16.7; p = 0.07) or previous or concomitant bladder tumor (95% CI 1.13–32.74; HR = 6.07; p = 0.036). ASDM reduced the risk of recurrence 7.7-fold (95% CI 0.03–0.65; HR = 0.13; p = 0.013) (Table 2).
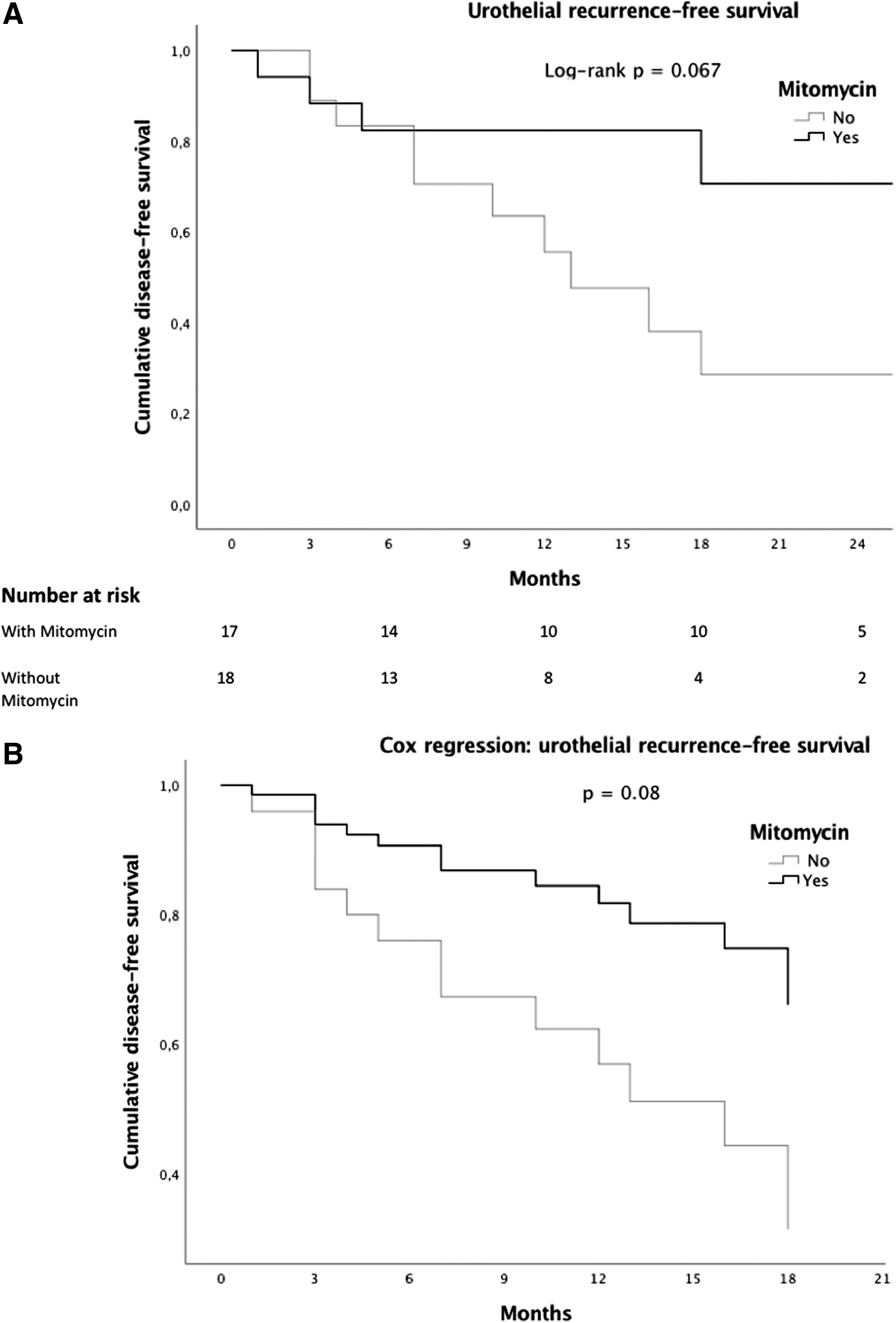
Urothelial recurrence-free survival (Kaplan–Meier and univariate Cox regression model) for patients submitted to mitomycin (group A) or treated conventionally (group B)
Univariate and Stepwise Backward Multivariate Cox Regression for Urothelial Recurrence
Discussion
In this study assessing immediate postoperative upper urinary tract instillation of mitomycin after endoscopic treatment of UTUC, it was found that ASDM had been feasible in >95% of the selected patients and resulted in a significant 50% relative reduction in urothelial recurrence. Adjuvant topical instillations may have a role in reducing UTUC recurrence, ultimately minimizing the need for nephroureterectomy and the number of endoscopic treatments per patient.
