
Abstract
Objective:
To describe a novel technique of ureteral reimplantation through robotic nontransecting side-to-side anastomosis. Although the standard approach to ureteroneocystostomy has a high rate of success, it involves transection of the ureter that may impair vascularity and contribute to recurrent strictures. Our method seeks to maximally preserve distal ureteral blood flow that may reduce this risk.
Materials and Methods:
We retrospectively reviewed a multi-institutional ureteral reconstruction database to identify patients who underwent this operation between 2014 and 2018, analyzing perioperative and postoperative outcomes.
Results:
Our technique was utilized in 16 patients across three U.S. academic institutions. Median operative time and estimated blood loss were 178 minutes (interquartile range [IQR] 150–204) and 50 mL (IQR 38–100), respectively. The median length of stay was 1 day (IQR 1–2). No intraoperative complications or postoperative complications with Clavien score ≥3 were reported. Postoperatively, 15 of 16 (93.8%) patients reported clinical improvement in flank pain, and all patients who underwent follow-up imaging had radiographic improvement with decrease in hydronephrosis at a median follow-up of 12.5 months.
Conclusions:
Ureteral reimplantation through a robotic nontransecting side-to-side anastomosis is a feasible and effective operation for distal ureteral stricture that may have advantages over the standard of care transecting ureteroneocystostomy.
Introduction
Ureteral strictures are commonly caused by ischemia, impacted ureteral calculi, history of ureteral instrumentation, iatrogenic injury, pelvic trauma, periureteral fibrosis, radiation, tuberculous infection, and other causes. 1,2 Although some strictures can be successfully managed by endoscopic intervention, surgical repair is often necessary for long-term relief of obstruction.
For distal ureteral strictures, the gold standard surgical approach is ureteroneocystostomy (i.e., ureteral reimplant). Although this technique is associated with high success rates ranging from 70% to 100%, 2 some patients develop recurrent strictures. Ureteroneocystostomy involves transection and mobilization of the distal ureter, which may impair the vascularity of the anastomosis and contribute to the development of these recurrent strictures.
In addition, reimplantation at another site on the bladder can make future ureteroscopy more challenging because the new ureteral orifice is no longer located in its orthotopic position and can be difficult to locate or access.
We report our multi-institutional outcomes for a novel technique of robotic nontransecting side-to-side ureteral anastomosis in patients with benign distal ureteral strictures. This method seeks to improve upon the standard ureteroneocystostomy by limiting ureteral dissection and mobilization and eliminating ureteral transection to maximally preserve distal ureteral vascularity. In addition, the technique leaves the native ureteral orifice in its anatomic position that can simplify access to the upper tract for future endoscopic procedures.
Although a similar technique has been described in the pediatric urology literature for surgical repair of primary obstructive megaureter, 3,4 to our knowledge, this approach has not been described in the adult literature nor for the indication of distal ureteral stricture.
Technique
The key surgical steps to robotic nontransecting side-to-side anastomosis are highlighted in Supplementary Video S1.
Setup and port placement
The patient is positioned in a modified flank position and secured to the operating table. Four robotic ports are placed on the side of the abdomen corresponding to the patient's stricture, and an additional periumbilical assistant port is placed. A Foley catheter (18F or larger) is placed on the field and the robot is docked.
Ureteral identification
The surgery begins by identifying the strictured ureter. A vessel loop may be placed around the ureter to help aid dissection without directly grasping the ureter. Since the blood supply of the distal ureter originates from a posterolateral direction, the distal ureter is not mobilized in this area to keep its native blood supply intact. Intravenous indocyanine green may be administered to help identify vascularity.
Bladder mobilization
The bladder is freed from its attachments to the anterior abdominal wall and pelvis until adequately mobilized to allow for a tension-free anastomosis. If needed, a psoas hitch or Boari flap can be performed in the usual manner.
Ureterotomy and cystotomy
A longitudinal ureterotomy is made proximal to the ureteral stricture while leaving the distal strictured ureter in situ. A long ureterotomy (∼3–4 cm) is preferred to ensure a widely patent anastomosis. A cystotomy is made in the posterolateral portion of the bladder in preparation for anastomosis to the ureterotomy.
Anastomosis and stent placement
Anastomosis is performed using a running 4-0 absorbable suture. First, one wall of the anastomosis is completed in a running manner. Next, a Double-J stent is placed in retrograde manner into the ureterotomy and across the anastomosis. Once the stent is in position, the remaining portion of the side-to-side anastomosis is closed. When completed, the configuration of the ureter is as appears in Figure 1.
