
Abstract
Objective:
To evaluate the feasibility of three bladder neck reconstruction (BNR) techniques in laparoscopic radical prostatectomy (laparoscopic RP) and their effects on urinary continence.
Methods:
We retrospectively analyzed 121 patients with organ-confined prostate cancer, who underwent laparoscopic RP in our center from March to December 2018. Three BNR techniques—zero o'clock reconstruction (ZOR), six o'clock reconstruction (SOR), and three/nine o'clock reconstruction (T/NOR)—applied in patients with large bladder opening after prostate resection are described comprehensively. Demographic and perioperative data were collected and analyzed using Pearson's chi-square and one-way analysis of variance test. Multivariate analysis was performed to explore predictors that affected continence recovery in 24 hours, 1 month, 3 months, and 6 months after catheter removal.
Results:
Laparoscopic RP was performed in all patients, wherein 37, 35, 34, and 15 patients underwent bladder neck preservation, ZOR, SOR, and T/NOR techniques, respectively. There were more high-risk patients and larger mean prostate volume in groups with BNR techniques. Perioperatively, patients with reconstruction techniques had longer operation and anastomosis time, more estimated blood loss, and more positive margin status. Nevertheless, there was no significant difference among four groups regarding continence recovery in 24 hours, 1 month, 3 months, and 6 months after catheter removal. On multivariable analysis, positive apical margin and long anastomosis time were independent adverse predictors of continence recovery in 24 hours. Large prostate volume and positive apical margin were adverse factors of continence recovery at 1, 3, and 6 months.
Conclusion:
Three different kinds of BNR techniques were safe and feasible in laparoscopic RP and had no different impact on continence recovery. Positive apical margin, large prostate volume, and long anastomosis time were independent adverse predictors of continence.
Introduction
Radical prostatectomy (RP) is the optimal management for organ-confined prostate cancer, 1,2 which aims to achieve complete cancer control. Besides oncological outcomes, quality of life (QoL) after RP is a major issue. 3
Urinary continence (UC), an important indicator of QoL after RP, has a strong relationship with treatment satisfaction. 4 In open era, there were ∼30% of patients who still suffered from urinary incontinence at 1 year after RP. 5 With the development of laparoscopic technique, >80% of the patients have regained UC after laparoscopic RP. 6 Although the detailed pathophysiologic mechanism of urinary incontinence after RP is still unknown, UC recovery after RP could be influenced by some surgical factors, such as the injuries of nerve-vessel bundle (NVB), urinary sphincter, and pelvic floor musculature. In addition, some individual factors, such as age, diabetes, and prostate volume, can affect UC achievement. 7 –9
Post-prostatectomy UC (particularly early UC) has recently been improved based on the development of several surgical technique modifications, such as Retzius-sparing technique, distal urethral preservation, total anatomical reconstruction, puboprostatic ligament reconstruction, and bladder neck preservation (BNP). 10 –16 BNP has been applied to protect the circular muscle fibers of bladder neck. However, in some cases, especially those with advanced prostate cancer, BNP technique could lead to high probability of positive surgical margins. 17 Furthermore, Tyson and colleagues demonstrated that a small bladder neck could not facilitate the early recovery of continence after RP, but increased the risk of positive margins at the bladder neck. 18
During laparoscopic RP, a large bladder opening after prostate removal is occasionally inevitable, which brings about the mismatch between the bladder neck and urethra. At our center, three reconstruction methods, zero o'clock reconstruction (ZOR), six o'clock reconstruction (SOR), and three/nine o'clock reconstruction (T/NOR) techniques, were performed during vesicourethral anastomosis in cases with large bladder opening. This retrospective study described these three reconstruction techniques during laparoscopic RP and compared their surgical outcomes and post-prostatectomy continence in a consecutive series of patients who did or did not undergo these reconstruction techniques.
Patients and Methods
Patient selection
A consecutive series of patients (n = 121) with organ-confined prostate cancer underwent laparoscopic RP by one surgeon from March 2018 to December 2018. All patients underwent multiparameter MRI to estimate the clinical stage before operation and were followed up for at least 6 months. Inclusion criteria included the following: (1) localized prostate cancer (cT1–T3a, N0, M0) and (2) without urinary incontinence before operation. Exclusion criteria were (1) receiving radiotherapy before or after operation or (2) having history of previous prostate surgery. Eligible patients provided written informed consent form approved by the institutional review board of our hospital.
