
Abstract
Introduction:
Herein we provide the first report regarding in vivo porcine renal forniceal, papillary, and infundibular blood flow at the urothelial level using a novel ureteroscopic Doppler transducer.
Materials and Methods:
Nephroureteroscopy was performed on 11 female Yorkshire pigs to map the forniceal, papillary, and infundibular blood flow. A Doppler transducer was mounted to a 3F 120 cm catheter; the probe was passed through the working channel of a flexible ureteroscope. Blood flow was categorized from 0 (no flow) to 3 (highest flow) based on auditory intensity. At each site, a holmium laser probe was activated until it penetrated ∼1 cm into each of the examined areas; bleeding times were recorded.
Results:
The frequency of the Doppler transducer signal was proportional to the blood velocity within the vessel with expected increased bleeding times confirmed after puncture with a holmium laser. Analysis demonstrated that the 6 o'clock position of the fornix had significantly greater blood flow than any other forniceal location (p < 0.001). The center of each papilla had the least blood flow (p < 0.001). Blood flow was significantly higher at the infundibular level compared with the caliceal fornices at all locations (anterior, posterior, upper pole, midkidney, and lower pole) (p < 0.001).
Conclusions:
In a porcine model, a miniaturized Doppler ultrasound probe used during ureteroscopy demonstrated that the renal papilla had the least amount of blood flow whereas the infundibula had the highest blood flow. These data may serve to inform site selection during percutaneous nephrostomy placement.
Introduction
Ultrasonography (US) has allowed urologists to safely and reliably evaluate the kidney and associated structures since its introduction to urology in the late 1960s. 1 Although providing an accurate and noninvasive approach for imaging the kidney, US also offers urologists a cost-effective intraoperative tool capable of detecting renal perfusion. 1 –3 Specifically, the introduction of Doppler US modalities has made it possible to accurately detect the direction, volume, and velocity of renal blood flow. 4,5
Owing to their physical design, currently employed US probes in urology are limited to surface evaluation of the kidney and its vasculature as they must be positioned either on the patient or atop the renal capsular surface during a laparoscopic procedure. To date, an intrarenal US analysis of renal perfusion patterns has not been done because of a lack of an appropriately sized Doppler US probe. We hypothesize that an analysis of this nature would potentially be of value for determining the best site for creating an endoscopically guided percutaneous nephrostomy tract.
In this study, we describe the use of a diminutive novel Doppler transducer that was passed through the working channel of a flexible ureteroscope. The objective of the study is to test the ability of the transducer to map blood flow patterns for the first time at the level of the caliceal fornix, caliceal papilla, and infundibulum throughout the porcine kidney.
Materials and Methods
Study design
After obtaining Institutional Animal Care and Use Committee approval, a nonsurvival study was performed on 11 female Yorkshire pigs ranging from 16.1 to 22.0 kg in weight. All pigs were anesthetized according to standard procedure. Cystoscopy was performed, a guidewire was passed under fluoroscopic guidance into each kidney, and a retrograde pyelogram was performed (Fig. 1). A 14F ureteral access sheath was then advanced into the renal pelvis.

Retrograde pyelogram in a porcine kidney.
A Doppler transducer (Vascular Technology Incorporated, Nashua, NH) mounted to a catheter with an overall diameter of 3F and a working length of 120 cm was coupled with a 20 pulsed Doppler transceiver unit (Fig. 2A). The catheter was passed through the working channel of a flexible ureteroscope (Fig. 2B). Saline irrigation at a pressure of 150 mm Hg was maintained using a manual hand-pump irrigation device through the unoccupied channel of the dual lumen ureteroscope. The flexible ureteroscope was passed into the kidney and the Doppler transducer was used to map renal blood flow within each of the anterior and posterior upper, middle, and lower calices (Fig. 2C). For the first six pigs, the probe was placed at the 12 o'clock, 9 o'clock, 3 o'clock, and 6 o'clock positions along the fornix then at the center of the papilla. The spatial orientation of these clock positions was confirmed both using fluoroscopy and by performing an air pyelogram allowing for differentiation of the anterior and posterior locations of the collecting system. For the subsequent five pigs, flow was recorded at the level of the upper, middle, and lower infundibula. Based on the intensity of the Doppler auditory signal, each reading was categorized as 0 (no flow), 1 (low flow), 2 (moderate flow), or 3 (high flow); this was done by the ureteroscopist and three additional assessors as previously described by Badani and colleagues. 6 After determining the flow at each of the aforementioned forniceal and papillary locations, a 365 μm holmium laser fiber (1 Joule and 10 Hz) was placed through the irrigation channel and fired to a depth of 1 cm into each of the assessed areas. The bleeding time for each site was recorded up to 5 minutes.

