
Abstract
Background and Objectives:
Transurethral resection of the prostate (TURP) is considered to be the gold standard surgical procedure for medium-sized prostates. However, there is a drastic difference between the weight of resected tissue reported by the pathologist and the sonographic estimate of prostate weight before the operation. The present study investigates the role of electrocoagulation in tissue loss during monopolar (M-) and bipolar (B-) TURP.
Methods:
In this experimental in vitro study, 33 prostate glands removed from patients by open suprapubic prostatectomy were roughly divided in half and the weight of each half was recorded precisely. One half of the specimen was resected using a monopolar resectoscope and the other half was resected by bipolar resectoscope in an out-of-body simulated condition. The weight of obtained chips was measured and the amount of lost tissue was calculated. Data from prostates with final pathologic diagnosis of benign prostatic hyperplasia were included in the analysis. The mean difference of prostate weight before and after out-of-body resection and also the proportion of tissue loss between M-TURP and B-TURP were compared using t-test.
Results:
Data from 62 prostate halves were included in the final analysis. The mean weight of samples after M-TURP was considerably lower than before resection (38.0 ± 6.9 and 48.7 ± 9.0, respectively, p < 0.001). Similarly, the mean weight of prostate samples after B-TURP was lower than the weight before resection (36.2 ± 7.3 and 48.4 ± 9.1, respectively, p < 0.001). However, the ratio of tissue loss in B-TURP (25.3% ± 2.5%) was significantly higher than in M-TURP (21.3% ± 3.7%) (p < 0.001).
Conclusion:
Prostate resection using electrocoagulation leads to a significant prostate tissue loss due to heat effect. Furthermore, tissue loss in B-TURP is slightly more than M-TURP.
Introduction
Benign prostatic hyperplasia (BPH) is one of the most common urologic diseases. Despite numerous procedures having been developed, transurethral resection of the prostate (TURP) is still the most practiced surgical method used for BPH treatment. 1 One of the relative contraindications of performing TURP is large prostatic size. Therefore, choosing the best surgical approach for treatment is dependent on prostate size, with the European Association of Urology and American Urological Association guidelines recommending TURP for medium-sized prostate glands (i.e., 30–80 mL). 2,3 Assessment of prostate size before operation is usually done using transabdominal ultrasonography due to its availability and low cost. However, transrectal ultrasonography and magnetic resonance imaging (MRI) are more precise in estimating prostate size. 4,5
In daily practice, the weight of resected tissue reported by the pathologist is often lower than the preoperative sonographic estimate of total prostatic volume. The most important explanation for this difference is reporting the total sonographic volume of prostate instead of volume of transitional and periureteral zones of prostate, which are resected in a complete TURP. In previous studies, the final amount of resected tissue was even smaller than the transitional zone volume (TZV) estimated by ultrasonography and researchers repeatedly associate this finding with an incomplete resection. 6 –8 However, it is possible that there are other reasons behind this. We hypothesized that part of the prostate tissue is lost due to the heat produced by resection with electrocoagulation. In addition, it is worth noting that the amount of heat applied to the tissue, resection method, and homeostatic maneuvers are different between bipolar TURP (B-TURP) and monopolar TURP (M-TURP), which may lead to varying amounts of tissue loss between these methods. Previous studies that compared the two approaches have reported a lower resected tissue weight to preoperative prostate size ratio in B-TURP, although no statistical test was performed in any. 9 –12 Considering that no previous study has explored the precise quantity of tissue loss, we conducted the current in vitro study to measure and compare the amount of tissue loss in both B-TURP and M-TURP.