Surgical techniques
Laparoscopic RP was performed in all cases using the transperitoneal–anterior approach, similar to that described by Hasan and Gill. 19 Briefly, patients were anesthetized (general) and placed in a Trendelenburg position. Five trocars were applied in a classical fan configuration. The parietal peritoneum of the abdominal cavity was incised to access the retropubic space. Then, the endopelvic fascia was incised, prostate apex was outlined, and deep venous complex (DVC) was sutured using 2/0 barbed sutures. Bladder neck dissection was then started according to the boundary of the prostate tissue and circular muscle fiber of the bladder neck. The retrotrigonal fascia was dissected to approach the retrotrigonal space, where seminal vesicles were identified and dissected. Then, the Denonvilliers' fascia was incised to enter the pre-rectal space.
The NVBs in the lateral prostatic pedicle were identified and released by a combination of hem-o-lock and harmonic scalp. DVC, prostate apex, and distal urethra dissections were performed sequentially. After prostate removal, vesicourethral anastomosis was accomplished by double-needled barbed suture from the posterior aspect with or without the bladder neck reconstruction (BNR). Then, anterior suspension was performed by running suture from the anterior bladder wall to the dissected periurethral tissue. Pelvic lymph node dissection (PLND) was performed in moderate- or high-risk prostate cancer patients.