To the best of our knowledge, this is the first prospective nonrandomized trial on adjuvant prophylactic upper tract topical chemotherapy after endoscopic management of UTUC. The EAU recommendations, which state that upper urinary tract instillations are feasible, rely on noncomparative studies of induction protocols at least 14 days following URS. 1,11
The tolerability of upper tract induction and maintenance instillation of mitomycin C has been assessed in a noncomparative cohort. 12 Martínez-Piñeiro et al. reported a case of death due to mitomycin extravasation during upper tract instillations. 13 Based on this experience, we strongly recommend performing a pyelography at the end of URS and to exclude patients with contrast extravasation from ASDM. All of our patients completed the instillation without any related urinary symptoms or adverse events. The complication rate was 40% (10/25 patients), which may be considered relatively high. However, 8/10 patients experienced minor complications requiring analgesia/observation in 50% of cases and antibiotics in the remainder. No major complication was directly related to ASDM.
Two retrospective series have reported on the use of mitomycin after endoscopic management of UTUC, but timing, complications, and oncological outcomes were not specified. 2,14 Eastham and Keeley described no systemic side effects related to adjuvant treatment with mitomycin on postoperative days 1–3. 15,16 Aboumarzouk et al. reported that one of 19 patients (5%) did not tolerate an immediate postoperative instillation and that three (15.7%) had ureteral strictures. 17 In our series, one patient per group (2/43; 4.7%) developed a ureteral stenosis. Considering that a single dose of mitomycin was administered, we speculate that ureteral strictures are more likely related to the endoscopic procedure than to the endocavitary instillation.
The oncological outcomes of adjuvant mitomycin C after URS are controversial. Martínez-Piñeiro et al. reported a UTUC recurrence rate of 14% with mitomycin compared with 25% in unmatched controls who were characterized only by grade 1–2 tumors and a lower rate of T1 UTUC. 13 Keeley et al. found a higher rate of local recurrence in the mitomycin group (42% vs 18%) but the unequal pathological grade (grade 3: 52% vs 33%) and number of multifocal tumors (63% vs 33%) between the groups rendered the comparison heavily biased. 16 Cutress et al., in a retrospective case/control series, showed that adjuvant mitomycin did not modify the recurrence rate of UTUC. However, the dosage and timing of administration were not described and the number of instillations per patient was not clear (29 instillations for 18 patients). 18
In our study, bladder recurrence rates in the ASDM and non-ASDM groups were, respectively, 21.4% vs 31.3% (p = 0.7). ASDM was associated with an absolute reduction in local recurrence of 15% [3/17 (17.6%) in group A vs 6/18 (33.3%) in group B; p = 0.4]. In group A, two high-grade UTUC recurred and one low-grade tumor progressed to become high grade. In group B, all six local recurrences occurred within the control visit at 1 year, and four (66.6%) were low-grade UTUC. The timing of recurrence differed between the groups, with a mean delay of 10 months in group A (28.8 months vs 18.8 months in group B). On multivariate analysis, the risk of urothelial recurrence was reduced 7.7-fold with ASDM (HR = 0.13; p = 0.013). This result suggested that early instillation of mitomycin C after therapeutic URS reduces the risk of urothelial recurrence in patients affected by low-grade UTUC without primary/synchronous bladder tumor.
This study has some limitations. No randomization was performed. The two populations compared are relatively small. ASDM was delivered through either a Single-J or a Double-J stent. As described in Table 3, the type of delivery, timing and dosage of mitomycin C differ widely among studies reporting upper tract mitomycin instillations for UTUC. Upper urinary tract topical chemotherapy using a Double-J stent is not recommended. 15 We considered not to modify the indication of urinary diversion after URS to give a treatment, which although beneficial was yet to be established. Moreover, when using a Double-J, mitomycin was diluted in 140 mL to guarantee a proper vesicoureteral reflux in ureters, which were just dilated, assuming the risk of an excessive dilution of mytomicin. 19 However, it must be highlighted that in group A, 2/3 (66.6%) patients in whom a Double-J was used suffered a local recurrence compared with only 1/13 (7.7%) when using a Single-J. As the implantation of neoplastic floating cells has been shown to take place early after endoscopic resection, we believe that ASDM should be performed as soon as possible after surgery. 3,20 Regarding the formulation of mitomycin C, no studies have succeeded in establishing a standard dose; a phase 3 trial analyzing an induction plus maintenance protocol for the administration of MitoGel™ is ongoing (NCT02793128). Another limitation is represented by the low number of events, which increases the risk of overfitting in the multivariate Cox regression analysis. In this respect, however, it is to be noted that the 1-to-10 rule (minimum of 10 outcome events per predictor variable) has been proven to be too conservative. 21 Based on the results of the present study, a randomized controlled trial is starting.
Comparison of Studies Reporting Upper Tract Mitomycin Instillations for Upper Tract Urothelial Carcinoma
N/A = not available.
Conclusions
Adjuvant single-dose upper urinary tract instillation of mitomycin C within 6 hours after therapeutic URS was well tolerated. It appeared to reduce the risk of urothelial recurrence in patients affected by low-grade UTUC without bladder tumor. Therefore, its use should be tested on a randomized controlled trial.
Footnotes
Author Contributions
Study design: Breda A, Territo A, Gallioli A, Palou J; Data collection: Gallioli A, Vila Reyes H, Regis F, Subiela JD; Manuscript writing: Gallioli A, Boissier R, and Territo A; Article editing: Gaya JM, Sanguedolce F, Territo A, and Subiela JD.
Acknowledgment
The authors like to thank Cristina Esquinas Lopez for statistical revision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.