Statistical analysis
For statistical analyses, Doppler flow readings were grouped into low flow (0–1) and high flow (2–3). These binary unpaired categorical data were analyzed using a chi-squared test, and pairwise comparison was performed with Bonferroni correction to control for multiple comparisons.
Results
An audible signal was produced when the Doppler transducer was placed upon a vessel within which there was flow; vessels up to a depth of 1 cm could be detected. Distinctive tonal patterns were produced that were indicative of the flow pattern in terms of velocity vs time. A three-dimensional (3D) model of the porcine kidney was created utilizing 3D Slicer, an open source software available through the National Institutes of Health. By pooling the data, composite images were created that depict the average flow patterns observed with the Doppler transducer in the anterior and posterior calices, respectively (Fig. 3).
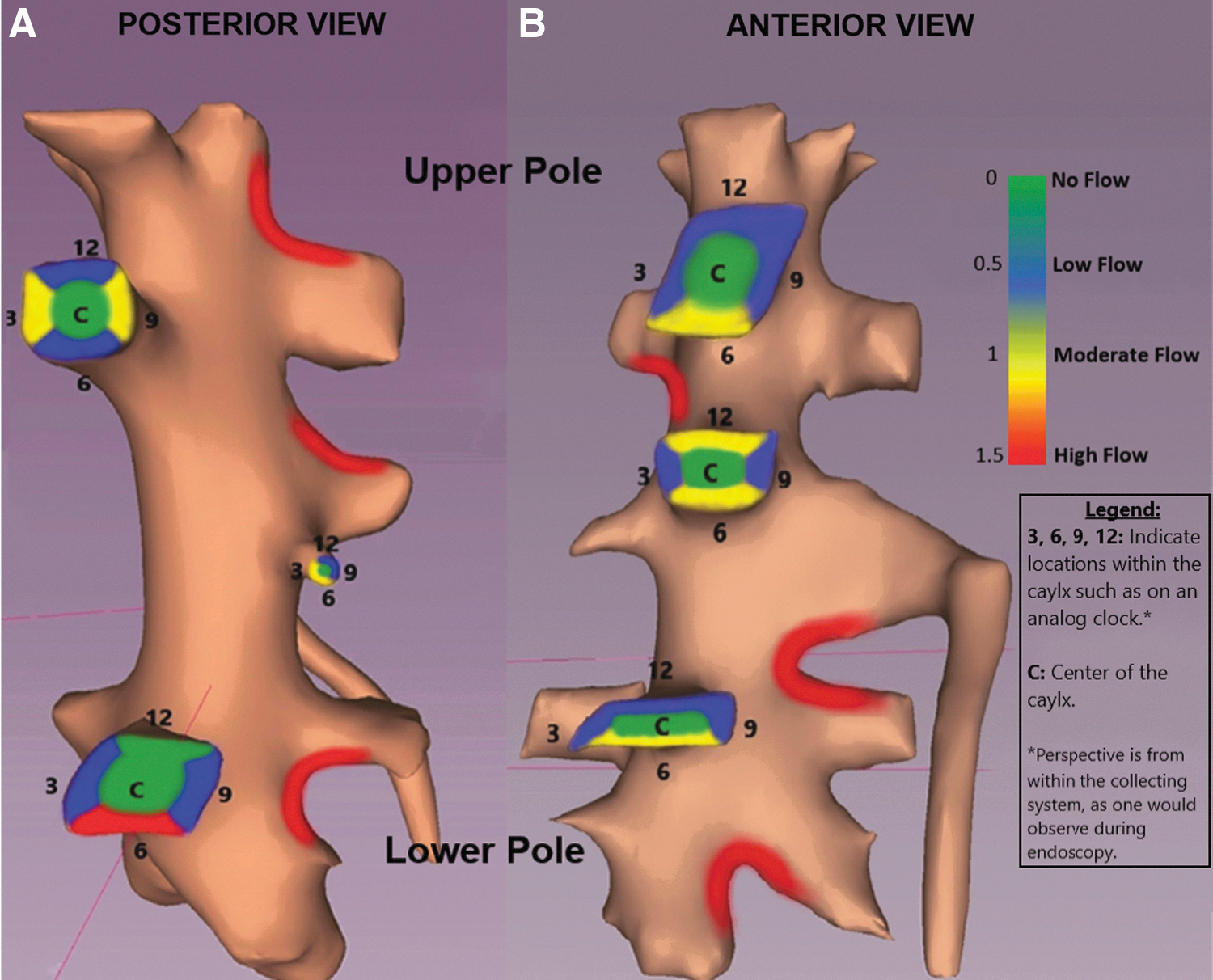
The frequency (i.e., pitch) of the signal was found to be proportional to flow velocity within the vessel as the Doppler-mapped flow regions did have the expected increased bleeding times after a 1 cm puncture through the urothelium and into the renal parenchyma with an activated Holmium laser fiber. For the “no flow” regions, the average bleeding time was 49.75 seconds as compared with the regions with flow, which had an average bleeding time of 116.95 seconds (p = 0.01).
Comparisons of Doppler-mapped readings by caliceal and infundibular location are noted in Table 1. The distribution of blood flow did not differ significantly between anterior calices (n = 544, 11.9% high flow, 88.1% low flow) and posterior calices (n = 512, 15.8% high flow, 84.2% low flow) (p = 0.10). Further analysis also showed no significant difference in the distribution of blood flow at the upper pole (n = 368, 51.5% high flow, 48.5% low flow), interpolar (n = 352, 14.5% high flow, 85.5% low flow), and lower pole (n = 336, 13.7% high flow, 86.3% low flow) calices (p = 0.90). Alternatively, both the anterior and posterior