ZOR technique
In this technique, vesicourethral anastomosis was performed first from dorsal to ventral part (Fig. 1). The remaining part of the bladder neck anterior to the anastomotic stoma was closed by a 3/0 barbed running suture.
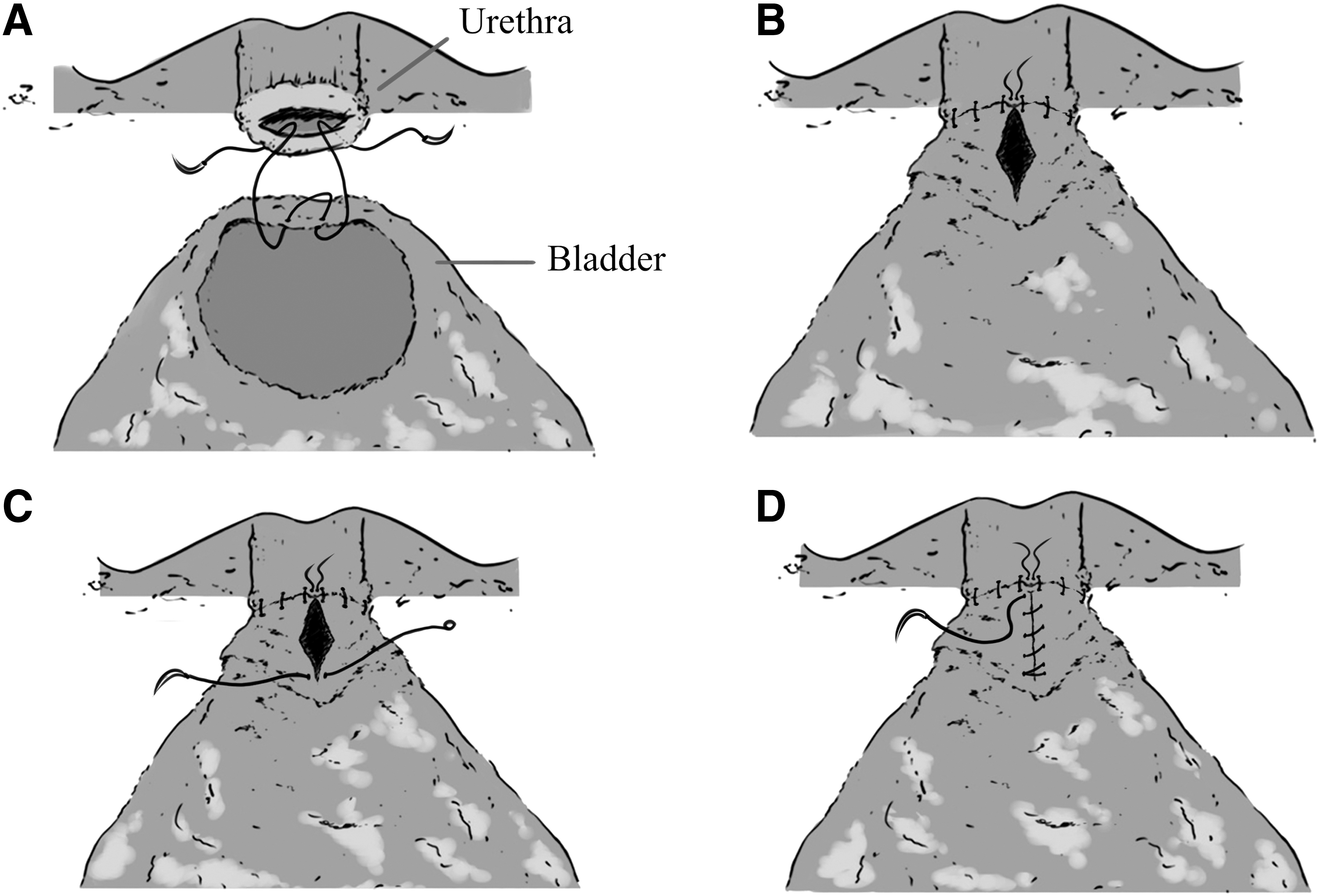
The procedure of zero o'clock reconstruction technique: vesicourethral anastomosis was performed first from dorsal to ventral part, and then the remaining part of the bladder neck anterior to the anastomotic stoma was closed by running suture.
SOR technique
The bladder neck was reconstructed using a 3/0 barbed running suture from the posterior part (close to trigonal part) to the anterior part of the neck (Fig. 2). The reconstructed bladder neck should be suitable for the size of the urethra. Vesicourethral anastomosis was then performed from the posterior part of the newly reconstructed bladder neck.
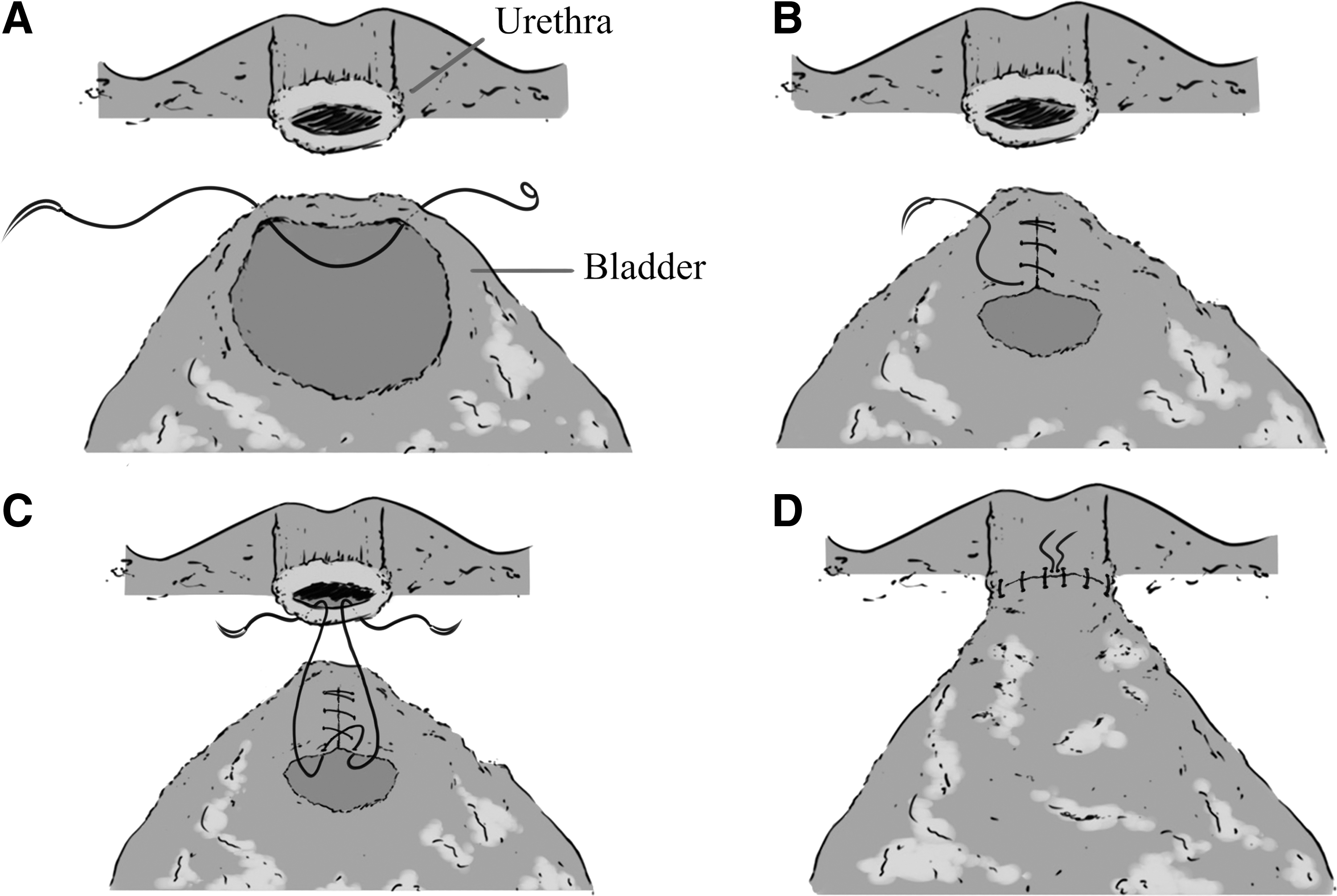
The procedure of six o'clock reconstruction technique: the bladder neck was reconstructed from the posterior part of the neck (close to trigonal part) to the anterior part before vesicourethral anastomosis.
T/NOR technique
This technique was started from the bilateral part of the bladder neck (3 and 9 o'clock) to the median (Fig. 3). The reconstructed bladder neck had a fish-mouth shape, suitable for the size of the urethra. Anastomosis was performed from the posterior part of the reconstructed bladder neck.