Patients and Methods
This experimental in vitro study was performed from January to June 2019 after being approved by the Research Ethics Board of Isfahan University of Medical Sciences. Patients who were candidates for open prostatectomy were evaluated for eligibility. Patients with prostate-specific antigen (PSA) level greater than 4 ng/dL, those with prostatic nodule felt in digital rectal examination, and patients with a history of prostate biopsy in the last 3 months were excluded. Transabdominal ultrasonography was performed by an experienced radiologist. Length, width, and height of the prostate were measured using a 3.5 MHz transducer, and prostate volume was calculated using the formula for the volume of a prolate ellipsoid (width × length × height × π/6). 13 Since the specific gravity of prostate tissue is 1.06 g/mL, the estimated volume is almost representative of the prostate weight. 14
Urinary tract infection was treated before the operation and the decision for performing open surgery or TURP was made based on the prostate size and cystourethroscopy. Patients had a minimum prostate size of 80 mL. After changing the patient's position to supine, a lower midline incision was made and suprapubic transvesical prostatectomy was performed. After prostate enucleation, the extracted tissue was cut roughly in half by an assisting surgeon. First, the weight of each half was determined by a precise scale (Metro Electronic, India) by two decimal points. Then, one half using a monopolar resectoscope and the other half using a bipolar resectoscope underwent resection in an out-of-body simulated condition by another surgeon solely tasked with the resection of samples. All procedures were performed using the KLS Martin® ME 402 maXimum radiofrequency generator, compatible resectoscopes, and disposables (Karl Storz Endoscope, Tuttlingen, Germany). The cutting power for M-TURP and B-TURP was 90 and 80 W, respectively. Coagulation was not performed.
To simulate M-TURP, a prostate half was placed in a stainless-steel kidney bowl filled with 300 mL of glycine. The kidney bowl was placed on a cautery plate to create a closed electrical circuit. With the prostate tissue touching the inner wall of the bowl, monopolar resection was performed in the liquid resembling real TURP conditions (Fig. 1). The resulting chips were sifted and after allowing the liquid on the samples to drain passively for 1 minute, their weight was measured using the same scale. To simulate B-TURP, the other prostate half was placed in an insulated container filled with 300 mL of physiologic saline. Resection was performed using the same method as monopolar resection, with the only exception being the prostate not touching the inner wall of the container. Both monopolar and bipolar resections were performed by the same surgeon with an appropriate level of experience with both systems. It took about 5 minutes to resect each prostate lobe by either M- or B-TURP system. The obtained chips were measured and the weight was documented. The chips were sent for pathologic examination and data from prostates diagnosed with BPH entered the final analysis. Specimen weight reported by the pathologist was also recorded. Data were entered in IBM SPSS Statistics 20 software. T-test for independent samples was used to compare the prostate tissue weight before and after resection (primary outcome) and also to compare the rate of tissue loss between M-TURP and B-TURP (secondary outcome). Level of significance was set at 0.05.

Out-of-body prostate resection by monopolar resectoscope.
Results
Enucleated prostates from 31 patients with a mean age of 69.3 ± 7.1 years and mean PSA levels of 3.2 ± 1.8 ng/dL were included in the analysis. The mean preoperative sonographic volume of prostates was 112.8 ± 25.3 mL. Based on the pathologic examination, one case of xanthogranulomatous prostatitis and one case of prostate cancer with more than 5% of chips involved were excluded from the final analysis.
In the monopolar group, the mean weight of the tissue before resection was 48.7 ± 9.0 g, which was reduced to 38.0 ± 6.9 g after resection (p < 0.001). Similarly, tissue weight was decreased significantly after bipolar resection (48.4 ± 9.1 vs 36.2 ± 7.3, p < 0.001) (Fig. 2). The relative amount of reduced tissue weight in monopolar and bipolar resection was 21.3% ± 3.7% and 25.3% ± 2.5%, respectively (p < 0.001) (Table 1). The sum of the average weight of resected tissue by both resectoscopes was 74.2 ± 14.2 g, which was different from the pathology report of the sample weight after fixation in formalin (67.5 ± 12.4 g, p < 0.001).