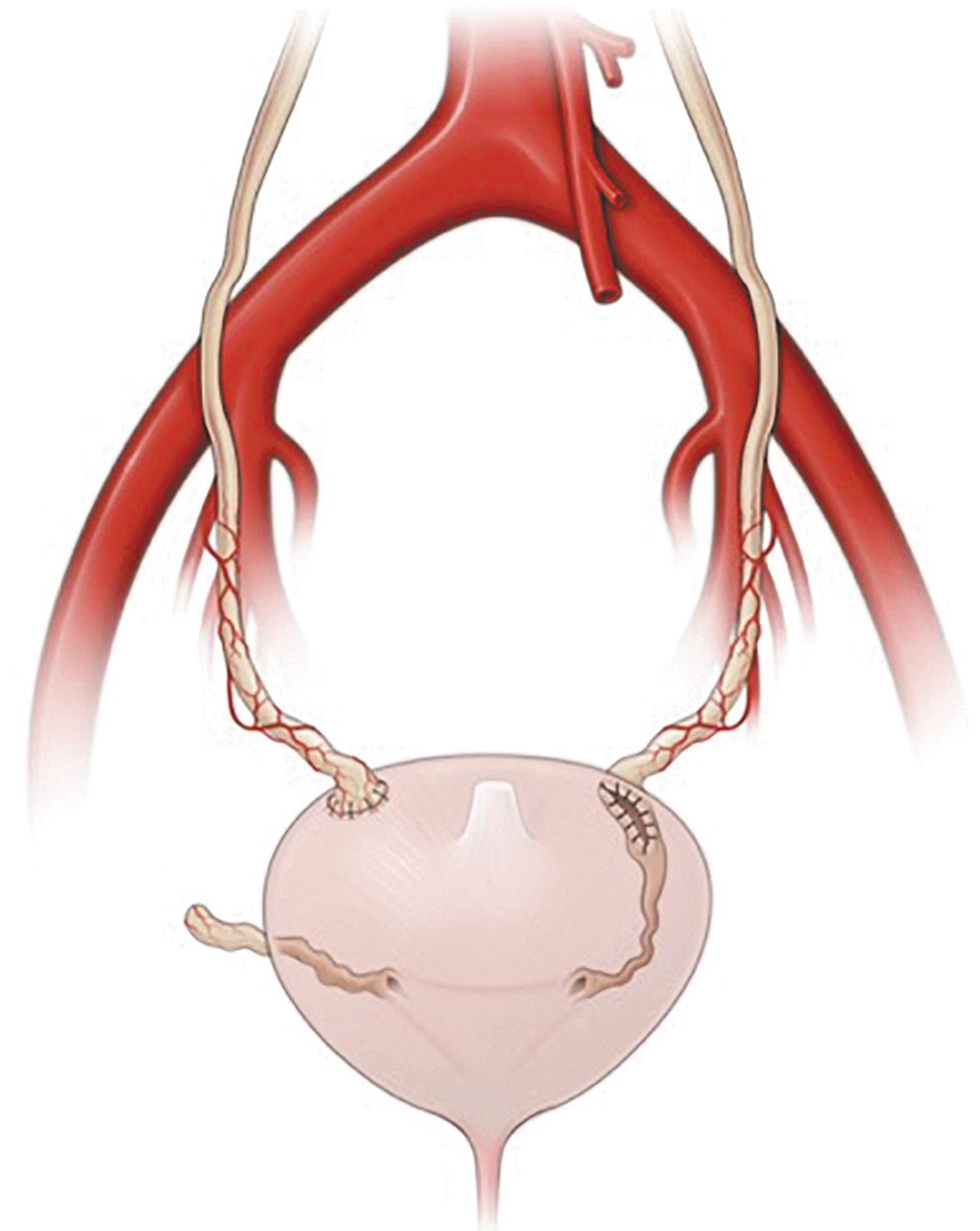
A standard transecting ureteroneocystotomy with end-to-end anastomosis is depicted on the right ureter, whereas a nontransecting ureteral reimplant with side-to-side anastomosis is depicted on the left ureter.
Final steps
After the anastomosis is complete, the bladder is filled with ∼200 mL of normal saline to ensure a water tight closure. A 15F Blake drain is placed into the pelvis through an inferior robotic port site, and the previously placed Foley catheter (18F or larger) remains in the bladder.