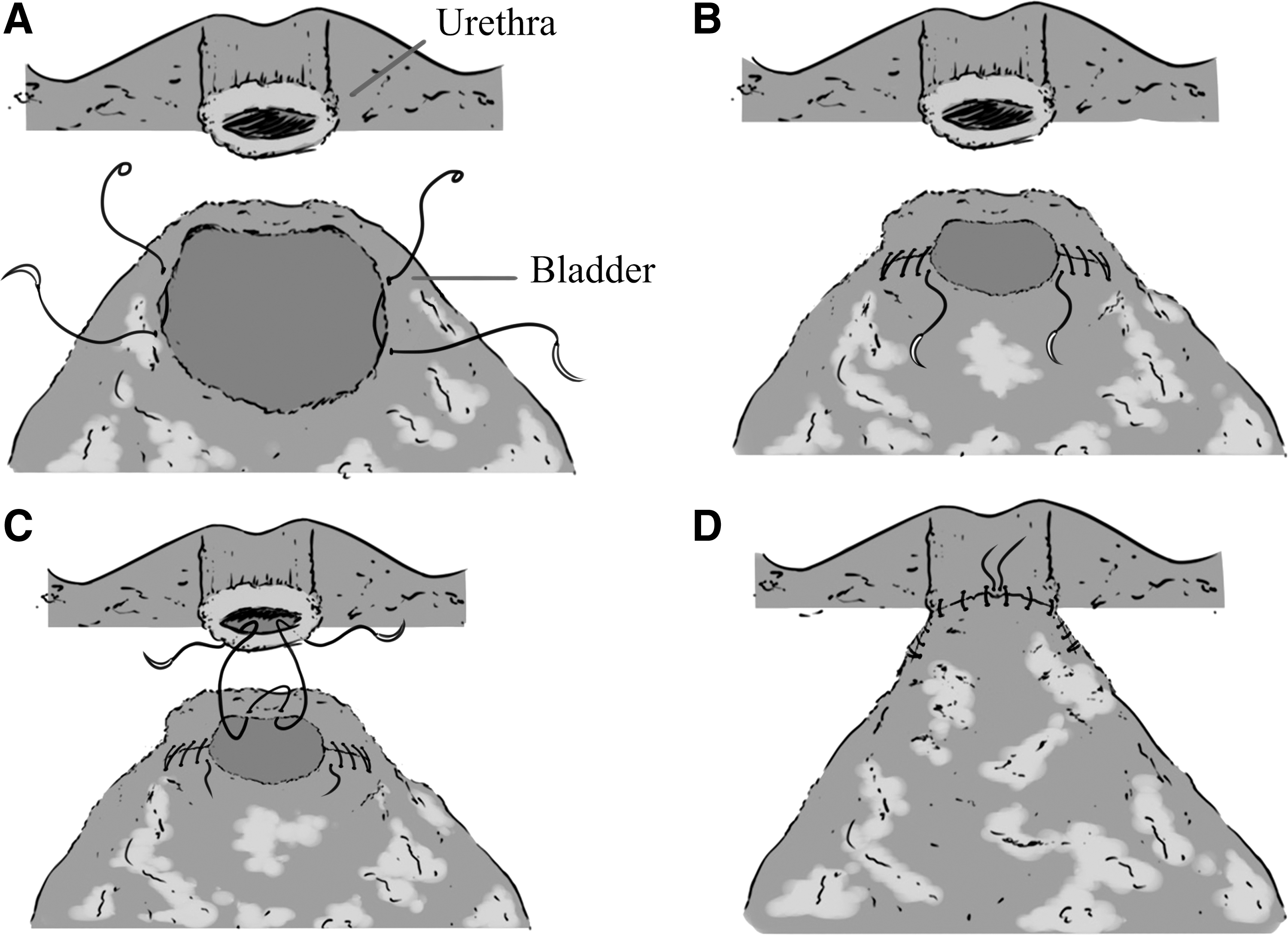
The procedure of three/nine o'clock reconstruction technique: the reconstruction was started from the bilateral part of the bladder neck (3 o'clock and 9 o'clock) to the median before vesicourethral anastomosis. The reconstructed bladder neck had a fish-mouth shape and was suitable for the size of the urethra.
Assignment to procedure methods
Vesicourethral anastomosis was performed directly when the bladder neck was suitable for the size of the urethra. BNR techniques, including ZOR, SOR and T/NOR techniques, were performed in cases with mismatch between the bladder neck and urethra. Cases with high-tension anastomosis or close proximity of the ureteral openings and bladder neck margin were performed by SOR technique, otherwise they would be performed by ZOR technique. Those with irregular shape of bladder neck attributable to asymmetric prostate lobes were introduced in the T/NOR group. Of note, the choices of different BNR technique could be flexible, partially depending on individual experience of the surgeon.
Data collection and follow-up
