
Abstract
Aim:
To test the characteristics of a hybrid laser (combination of a thulium and blue diode laser) vs thulium and Ho:YAG lasers regarding soft tissue ablation.
Methods:
Tissue samples of fresh nonfrozen porcine kidneys were used to compare the three lasers. A motorized translation XY stage with a fixed fiber holder to control the speed of cutting (2 and 5 mm/s) was used. Five incisions with each laser were performed. Lactate dehydrogenase staining of the embedded specimens was performed to determine incision depth, zones of vaporization, coagulation zone, carbonization grade, and thermomechanical damage of the coagulated tissue. All data are expressed as mean ± standard deviation.
Results:
The hybrid laser demonstrated the highest vaporization speed (34.4 ± 0.1 mm3/s) and coagulation zones (10 ± 0.1 mm2) at a drag speed of 5 mm/s among the investigated lasers. It showed a two to three times larger coagulation zone compared with the Ho:YAG laser (4 ± 0.1 mm2). The continuous wave thulium fiber laser (cwTFL) showed a significantly higher grade of carbonized tissue compared with the hybrid and Ho:YAG lasers.
Conclusions:
The hybrid laser showed deeper incisions and a faster vaporization speed compared with the cwTFL and the Ho:YAG laser. It might be an effective tool to combine the advantages of both lasers to effectively vaporize soft tissue with excellent coagulative properties.
Introduction
Laser enucleation of the prostate (LEP) has shown significantly less bleeding rates in comparison with transurethral resection of the prostate (TURP) and open prostatectomy (OP). 1 It has already been demonstrated that the holmium laser is effectively absorbed by water because of its wavelength of 2.1 μm. 2 The continuous wave (cw) thulium fiber laser (TFL) has a similar wavelength of 1.94 μm with an even stronger water absorption and better cutting effects caused by the cw mode. 3 It has been shown that LEP using a holmium or a thulium laser is highly effective as a minimally invasive technique for the treatment of benign prostatic hyperplasia (BPH). Both procedures lead to a long-lasting micturition improvement. 4 In a randomized study, both techniques showed a comparable complication rate with a similar postoperative outcome. 5 Despite a significant lower rate of blood transfusions in comparison with TURP and OP, the bleeding complication rate is still a major issue during LEP in patients with ongoing oral anticoagulation. 6,7
Another promising technique for endoscopic enucleation of the prostate (EEP) is the bipolar enucleation of the prostate. After 1 and 5 years of follow-up it showed comparable functional results with shorter hospitalization and catheterization rates compared with TURP. 8 Despite these encouraging results of EEP techniques, the ablative procedures in BPH have yet not been elucidated appropriately.
A novel and simple method, yet a prototype of a laser, which might minimize the complications could be a hybrid laser that combines two different wavelengths: one that has its absorption maximum in water and one with hemoglobin as its target chromophore.
A blue diode laser (BDL) that emits light at a wavelength of 0.45 nm was first introduced in 2015 in dental surgery to reduce bacterial colonization and to coagulate and cut soft tissue. 9,10 Braun and colleagues tested a 445-nm semiconductor laser using pork oral mucosa. 10 It showed clinically acceptable incision depths at low energy outputs without signs of extensive tissue denaturation. 10 A few years before, Ishikawa and colleagues showed that a blue–violet light-emitting diode caused immediate clot formation and hemostasis in an in vitro setting. 11 Jiang and coworkers even demonstrated a fourfold better tissue vaporization using a BDL compared with a Greenlight laser with similar coagulation properties. 12
The ablative and coagulative properties of the BDL appear to be promising for the treatment of BPH. So far, however, there are no studies that systematically examine the hypothesis if a hybrid laser can be safely applied for soft tissue ablation. The aim of our study was, therefore, to test the characteristics of a hybrid laser (combination of a thulium and BDL) vs thulium and Ho:YAG lasers regarding soft tissue ablation.
Materials and Methods
Fresh nonfrozen porcine kidney samples were obtained. The tissue samples were cut with an electric slicer into 8 mm thick samples. The experimental setup used in this study has been described before by Becker and colleagues. 3 Table 1 lists the lasers with its physical properties that were used during the experiments. In total, three lasers were tested: (1) Ho:YAG laser (Lumenis, USA; 550 μm fiber), (2) cwTFL (NTO IRE-Polus, Russia; 600 μm fiber), and (3) prototype of a hybrid laser (cwTFL/BDL, NTO IRE-Polus, Russia; 600 μm fiber).