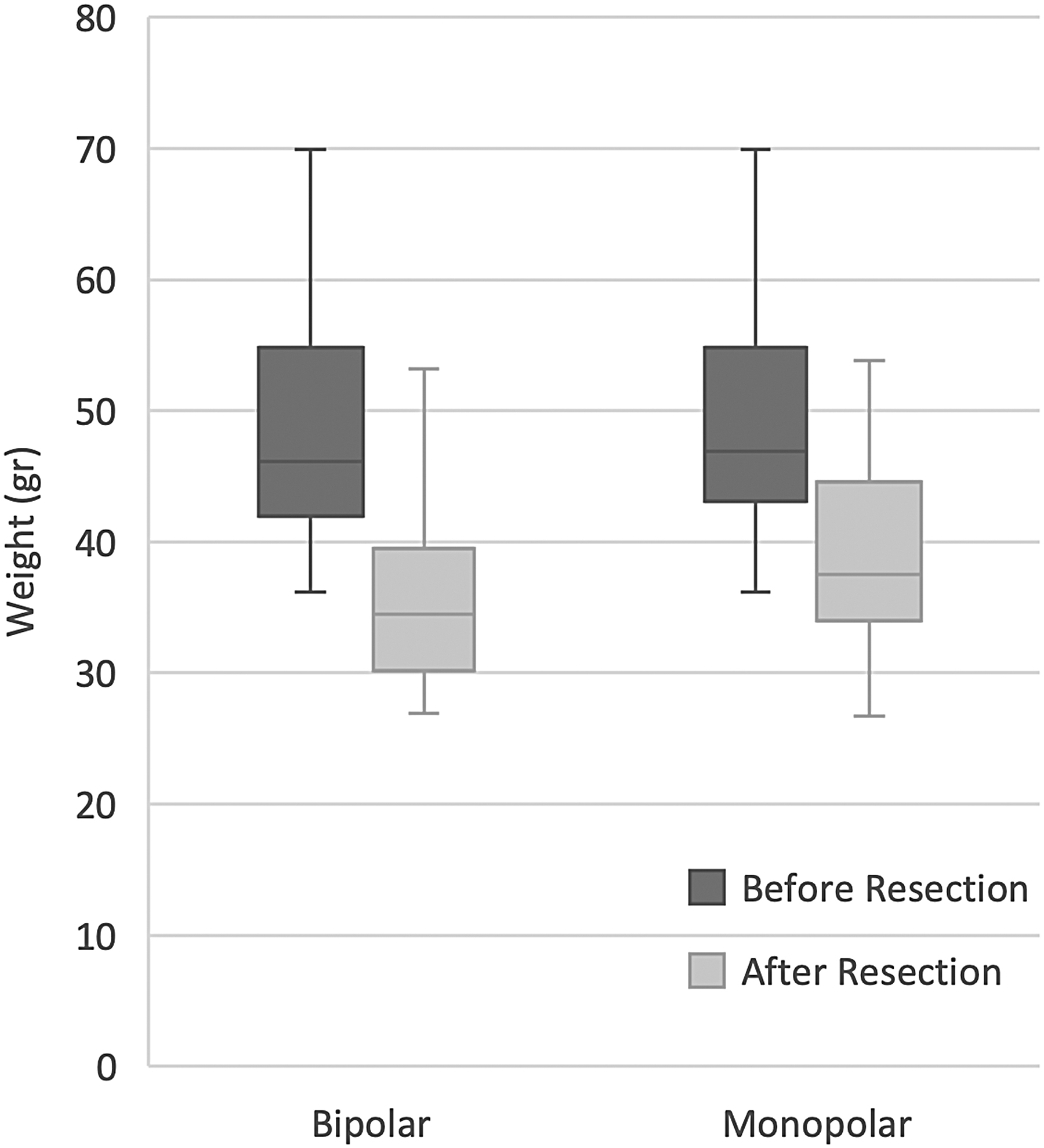
Box-plot showing weight before and after resection of prostate by different resectoscopes.
Weight Assessment Values
SD = standard deviation; TURP = transurethral resection of the prostate; B-TURP = bipolar TURP; M-TURP = monopolar TURP.
Discussion
Our results indicated that a significant amount of tissue is burned and lost during both monopolar and bipolar systems, but higher in B-TURP (∼25%) than M-TURP (∼21%). To our knowledge, our study is the first to experimentally determine the amount of tissue loss due to TURP in an in vitro model. Studies on TURP outcomes performed usually on medium-sized prostates showed that the resected tissue weight is 28%–78% of preoperative sonographic total volume of prostate. 9 –12,15–17 So far, the major reasons behind this have mainly been presented as the resection of only transitional and periureteral prostate zones in a complete TURP and simply an incomplete resection. Another reason offered by Lukacs and colleagues was a 13.3% loss of tissue after fixation with formaldehyde, which is concordant with 10% reported in our study. 18 The findings of this article provide another reason by explaining the effect of heat generated from electrocoagulation on tissue loss.