Preoperative data, including age, body mass index (BMI), diabetes status, hypertension status, prostate-specific antigen (PSA) level, D'Amico score, and prostate volume estimated by MRI, were collected. Intraoperative variables included estimated blood loss (EBL), operative time, anastomosis time (including reconstruction and vesicourethral anastomosis), type of reconstruction techniques, PLND rate, and blood transfusion rate. Postoperatively, several variables were collected, including catheterization duration, surgical complications (according to Clavien–Dindo system 20 ), and pathologic results (Gleason's score and surgical margin status).
Postoperative UC was assessed in each patient at 24 hours and at 1, 3, and 6 months after catheter removal. UC was evaluated based on the Expanded Prostate Cancer Index Composite Urinary Assessment. Patients were defined as continence if they were free from the use of a safety pad (0 pad/day).
Statistical analysis
Continuous variables were reported as mean and standard deviation, whereas categorical variables were reported as numbers and percentage. Pearson's chi-square and one-way analysis of variance tests were performed to analyze the differences of these variables between subgroups. To estimate the predicted factors of postoperative UC recovery, logistic regression analysis was applied for univariable and multivariable analyses. All data analyses were performed using SPSS 22.0 statistical software (IBM SPSS, Chicago, IL). p-Value <0.05 was considered statistically significant.