Laser Characteristics and Laser Settings of the Investigated Lasers (Ho:YAG, Thulium Fiber Laser, and Hybrid Laser (Thulium Fiber Laser and Blue Diode Laser)) and Results of Histopathological Evaluation
BDL = blue diode laser; TFL = thulium fiber laser.
The incisions were performed on a motorized XY translation stage with a fixed fiber holder to exactly maintain the cutting speed of 2 and 5 mm/s, respectively (Fig. 1). All incisions were made in saline. The distance between the tissue surface and laser fiber tip was set to 0.1 mm. To minimize the range of measurements, five incisions were performed with each laser.
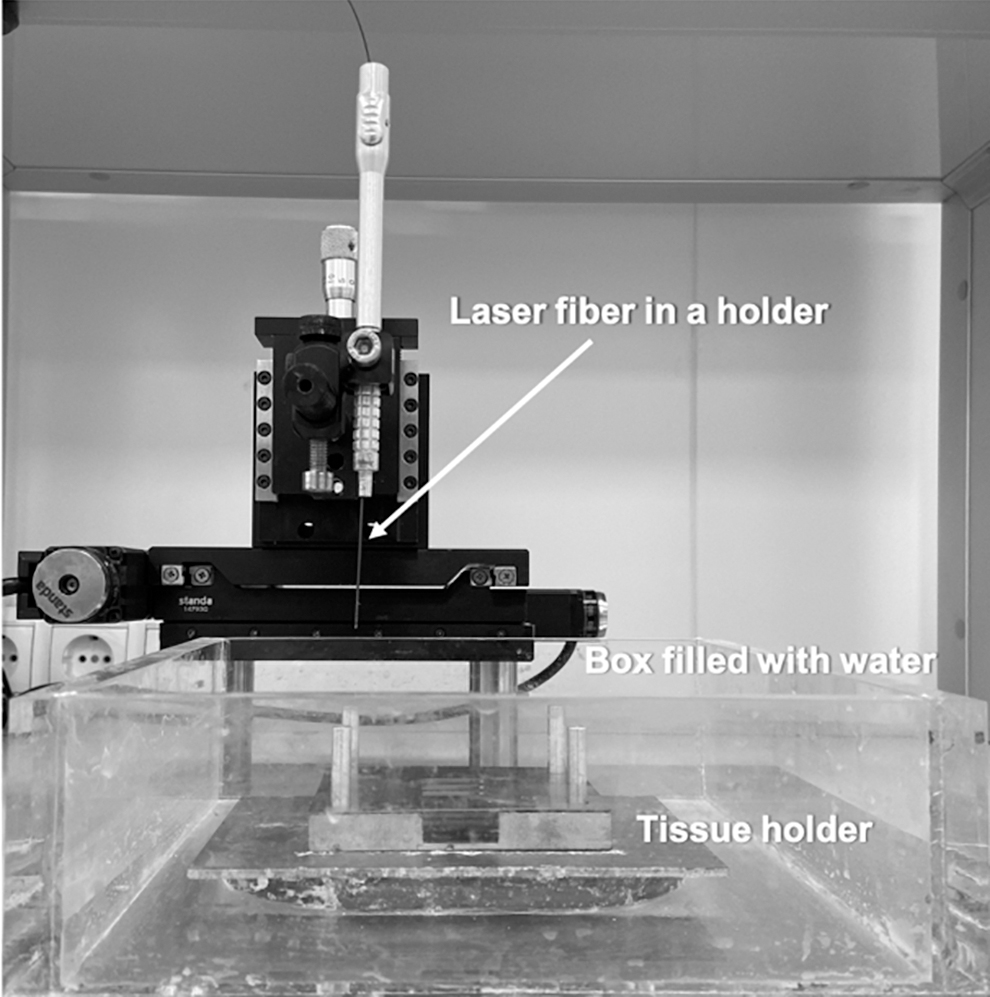
Experimental setup.
Afterward, all samples were sliced with a microtome (LEICA RM2235; Leica Biosystems, Switzerland) into 300 μm thick cryosections. For analysis of laser-induced thermal damage, a lactate dehydrogenase staining of the embedded specimens was performed. For each incision, five cryosections were analyzed.