infundibular blood flows were more often noted to be high (48.2% and 48.6%, respectively) than that of the anterior and posterior caliceal fornices (11.9% and 15.8%, respectively) (p < 0.001). In addition, the blood flow at the upper pole, interpolar, and lower pole infundibula was more often regarded as high compared with the blood flow at the upper pole, interpolar, and lower pole caliceal fornices (p < 0.001).
Comparison of Blood Flow by Infundibular and Caliceal Location
Anterior vs posterior total four comparisons, α < 0.0125 considered significant. Upper pole vs interpolar vs lower pole total six comparisons α < 0.00833 considered significant. Comparisons that were statistically significant are noted in the last column, whereas comparisons that were not significant are omitted.
α adjusted using Bonferroni correction to control for multiple comparison.
AC = anterior Calyx; AI = anterior Infundibulum; IPC = interpolar Calyx; IPI = interpolar Infundibulum; LPC = lower pole Calyx; LPI = lower pole Infundibulum; PC = posterior Calyx; PI = posterior Infundibulum; UPC = upper pole Calyx; UPI = upper pole Infundibulum.
Comparisons of Doppler-mapped readings at the positions of the caliceal fornices are found in Table 2. Of note, high blood flow was more frequently reported at the 6 o'clock forniceal position (25.8% high flow) compared with the other forniceal locations (high flow readings ranging from 8.3% to 12.1%) (p < 0.001). In contrast, the center of each papilla had significantly less blood flow (p < 0.001) compared with any region along the fornix (Table 2). Indeed, the Doppler probe did not detect demonstrable blood flow in the center of any papilla (i.e., rate “0” for all 264 papillae studied).
Comparison of Blood Flow by the Positions of the Caliceal Fornices
Four total comparisons so α < 0.0125 is considered significant. Comparisons that were statistically significant are noted in the last column, whereas comparisons that were not significant are omitted.
α adjusted using Bonferroni correction to control for multiple comparison.
CP = center of papilla.