Results
Basic information and perioperative data of all patients are shown in Table 1. The mean age was 70.6 years, with mean BMI of 24.3 kg/m2. There were 21 (17.4%) and 62 (51.2%) patients with diabetes and hypertension, respectively. The mean serum PSA level at diagnosis was 26.5 ng/mL (5.3–240.2 ng/mL), and the mean prostate volume was 40.1 mL. According to the D'Amico risk classification, 3.3%, 44.6%, and 52.1% of patients were defined as low, middle, and high risk, respectively. Laparoscopic RP was performed in each patient, and 117 (96.7%) patients underwent PLND. The mean operation time was 145.3 minutes, and the mean anastomosis time (including the procedure of reconstruction and anastomosis) was 35.5 minutes. During the operation, the mean EBL was 190.3 mL, and 4 (3.3%) patients received blood transfusion.
Baseline Characteristics and Perioperative Outcomes
Bold values indicate p-values < 0.05.
BMI = body mass index; BNP = bladder neck preservation; EBL = estimated blood loss; PLND = pelvic lymph node dissection; PSA = prostate-specific antigen; SD = standard deviation; SOR = six o'clock reconstruction; T/NOR = three/nine o'clock reconstruction; ZOR = zero o'clock reconstruction.
After the operation, urine leakage occurred in three patients, with no surgical intervention (Clavien–Dindo grade 1). One patient suffered from posterior urethral obstruction because of posterior urethral stone formation and received lithotriptoscopy under general anesthesia (Clavien–Dindo grade 3b). The mean time of catheterization was 14.9 days.
Pathologic results revealed prostate adenocarcinoma in all patients. Negative surgical margin occurred in 69 (57.0%) patients, and 4 (3.3%), 33 (27.3%), and 15 (12.4%) patients had positive bladder neck margin, apical margin, and both bladder neck and apical margin, respectively. Follow-up data showed that 41 (33.9%), 64 (52.9%), 77 (63.6%), and 97 (80.2%) patients were continent at 24 hours, 1 month, 3 months, and 6 months after urine catheter removal, respectively.
We performed BNP in 37 (30.6%) patients, and BNR in 84 (69.4%) patients, of which 35 (28.9%), 34 (28.1%), and 15 (12.4%) patients underwent ZOR, SOR, and T/NOR, respectively. There was no significant difference among these four groups in terms of age, BMI, diabetes, hypertension, serum PSA level, Gleason's score, blood transfusion, postoperative complications, and continence recovery rate at 24 hours, 1 month, 3 months, and 6 months after catheter removal.
Based on D'Amico risk score, there were more high-risk patients in BNR groups (p = 0.009). Compared to the BNP group, patients in the reconstruction groups tend to have more pathologic results of positive apical margin, positive bladder neck margin, or both (p = 0.02). Prostate volume was larger in the reconstruction groups, particularly in the SOR group (p = 0.000). Similarly, operation time and anastomosis time were longer in the reconstruction groups than in the BNP group (p = 0.044 and p = 0.000 for operation time and anastomosis time, respectively). EBL was high in the BNR groups, peaking in the SOR group (p = 0.003). Catheter removal time was longer in the SOR and T/NOR groups (p = 0.002).
On multivariable logistic regression analysis, positive apical margin (p = 0.002) and long anastomosis time (p = 0.011) were independent adverse predictors of continence recovery rate in 24 hours. For continence recovery rates at 1, 3, and 6 months, positive apical margin (p = 0.000, p = 0.004, and p = 0.009 for 1, 3, and 6 months, respectively) and large prostate volume (p = 0.006, p = 0.005, and p = 0.002 for 1, 3, and 6 months, respectively) were adverse factors (Table 2).
Logistic Regression Analysis of Postoperative Continence
Bold values indicate p-values < 0.05.
CI = confidence interval; OR = odds ratio.
Discussion
UC is considered an essential issue in RP recovery, 21 which affects QoL postoperatively. Several technical modifications, such as BNP, have been attempted to achieve better UC recovery. In a randomized trial, BNP was proved to be associated with improved continence at 3 and 6 months. 22 In our study, BNP was applied in 37 (30.6%) patients, of whom 40.5%, 54.1%, 64.9%, and 81.1% were continent at 24 hours and 1, 3, and 6 months after catheter removal. BNP has the advantage of keeping bladder neck tissues intact, including striated and smooth muscle fibers. 23
However, a large bladder opening after prostate removal is occasionally inevitable, and as mentioned above, reconstruction techniques are wise choices when encountering the anastomosis mismatch. At our center, three types of BNR techniques are performed, which have been previously described. Based on our results, prostate volume, apical margin status, and anastomosis time were considered independent predictors of postoperative continence recovery rate, instead of the type of BNR technique itself.
