
Abstract
Purpose:
To compare the efficacy of the erector spinae plane block (ESPB) and conventional analgesia (CA) in pain management after percutaneous nephrolithotomy (PCNL).
Materials and Methods:
After obtaining the approval of the institutional ethics committee and patients' written informed consent, 60 cases ages 18 to 65 years, with the status of American Society of Anesthesia I/II and body mass index of 18.5 to 30, were included in the study. The patients were randomized to receive ESPB or CA by a computer-based list.
Results:
The demographic parameters were similar in both groups. Regarding the visual analog scale (VAS) score assessment, the patients in the ESPB group described statistically less pain according to the total score and evaluations at hours 0, 1, 6, and 24 (p = 0.001, 0.009, <0.001, and 0.014, respectively). The time to first rescue analgesic was longer in the ESPB group compared with the CA group (172.33 ± 180.5 minutes vs 84.33 ± 71.12 minutes), which was statistically significant (p = 0.016). The use of tramadol and paracetamol was less in the ESPB group (60 ± 72.3 mg vs 120 ± 55 mg and 1.8 ± 0.76 g vs 3.2 ± 0.99 g, respectively). (p = 0.001 and <0.001, respectively).
Conclusions:
ESPB is a safe technique that provides effective postoperative analgesia in patients undergoing PCNL. ESPB decreases the postoperative VAS score, prolongs the salvage analgesia time, and reduces the need for paracetamol and tramadol use compared with general anesthesia with CA.
Introduction
Percutaneous nephrolithotomy (PCNL) is the gold standard surgical method for the treatment of renal stones greater than 2 cm. However, the discomfort, stress, and pain caused by the nephrostomy tube after surgery increase the importance of postoperative analgesic treatment. It has been suggested that post-PCNL pain associated with the nephrostomy tube may result from structures beyond the skin puncture site, such as the kidney capsule. 1
Anatomical studies have shown that the main sources of acute pain after PCNL are visceral pain from the kidneys and ureters and somatic pain from the incision site. Kidney pain is carried from the T10-L1 spinal cord nerves, and ureteral pain from the T10-L2 spinal cord nerves. 2 In addition, PCNL incision and tract are usually made from the subcostal or 10th and 11th intercostal spaces, and the cutaneous innervation of this region is mostly carried by T10–11. 2
Intravenous nonsteroidal anti-inflammatory drugs and opioids are widely used to manage postoperative pain. However, this type of pain has a limited response to oral and intravenous treatments and is often underestimated. 3 Furthermore, these drugs used in analgesic therapy have many side effects and their use in patients with potential kidney problems requires caution. 4,5 As an alternative method, well-established anatomical nerve pathways make regional nerve blocks, such as intercostal nerve block (ICNB) and paravertebral nerve block (PVB) preferable in the treatment of postoperative pain. Since PCNL is performed unilaterally, it is recommended to block the sensation of pain arising from the kidney and surgical area through regional anesthesia. 6 However, the effectiveness of nerve blocks has not yet been clearly demonstrated. 7
First described by Forero in 2016 for the treatment of thoracic neuropathic pain, the erector spinae plane block (ESPB) is based on the principle of blocking the dorsal and ventral roots of the thoracic abdominal spinal nerves by applying an ultrasound-guided local anesthetic between the erector spinae muscle and the transverse process. 8,9 ESPB is known to provide effective analgesia in thoracic and abdominal surgery. 10,11
Our hypothesis is that ultrasound-guided ESPB can provide sufficient analgesia in the postoperative period when applied at the level of T8. To the best of our knowledge, there is no other randomized controlled trial investigating the use of ESPB in PCNL surgery in the English-indexed literature. The aim of this randomized controlled study was to compare the efficacy of ESPB and conventional analgesia (CA) in pain management after PCNL.
Materials and Methods
Study design
The study protocol was examined by the Erzincan Binali Yıldırım University Ethics Committee and approved with the protocol number 9048. A prospective, single-center, randomized controlled follow-up study was performed with patients who underwent PCNL with or without ESPB for the treatment of renal stones between January 2017 and March 2019. A total of 60 patients were included in the study. The patients were randomly assigned to the ESPB (n = 30) and CA (n = 30) groups. Randomization was performed using a computer-based list before the operation.