A microscope (LEICA DM1000 B LED) with a digital camera (LEICA DFC7000 T) was used for histopathological examination. Laser wound analysis was separately performed by a pathologist and a urologist. Incision depth (mm), coagulation zone (mm2), zones of vaporization, and thermomechanical damage (mm2) were evaluated. The thermomechanical damage was defined as the superficial layer with pronounced irregular mechanical damage of the coagulated tissue. Furthermore, the carbonization grade (CG) was qualitatively assessed from 0 (no carbonization) to 3 (strong carbonization). Laser vaporization speed (mm3/s) was calculated as the area of vaporized tissue multiplied by the speed of cutting.
All data are expressed as mean ± standard deviation. For data analysis, the SPSS 23 software package (IBM Corp., Armonk, NY, USA) was used.
Results
All laser characteristics, laser settings, and the histopathological findings are shown in Table 1. Figure 2a and b demonstrates exemplary histological effects after performing the laser cuts. Figure 2c shows how zones of vaporization, coagulation, and carbonization were measured. In our experiments, the Ho:YAG laser showed smaller incision depths (2.5 ± 0.1 mm) and coagulation zones (4.0 ± 0.1 mm2) at a speed of 2 mm/s in comparison with the other lasers. At a higher cutting speed of 5 mm/s, the incision depth and coagulation zone were lower with 1.1 ± 0.1 mm and 2.1 ± 0.1 mm2, respectively. Owing to the energy transmission in a pulsed mode, we noticed ruptured margins of the incisions without carbonized tissue (CG 0) in all samples (Fig. 3).

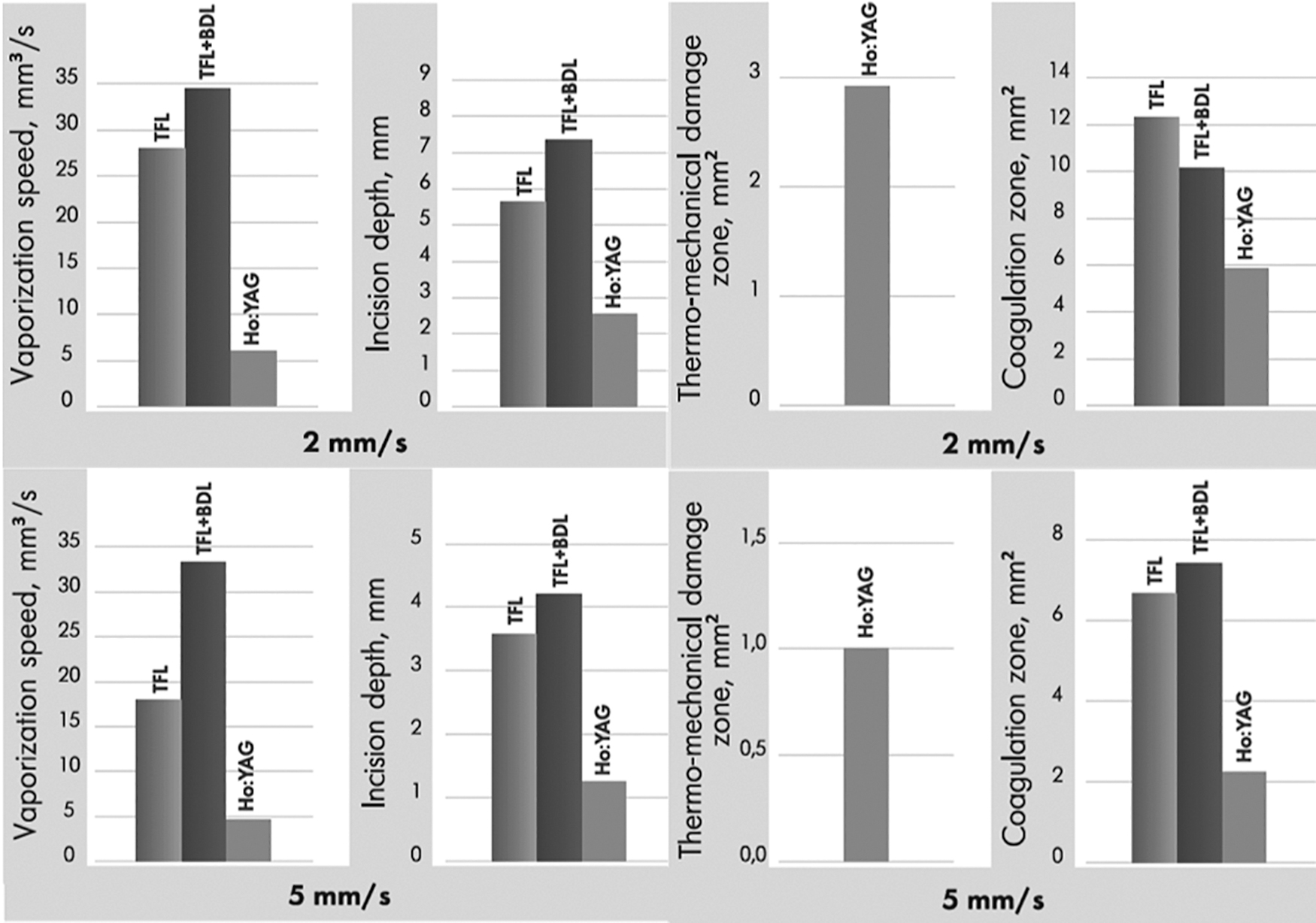
Results of vaporization speed (mm3/s) and thermomechanical damage zone (mm2) after laser cutting at 2 and 5 mm/s, respectively.