Postoperative care
The pelvic drain is removed before discharge when drain fluid creatinine level is consistent with serum. The Foley catheter is removed after 7–10 days if there is no leak on cystogram. The Double-J ureteral stent is removed after 3–4 weeks. Patients undergo imaging 1 month after stent removal through renal ultrasonography or mercapto acetyl tri glycine renal scan at the discretion of the primary surgeon. Success is defined as improved parameters clinically and on postoperative imaging.
Materials and Methods
A multi-institutional ureteral reconstruction database was reviewed to identify patients with distal ureteral stricture who underwent ureteral reimplantation through a nontransecting side-to-side anastomosis across three U.S. academic institutions between 2014 and 2018.
All patients who underwent the operation were included in the analysis. Data that were captured included patient preoperative information (age, gender, body mass index (BMI), etiology of stricture, stricture length, and prior stricture management), intraoperative data (operative time, blood loss, and length of stay), and postoperative outcomes (complications, symptom improvement, and absence of hydronephrosis on imaging).
Results
The results are summarized in Table 1. Among our three institutions, 16 patients underwent a robotic ureteral reimplant through nontransecting side-to-side anastomosis between 2014 and 2018. Eight patients were male and eight patients were female. The median age and BMI were found to be 64 years (interquartile range [IQR] 51–68) and 29 kg/m2 (IQR 27–34), respectively. The median stricture length for all treated patients was 3 cm (IQR 2.5–3.3). Etiology for the stricture in our cohort included iatrogenic injury (44%), impacted ureteral calculus (19%), pelvic radiation (13%), endometriosis (6%), and idiopathic (19%). This distribution of stricture etiology is similar to that which is reported in the literature. 2 Five of 16 (31%) patients had undergone prior endoscopic management for their stricture, all of whom underwent ureteral balloon dilation.
Summary of Results
BMI, body mass index; IQR = interquartile range.
All patients underwent a robot-assisted operation without conversion to open surgery. The median operative time and estimated blood loss were 178 minutes (IQR 150–204) and 50 mL (IQR 38–100), respectively. Median length of stay was 1 day (IQR 1–2).
No intraoperative complications or postoperative complications with Clavien score ≥3 were reported. A total of 15 of 16 (93.8%) patients were found to have clinical success defined as absence of flank pain, and 100% of patients with follow-up imaging had radiographic improvement at a median follow-up time of 12.5 months (IQR 4–23).
Discussion
Ureteral reimplantation through a nontransecting side-to-side anastomosis is a feasible and effective operation for distal ureteral stricture.
Patients in our study tolerated the surgery well with low volume blood loss, short hospital stay, and good clinical and radiographic outcomes. We hypothesize that our technique is less disruptive to the blood flow of the distal ureter and allows for the creation of a widely patent anastomosis, which theoretically should result in a lower risk of recurrent stricture. Although our series has only followed patients for a median of 12.5 months, we have not yet encountered a recurrent stricture utilizing this technique.
Our technique also has the added benefit of keeping the ureteral orifice in its orthotopic position, which can aid with access to the upper tract if endoscopic intervention is required in the future. For example, a ureteroscope can be advanced into the native orifice and can dilate the stricture in the distal ureter if needed. Alternatively, a sensor wire can be passed through the native orifice to locate the new anastomotic orifice, which can then be cannulated.
This technique is also particularly helpful in the setting of severe distal ureteral fibrosis, which can be encountered in patients who have undergone prior ureteral surgery or in patients with radiation-induced strictures. Rather than mobilizing the fibrotic distal ureter, the dissection takes place more proximally in an area with better defined dissection planes.
One key limitation of this procedure is the inability to create a nonrefluxing anastomosis in the standard tunneled manner. However, if a nonrefluxing anastomosis is desired, detrusor flaps can be developed and laid around the ureter just proximal to the anastomosis in a 5:1 ratio of flap length to ureteral diameter. In our series of 16 patients, 1 had a “clinical failure” caused by persistent bothersome flank pain during urination consistent with reflux pain, a complaint that could have been possibly addressed by adding this step to our technique. As we gain more experience with this operation, we can determine whether this step needs to be utilized more frequently.
Another limitation of this procedure is interference by the uterus and ovaries if present. Further research with larger cohorts, longer follow-up, and prospective design is also required to better determine whether long-term outcomes of this operation are similar or improved compared with a standard transecting ureteroneocystostomy.
Conclusions
We demonstrate that ureteral reimplantation through a nontransecting side-to-side anastomosis appears to be an effective tool in the armamentarium to manage distal ureteral strictures.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Video S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.