The demographic data of the patients (age, sex, weight, height, and body mass index), laboratory results (hematocrit, creatinine, and estimated glomerular filtration rate), operation time, hospitalization time, postoperative analgesia usage (tramadol and paracetamol use and time to first rescue analgesic), and the degree of postoperative pain (visual analog scale [VAS] scores) were noted. A decrease in the pain score was the primary endpoint of our study. Our secondary endpoints were the determination of time to first rescue analgesic, rates of tramadol and paracetamol use, length of hospital stay, and postoperative stone-free rates.
Patients older than 18 years, who had >2 cm kidney stones, and were scheduled to undergo PCNL were included in the study. The exclusion criteria were a body mass index of >30, contraindication for ESPB, substance abuse, allergy to local anesthetics, cardiovascular, respiratory, neurologic, or metabolic diseases, severe coagulopathy, complex stones requiring more than two renal access punctures, musculoskeletal deformities, low cognitive function that would make VAS score difficult to assess, missing data, and patient withdrawal from the study.
Operation technique
All surgical operations were performed under general anesthesia. A ureteral catheter was placed in the lithotomy position for retrograde pyelography. Subsequently, the patients were placed in the prone position and underwent ultrasound-guided ESPB before needle entry for the first renal puncture. Following these steps, percutaneous renal access was achieved with the triangulation technique under C-arm fluoroscopic guidance. The tract was dilated to 30F with a high-pressure balloon dilator (NephroMax™; Microvasive Boston Scientific Corporation, Natick, MA). The stones were fragmented with a pneumatic lithotripter and removed using stone clamps. A nephrostomy tube was placed in the system after the operation. A ureteral Double-J stent or catheter was not applied during the operation.
ESPB technique
All ESPB procedures were undertaken by an anesthesiologist experienced in regional blocks (F.A.). A 12 MHz linear probe was used for ultrasound-guided ESPB (GE Medical Systems, Milwaukee, USA.) performed at the T8 level. The transverse process was detected by sliding the transducer 3 to 4 cm laterally from the midline, and after identification of the transverse process, a 22-gauge insulated echogenic needle (Stimuplex; B. Braun Medical, Inc., Bethlehem, PA) was used to administer 20 cc of 0.5% bupivacaine (Bustesin; Vem Drug Company, Istanbul, Turkey) between the erector spine muscle and the transverse process. The distribution of bupivacaine was observed on ultrasound (Fig. 1).

Ultrasound image showing the transverse process of T7–T8, needle, and spread of local anesthetic.
Pain assessment
All patients and an independent observer who was responsible for follow-up during 24 postoperative hours were blinded to the randomization groups. The degree of pain was assessed using VAS on a scale of 0 indicating no pain and 10 indicating the most severe pain ever experienced. The VAS scores were recorded at hours 0, 1, 6, 12, and 24 by an independent observer in accordance with the patients' reports. Rescue analgesia was performed with intravenous tramadol in cases where the VAS score was ≥4. Total analgesic use was noted.
On the first postoperative day, the urethral catheter was removed and hemogram was performed. The amount of hematocrit decrease compared with the preoperative analysis was noted. On the second postoperative day, the nephrostomy tube was extracted if the patient tolerated the blockage of nephrostomy tube drainage. The patients were discharged on the postoperative second day. If any adverse event was observed, such as infection, bleeding, and nephrostomy blockage intolerance, hospital stay was prolonged.
Statistical analysis
For the statistical analysis, IBM SPSS Statistics version 25 Windows package program was used. The compliance of data to the normal distribution curve was evaluated by the Shapiro–Wilk test. Student's t-test or the Mann–Whitney U-test was used to compare the continuous variables between the two groups, depending on whether the statistical hypotheses were fulfilled. The chi-square test was used to compare categorical variables between the groups. p < 0.05 was accepted as statistically significant.
Results
The patient demographics, stone size, puncture site, surgical outcome, operation time, and length of hospital stay are given in Tables 1 and 2. There was no statistically significant difference between the two groups regarding patient demographics, stone characteristics, operation outcome, operation time, and hospital stay.
Patient Characteristics
ASA = American Society of Anesthesiologists; CA = conventional analgesia; eGFR = estimated glomerular filtration rate; ESPB = erector spinae plane block; SD = standard deviation.