The cwTFL mainly showed coniform formed tissue cuts with a mean incision depth of 5.5 ± 0.1 mm and coagulation zones of 12.5 ± 0.1 mm2 at a drag speed of 2 mm/s. At a cutting speed of 5 mm/s, only little decrease was noted in the incision depth with 4.5 ± 0.1 mm. However, the coagulation zone showed half as much coagulated tissue (6.5 ± 0.1 mm2). At both drag speeds, the tissue showed less ruptured margins compared with the Ho:YAG laser, however, with a higher grade of carbonization (CG = 2–3).
The hybrid laser demonstrated the deepest incision depth among the lasers with 7.3 ± 0.1 mm at 2 mm/s. At this speed, it showed a smaller coagulation zone compared with the cwTFL with 10 ± 0.1 mm2. After acceleration of the drag speed, the incision depth and coagulation zone decreased to 4.1 ± 0.1 mm and 7.1 ± 0.1 mm2, respectively. Wound analysis revealed deep narrow cuts with sharp margins with minimal to average carbonization (CG 0–1). With regard to vaporization speed, the hybrid laser showed significantly higher values compared with the Ho:YAG and TFL at both drag speeds (Table 1).
Discussion
In this study, we investigated the tissue effects of different lasers in an in vitro kidney model. We showed that all tested lasers lead to effective tissue vaporization and coagulation with a drag speed of 2 and 5 mm/s, respectively. Overall, the hybrid laser showed the highest vaporization (34.4 ± 0.1 mm) and coagulation (7.1 ± 0.1 mm) zones at a drag speed of 5 mm/s. It showed a two to three times larger coagulation zone compared with the Ho:YAG laser and less carbonization in comparison with the cwTFL.
A hybrid laser that combines the cutting abilities of a cwTFL and the coagulation properties of a BDL might overcome the risk of bleeding with a comparable outcome as reported for LEP. Owing to the instant coagulation, particularly in a noncontact mode, the surgeon easily keeps the overview of the surgical site without formation of coagula at the laser fiber tip. 11 Therefore, the combination of both wavelengths could lead to a more effective treatment with less operation time caused by significantly higher vaporization volumes in comparison with the well-established Ho:YAG and cwTFL. It was a surprising finding that the hybrid laser causes less coagulation than the TFL alone. Owing to the combination of the hybrid laser, a better vaporization of the tissue can be achieved. The part of the tissue that would have been coagulated by the cwTFL itself is vaporized with the hybrid laser. Therefore, it leads to deeper incisions and decreases coagulation in comparison with the cwTFL. The deep incision depths might be disadvantageous during LEP, because deeper tissue cuts lead to less meticulous lasering near the prostate capsule. However, in terms of vaporization the hybrid laser might be useful in some steps of EEP, yet without affecting the complication rate because of only minimal changes compared with the established lasers. These intraoperative aspects have yet to be tested in clinical trials. The Ho:YAG laser showed the lowest incision depth of 2.5 mm at a drag speed of 2 mm/s and is well comparable with a study that was published in 2018. 13 The slight difference between these two experiments could be because of the fact that Emiliani and colleagues chose a faster drag speed (3 mm/s) and had lower power settings compared with our experiments. However, in the literature it was shown that most of the prostate capsule ruptures happen because of the technique and the anatomy of the prostate independently of the device used for EEP. 14
The coagulation zone at a drag speed of 5 mm/s resulted in a larger coagulation zone of the hybrid laser compared with the cwTFL. The main advantage could, therefore, be at the end of surgery because of better coagulation performance with an enhanced bleeding control in the prostate fossa. The superior ablation capacity with the BDL in comparison with 970 nm and KTP:YAG lasers was described before. 10,15 Gobbo and colleagues investigated the BDL in comparison with other surgical techniques and showed that it minimizes the risk of bleeding with only little thermal damage. 16
One interesting outcome was that the hybrid laser was associated with decreased carbonization compared with cwTFL. This might be because of the fact that the lasers of the hybrid laser are absorbed in different media, that is, water (TFL) and hemoglobin (BDL), whereas the cwTFL is only absorbed in water. 16 Therefore, the energy transmission of the hybrid laser is distributed to the two media instead of only water. Since carbonization occurs primarily when water is vaporized, the carbonization rate is higher if the cwTFL is used exclusively.