Our results demonstrated that B-TURP caused more tissue loss than M-TURP. In monopolar circuit, the return electrode is placed in a region of the body far from the active electrode. Therefore, the current travels a notable distance to reach the end of the circuit. 19 In contrast, in the bipolar method, the return and active electrodes are positioned close to each other. Thus, the current only travels a short distance between the electrodes. 20 Bipolar systems need lower energy and voltage to complete the circuit owing to less tissue and thus lower resistance. Usually in a monopolar system, the urologist quickly performs the resection and leaves the homeostasis until the end of operation. In contrast, during B-TURP, the low voltage leads to some levels of homeostasis. Homeostasis is not controlled by the depth of current penetration in M-TURP, but it is dependent on the speed with which the loop passes through the tissue during bipolar resection and it is recommended to lower the speed of resection to benefit from the simultaneous homeostasis during the B-TURP.
The bipolar system fosters the possibility of performing TURP in physiologic saline. Prevention of transurethral resection (TUR) syndrome during B-TURP makes it possible to be performed with care and at a slow pace. However, previous studies have not described longer operation time for B-TURP, which can be explained by the time attained from better homeostasis during this procedure. 5,17,21 –24 The increased homeostasis during B-TURP leads to higher tissue burning and evaporation compared with M-TURP and explains our results of more tissue loss using the bipolar system. In separate studies performed by Huang and colleagues on pathologic specimens of TURP, the authors showed that B-TURP has a mean coagulation depth bigger than the maximum microvessel diameter, and B-TURP has better hemostatic capability than M-TURP. 15,25 Although no study has directly compared the amount of tissue loss between M-TURP and B-TURP, many have researched the consequences of these systems and reported the volume of prostate before and weight of resected tissue after the surgery separately. The weight to volume ratio calculated from these studies was 2%–10% more in M-TURP than B-TURP, which is consistent with the findings of the present study. 9 –12
The most prominent limitation of this study was the out-of-body resection. Despite our efforts to reproduce a real TURP during the resection, there are still differences: often, in an actual TURP, first chips are larger than the last ones. Although we attempted to reduce this difference by replicating an actual resection technique, in out-of-body resection, there is no need for electrocoagulation, while during TURP occasionally there is a need for coagulation before finishing resection, which can theoretically affect the amount of evaporation; Out-of-body resection of last chips in monopolar system is difficult owing to the need for direct contact of tissue with the container wall. Although the last chips form a small portion of the total volume and the confounding effect will be negligible; and finally, the current study involved larger prostate specimens from patients undergoing open prostatectomy which have epithelial nodule predominance unlike smaller prostates undergoing TURP with predominance of fibromuscular stroma. 26,27 This possible histopathologic difference may slightly influence the tissue resistance and electrocoagulation properties.
Despite all of the aforementioned limitations in out-of-body resection of the prostate, they seem to have little to no effect on the final outcomes of the study. Furthermore, the benefit of out-of-body resection of prostate for assessment of tissue loss outweighs the limitations. M-TURP may not allow full resection due to the risk of developing TUR syndrome, while B-TURP provides the opportunity to fully resect the prostate with near perfection. On the contrary, a direct and trustable measurement of tissue weight is unlikely in clinical studies, even with the aid of MRI to determine the TZV, which will be resected during the procedure. Therefore, a clinical study cannot effectively measure and compare the amount of tissue loss without error, while this study with an in vitro design succeeded in tackling this issue.
Several clinical studies have discussed the effect of a complete prostate resection on some clinical outcomes by comparing the sonographic TZV before the operation with the weight of resected tissue. 6 –8 Acknowledging the fact that a noteworthy part of the tissue is lost during resection allows the urologist to be cautious in associating the degree of resection completeness with clinical outcomes and equips it with better foresight in research design or data analysis.
In summary, the four major reasons for the weight of resected tissue by TURP being lower than the estimated sonographic volume are (1) resection being limited to transitional zone and periurethral tissue during the operation, (2) performing an incomplete TURP, (3) loss of tissue due to the heat generated as a result of electrocoagulation, and (4) tissue reduction after fixation with formaldehyde. Other possible reasons for the issue are tissue blood loss throughout the resection and loss of small chips during sample collection. Even if the precise weight of prostate after operation is not of high importance yet, it is well established that it should be recorded as it may be valuable in future research and critical in precise documentation.
Conclusion
Prostate resection using a resectoscope leads to a significant loss of tissue due to tissue evaporation caused by heat resulted from electrocoagulation. This article provides another reason for the drastic difference between the sonographic size of the prostate before surgery and the final weight reported by the pathologist. In addition, the loss in M-TURP and B-TURP is unequal, a difference that can be explained by their different mechanisms of action.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.