Surgical and Postoperative Data
Table 3 presents the patients' pain scores at hours 0, 1, 6, 12, and 24, time to first rescue analgesic, total tramadol use, and total paracetamol use. When the pain scores of the two groups were compared, it was seen that the patients in the ESPB group described statistically less pain according to the total score and at hours 0, 1, 6, and 24 (p = 0.001, 0.009, <0.001, and 0.014, respectively). Although the 12th-hour VAS score was higher in the CA group, there was no statistically significant difference between the two groups (p = 0.36) (Fig. 2).
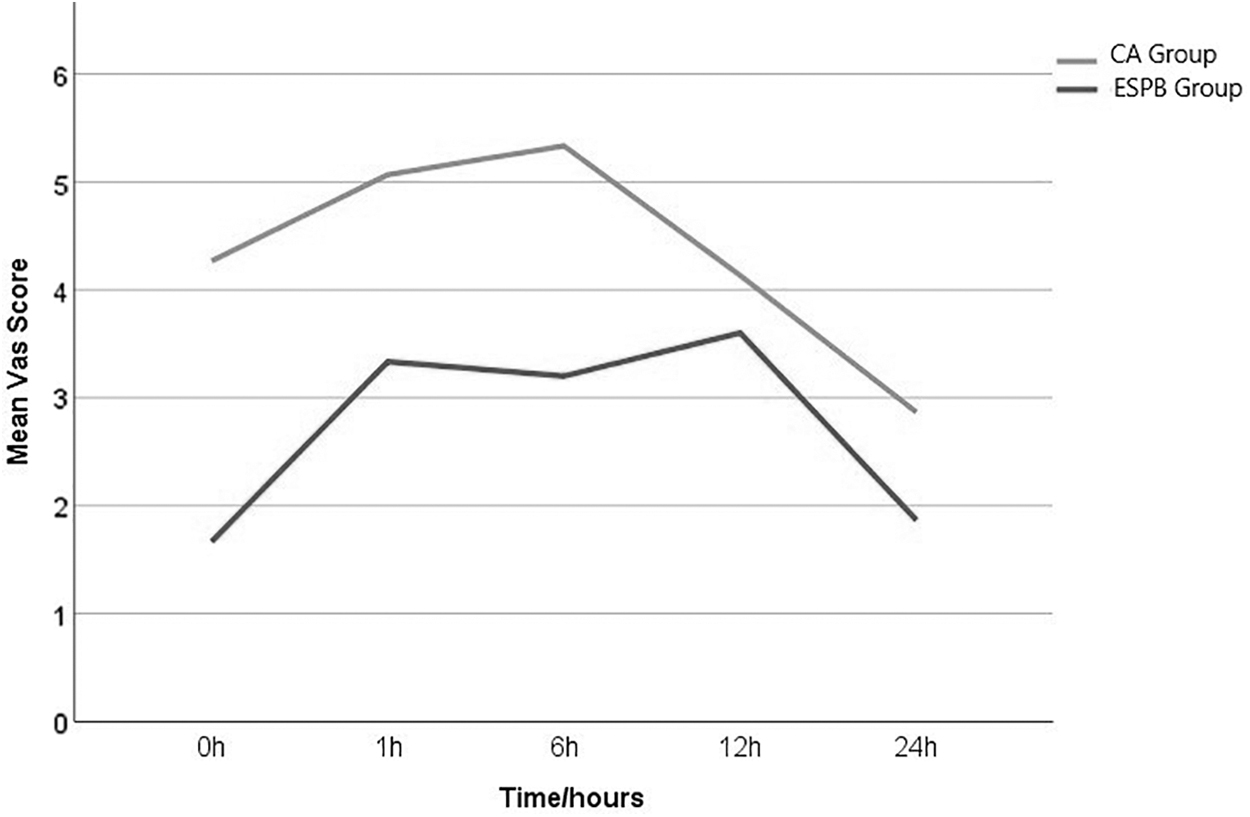
Changes in the postoperative VAS scores. CA = conventional analgesia; ESPB = erector spinae plane block; VAS = visual analog scale.
Postoperative Analgesia and Visual Analog Scale Scores
Bold values indicate statistical significance.