This might lead to less urge incontinence in the immediate postoperative course after the use of a hybrid laser, although it delivered deeper changes in the tissue in our study. 17 However, it is to note that no clinical study could yet prove the fact that less carbonization layer and clearer cuts lead to less urge incontinence. 5
In our experiments, the Ho:YAG laser showed tissue cuts free of carbonization with a minimal vaporization and coagulation depth. This is most likely because of its pulsed mode that allows a thermal relaxation of the tissue with a decrease in both vaporization and coagulation. 18
Another factor that shows the intensification of the hybrid laser is the form of the tissue cuts. The cwTFL leads to conical cuts, whereas the hybrid lasers showed a more cylindrical tissue ablation. This suggests that the laser energy is minimally reflected or absorbed in carbonized tissue using the hybrid laser.
These properties would be useful not only in the therapy of BPH but also in the field of partial nephrectomy. Arkhipova and colleagues investigated a BDL during laparoscopy in an animal model. 19 They demonstrated an almost carbonization-free resection using a combination of a cwTFL and a BDL in pig kidneys. In this study, the laser-induced ablation was not affected by the presence of CO2; however, the coagulation thickness was less using the BDL in a CO2 environment. 19 In our experiments, all incisions were performed in saline, which limits its applicability to laparoscopy. Further investigations targeting the use in laparoscopy would, therefore, be necessary.
Despite the high standardization of our experiments, some limitations have to be mentioned. First, we used a nonperfused kidney model. We believe that a blood supplied organ might lead to an inability to correctly control all measured variables; however, especially the effect of coagulation cannot be easily transferred to a human prostate or kidney. Second, it is difficult to compare our results with other studies, since even slight differences in drag speed and power settings can lead to errors in interpretation. We believe that our model can be easily copied with the specified settings and thus better comparability can be achieved. But, because of the fact that the laser fiber cannot be kept at a constant speed in clinical use, we would recommend performing following experiments at different drag speeds to better interpret the range of results. Third, the distance between the laser fiber and the tissue was a constantly kept at 0.1 mm. This leads to a high comparability of the histological results, but it is difficult to interpret clinically, since the distance alternates in air-made incisions. Finally, we used different sized laser fibers; however, the Ho:YAG laser that was used in our study could only be operated with specially designed fibers (550 μm fiber; SlimLine).
It is difficult to develop a new laser in addition to the existing lasers, which is even more effective than the previous ones. Other attempts of a hybrid laser showed promising results; however, no advantages over already established lasers were seen and hence it did not find entry into the market. 20 We believe that the hybrid laser has the potential to clinically exist alongside Holmium:Yttrium-Aluminium-Garnet (Ho:YAG), Thulium (Tm), and potassium-titanyl-phosphate (KTP) lasers. To confirm this, further studies, especially in a clinical setting, must be awaited.
Conclusions
It seems that the hybrid laser could be a useful device in terms of vaporization of soft tissue. It demonstrated the fastest vaporization with the largest coagulation zone at 5 mm/s drag speed. It further showed a minimal carbonization compared with the cwTFL. This study was conducted to only investigate the ablative properties. Whether this laser proves itself clinically has yet to be clarified.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.