Discussion
There has been a marked increase in the prevalence of urolithiasis in the United States with 1 in 11 persons affected. 7 Percutaneous nephrolithotomy (PCNL) is the standard of care for large renal stones (>2 cm) 8 with contemporary data showing that PCNL utilization is on the rise from 1.7/100,000 in 1999 to 3.6/100,000 in 2014 Refs. 9,10 ). This is possibly because PCNL is associated with a higher stone-free rate than retrograde intrarenal surgery, although at the expense of a higher complication rate (i.e., 23% overall; 3.3% with a blood transfusion). 10,11
Hemorrhage encountered during a PCNL negatively impacts observation and reduces stone-free rates. In 1% to 2.6% of cases, the hemorrhage is life threatening and there is a need for postoperative angioembolization with attendant loss of renal parenchyma. 12 –15 The Doppler probe used during flexible ureteroscopy in this study, if brought into the clinical realm, could allow for safer access as the calyx of entry could be mapped before puncture, allowing for selection of the least vascular site when performing an endoscopic guided percutaneous access in the traditional antegrade manner or in the more recently described retrograde manner. 16,17
Current information regarding anatomic relationships of the intrarenal vessels comes from studies performed in cadaveric kidneys. 18,19 These studies showed that percutaneous access conducted at the level of the renal calyx is preferred as a puncture in the infundibulum or in the direction of the renal pelvis theoretically increases hemorrhagic risk. Although our findings are consistent regarding infundibular blood flow, our study went a step further by showing no appreciable flow detected by the Doppler US probe in the center of each papilla. Interestingly, we also found that the 6 o'clock forniceal position had a consistently higher blood flow and should likely be avoided when considering renal access. There were no differences in blood flow noted between the anterior and posterior calices.
There have been several recent technological advances in renal access for PCNL including utilizing electromagnetic sensors (Aurora EMT Systems; Northern Digital, Waterloo, Canada) and also robot-guided percutaneous access. 20,21 These techniques both represent possible improvements to the fluoroscopically guided endoscopically blind antegrade puncture technique that is traditionally used by most radiologists and urologists for renal access. An alternative approach to help reduce vascular injury would be to direct access through the center of a papilla under endoscopic guidance either in the traditional outside–in manner or with an inside to outside approach using a Lawson puncture wire or, as recently described by Kaler et al., a holmium laser. 17 Alternatively, if one wished to spare the papilla, a logical next step would be to utilize the Doppler probe through the ureteroscope to identify the least vascular access site along the fornix, which would then be used to establish access in a highly precise endoscopically controlled antegrade or retrograde manner.
The major limitation to this study was that the renal vasculature was mapped only in female pigs of the same size and weight. Whether the findings are the same in male pigs has yet to be determined. Also we did not simultaneously measure pressure within the calices or renal pelvis while doing the study, so it is conceivable that the intracaliceal blood flow was to some extent blunted. Indeed, in one of our studies in which a 14F access sheath was used during measurement of intracaliceal pressure in the clinical situation, an inflow irrigant pressure of 150 mm Hg raised the intracaliceal pressure up to 40+ mm Hg (R. Patel, unpublished data). Similarly how well this characterization of blood flow at the urothelial level transfers to the human situation remains unknown; however, the intrarenal vasculature of porcine kidneys has been extensively compared with that of humans and many similarities exist to support the porcine kidney as the best surrogate for the human kidney. 22 Future clinical studies with the ureteroscopic Doppler probe are pending Food and Drug Administration approval of a Doppler probe suitable for use through a flexible ureteroscope.
Conclusions
Utilizing a unique miniaturized Doppler ultrasound unit, the in vivo mapping of porcine calices revealed areas of high blood flow along the infundibula throughout the kidney. With regard to the renal fornices, 6 o'clock position along the fornix had the highest blood flow although significantly less than along the infundibula. The renal papilla revealed no perceptible blood flow.
Footnotes
Acknowledgments
The authors thank Christina Hwang, Krista Larson, and Zachary Valley for assistance during the laboratory experiments.
Author Disclosure Statement
The authors have no conflicts of interest.
Funding Information
No funding was received for this article.