NSAIDs = nonsteroidal anti-inflammatory drugs; VAS = visual analog scale.
The first rescue analgesic was applied after 172.33 ± 180.5 minutes in the ESPB group and after 84.33 ± 71.12 minutes in the CA group, which was statistically significant (p = 0.016). The use of tramadol and paracetamol was less in the ESPB group (60 ± 72.3 mg vs 120 ± 55 mg and 1.8 ± 0.76 g vs 3.2 ± 0.99 g, respectively), with a statistically significant difference between the two groups (p = 0.001 and <0.001, respectively).
Discussion
In this study, we found that in patients undergoing PCNL due to large kidney stones, ultrasound-guided ESPB reduced the VAS score and analgesic therapy requirement, compared with the patients who did not receive any additional regional anesthesia.
PCNL is a gold standard surgical procedure commonly used for the treatment of kidney stones larger than 2 cm. Although the skin incision made during the operation is small, postoperative pain is severe. It is desirable to reduce the use of postoperative analgesic therapies that may have nephrotoxic effects because most patients with a history of renal stones have impaired renal function or are potential candidates for the loss of renal function. Regional methods provide effective analgesia in the postoperative period systemic side effects of narcotic analgesics such as nausea, bowel dysfunction, and return to regular diet. The use of spinal, epidural, and local anesthesia around the nephrostomy tube, PVB, ICNB, and ESPB for PCNL has been reported in the literature.
ESPB is a more superficial block than other block methods. The most significant advantage of ESPB block is its simplicity and safety over other PVB and ICNB. In ESPB, the local anesthetic is directly applied between the transverse process and the erector spinae muscle, and the point of application can be easily determined on ultrasound. The transverse process is a bonny tissue and the sono-anatomy of this target point is easily recognizable. Also, there are no structures at risk of needle injury in the adjacent tissues. Important structures (such as main vessels, pleura, or medulla), whose injury can cause serious complications, are far from the target of blockage. 8 The PVB technique is particularly challenging, as the needle is placed in immediate proximity to the pleura, which increases the risk of pleural puncture. 12 Hematoma, pneumothorax, and nerve injury are the possible complications of PVB regarding its invasive nature. The target point of PVB is close to the neuraxial space and this makes it a more invasive block than ESPB. In ICNB, a local anesthetic agent is injected between the internal intercostal muscle and innermost intercostal muscle. The posterior border of this space is made by innermost internal intercostal muscle and this soft structure would be mistakenly passed by the needle. So, pneumothorax and intravascular injections are the possible complications of ICNB. 13 In addition, the local anesthetic agent only spreads into the related intercostal space and to achieve adequate postoperative analgesia, mostly multilevel intercostal blocks are required. 14 By the illumination of this anatomical and technical knowledge, ESPB is considered to have lower risk of pneumothorax than PVB and ICNB. By the way, head-to-head comparison of ESPB, PVB, and ICNB with regard to technical simplicity and safety is lacking in the literature.
Following its first description in 2016, 8 ESPB has been used in many procedures, such as thoracic and abdominal surgery, thoracic neuropathic pain management, bariatric surgery, 15 thoracotomy, 10 and hip surgery. 9 The use of ESPB in kidney pain is only encountered in case reports. First, Aydin et al. reported their initial experience with ESPB in renal colic and concluded that it was an alternative safe way of relieving uncontrolled acute pain in patients with renal colic. 16 Following these authors, Kim et al. described the use of ESPB to reduce postoperative pain in PCNL and suggested that it might be a good alternative for postoperative analgesia. 7 However, to our knowledge, there is no randomized controlled clinical trial of ESPB in PCNL cases in the current literature.
In a cadaver study, the distribution of the local anesthetic agents was found to be similar between ESPB and PVB. 17 With the illumination of the abovementioned study and due to the rarity of research on ESPB, we compared our findings with PVB, which is anatomically the closest block method to ESPB.