ZOR technique, also called anterior reconstruction, was performed after vesicourethral anastomosis. Therefore, the advantage of this technique is that precise suture of the posterior wall of bladder neck and urethra can be promised, and the incidence of urine leakage is decreased, which was verified by our study. The mean prostate volume in the ZOR group was 37.1 mL, a little larger than the BNP group and significantly smaller than the SOR group.
Relatively large prostate volume could lead to high suture tension in anastomosis and close proximity of the ureteral openings and bladder neck margin, which is the indication of SOR technique. In this technique, reconstruction is performed from the posterior wall of the bladder neck before anastomosis, and therefore, bilateral ureteral opening could be protected during the procedure. As a result, it can reduce the risk of ureteral opening injury during anastomosis. Furthermore, SOR can facilitate anastomosis by decreasing suture tension. However, because of the reconstructive suturing on the posterior wall of the bladder neck, this procedure could lead to an inaccurate suture of the posterior wall of the bladder neck and urethra during anastomosis. There were two patients in this group who suffered from urine leakage after operation.
T/NOR was started from the lateral sides of the bladder neck, which could keep the reconstructed bladder neck anatomically in situ. However, it was time-consuming. In this study, the mean anastomosis time of T/NOR was 43.1 minutes, longer compared with BNP and other two reconstruction methods.
Poon and colleagues demonstrated that in open RP, no significant difference was found in UC recovery with BNP compared with BNR. 24 We obtained similar results in laparoscopic RP. Based on multivariable regression analysis, there was no significant difference in continence recovery rate between BNP and three different reconstruction techniques.
Positive apical margin played an important role in continence recovery rate at any time spot. Prostate apex is located in deep position of the pelvic and closely connects to the rhabdosphincter, nerve-vessel bundle (NVB), and muscles on the pelvic floor. 25 The fibers of the external urethral sphincter surround the urethra near the prostate apex and play an important role in UC. 26
First, positive apical margin probably implied that the prostate tumor could have invaded into the external urethral sphincter, influencing postoperative continence. Second, a positive apical margin could force the surgeon to perform extended resection around the prostate apex, resulting in damage to the external urethral sphincter and pelvic floor muscles, such as levator ani. Third, a positive apical margin might be accompanied by shorter length of functional urethra, the part in the range of 1.4 to 2.5 cm intraprostatically between the apex of the prostate and the colliculus seminalis. 26 In previous studies, a longer functional urethra resulted in substantially increased early UC results. 27 Therefore, a positive apical margin could lead to reverse continence recovery.
Skolarus and colleagues retrospectively demonstrated that the recovery of continence in patients with larger prostates (>100 g) was delayed compared with those with smaller prostates (<50 g) in 3 months. 28 However, several retrospective studies indicated that there was no significant correlation between prostate volume and 1-year continence recovery. 29,30 In this study, prostate volume was analyzed as a continuous variable and appeared to be an independent factor of postoperative continence at 1, 3, and 6 months.
In addition, anastomosis time was discovered to be related with continence recovery at 24 hours, which was not reported in other studies. We hypothesized that long anastomosis time could be accompanied by large prostate volume or result in more injuries to pelvic floor muscles and tissues surrounding the urethra, leading to decreased continence recovery. However, more studies were needed to clarify this result.
We described three different BNR techniques that were demonstrated to be equivalent in postoperative continence recovery to the BNP technique. However, our study is not free of any limitation. First, this was a single-center retrospective analysis, and if possible, prospective randomized clinic trials should be performed. Second, there was a selective bias. For example, the larger the prostate volume was, the more was the possibility that we choose to perform SOR. There was a lack of homogeneity between these different reconstruction groups, and it is difficult to compare the different reconstructions. Third, a longer follow-up period is needed in further studies.
Conclusion
The three different kinds of BNR techniques were safe and feasible in laparoscopic RP and had no different impact on continence recovery. Positive apical margin, large prostate volume, and long anastomosis time were independent adverse predictors of continence.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.