In this study, we found the VAS scores of the ESPB group to be significantly lower than the CA group at hours 0, 1, 6, and 24 (p = 0.001, 0.009, <0.001, and 0.014, respectively). Similar results were observed by Hatipoglu and colleagues, who compared PVB and intravenous tramadol for postoperative pain management and reported that the VAS score was significantly lower in the PVB group (p < 0.05). 18 In another study investigating the efficacy of PVB in PCNL, the authors observed lower VAS scores in the PVB group during the study period. 19
Although the 12th-hour VAS score of the ESPB group was lower than that of the CA group, there was no statistically significant difference between the two groups (p = 0.36). Since the surgical procedures were completed from 12:00 to 16:00 and the 12th-hour VAS score was evaluated between 00:00 and 04:00, this evaluation mostly corresponds to the hours when the patients were asleep. We consider that the patients aroused from sleep may have reported less pain than they felt or they were not able to fully cooperate. A similar situation was observed in a study by Jonnavithula and coworkers, in which despite the significant difference at the 4th, 8th, 12th, and 20th hours, there was no significant difference in pain scores for the 16th hour. 13
There is no homogeneity in the literature in terms of analgesic treatments used in the postoperative period. The most commonly used analgesic agents are diclofenac, 20,21 tramadol, 6,14 and pethidine. 22 In our study, we used tramadol as the rescue analgesic, but to reduce the total opioid use, we performed secondary treatment with paracetamol when analgesia did not have a sufficient effect. The combination of these two drugs is especially encountered in palliative care and postoperative pain management in cancer patients. 23 –25
To avoid numerical differences with the literature, we discussed the differences between the two groups as percentages and compared the values with the findings of previous reports. As a result, we found that in the ESPB group, the total tramadol use was decreased by 50% (60 ± 72.3 mg vs 120 ± 55 mg) and the total paracetamol use was decreased by 43.75% (1.8 ± 0.76 g vs 3.2 ± 0.99 g), compared with the CA group. Hatipoglu and coworkers examined the effect of PVB on PCNL and observed a 45.5% decrease in tramadol use (77.7 ± 60.5 mg vs 142.5 ± 61.0 mg, p < 0.001). 18 In another study, the postoperative analgesic effect of ICNB was investigated, and tramadol use in the ICNB group was 51.2%, which was lower compared with the CA group (97.5 ± 39.5 mg vs 199.7 ± 77.6 mg, p = 0.000). 14 Although our results did not numerically overlap, the percentages were consistent with the existing literature.
In our study, the ESPB group required rescue analgesia later than the CA group (172.33 ± 180.5 minutes vs 84.33 ± 71.12 minutes, p = 0.016). Borle et al. performed PVB in patients who underwent PCNL and found that the time to first postoperative analgesic requirement in the PVB group (120 minutes; range 30–570 minutes) was longer than in the control group (30 minutes; range 0–180 minutes) (p = 0.0000). 19 Ak and associates showed comparable results in their study, in which they performed multiple-level PVB in patients who underwent PCNL. They reported the time to rescue analgesic as 94.2 to 24.1 minutes in the multiple-level PVB group and 48.3 to 17.4 minutes in the control group. This earlier application of rescue analgesia compared with our study may be due to the previous authors' use of patient-controlled analgesia in their study. 21 Our results were consistent with the literature in terms of the prolonged time to rescue analgesic in the ESPB group.
This study has several limitations, such as the single-centered design and relatively small number of patients. Furthermore, we did not have a sham block group due to ethical considerations. Another limitation was that there was a significant difference in terms of sex distribution between the groups. Theoretically, gender-related differences can effect pain perception. Finally, all of our patients underwent general anesthesia before the ESPB procedure; thus, we did not perform a pinprick test to evaluate the actual area of analgesia. Further multicenter studies with a larger number of patients are required.
Conclusions
The results of this study show that ESPB is a safe technique that provides effective postoperative analgesia in patients undergoing PCNL. ESPB decreases the postoperative VAS score, prolongs the time to rescue analgesia, and reduces paracetamol and tramadol use without any side effects compared with general anesthesia with CA.
Footnotes
Acknowledgment
We thank Dr. Akif Erbin for his help on the revision.
Ethical Statement
This study was approved by the Institutional Ethics Committee of Erzincan Binali Yildirim University Medical Faculty with the IRB number of 9048.
Authors' Contributions
M.H.G. and A.E.: Protocol/project development, data collection or management, data analysis, and article writing/editing. F.A.: Data collection or management.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.