
Abstract
Objectives:
To compare direct ureteral length measurements with predictive formulas used for the preoperative assessment of ureteral length, and to evaluate patient factors that impact the accuracy of these predictive formulas.
Methods:
Patients undergoing ureteral stenting for benign and malignant indications were included. Clinical factors analyzed were gender, race, height, weight, prior abdominal or pelvic surgery, radiation therapy, pelvic organ prolapse (POP), laterality, hydronephrosis, and pre-existing ureteral stent. Three predictive formulas and a common height-based formula were used. Direct ureteral measurements were obtained with a ruled 5F ureteral catheter. Predictive formulas were compared with direct ureteral measurements using scatterplot and Spearman's correlation coefficient. Univariate and multivariate logistic regressions were used to evaluate patient factors associated with ≥2 cm deviation from direct ureteral measurements.
Results:
A total of 108 patients (134 ureters) were analyzed. All predictive formulas correlated poorly with direct ureteral measurements, although as much as 60% of ureteral stent lengths were accurately predicted. Several patient factors significantly impacted accuracy of formulas: male gender (p = 0.04), POP (p = 0.05), body mass index (BMI) ≥25 (p = 0.03), and pre-existing ureteral stent (p = 0.05).
Conclusion:
Our study suggests that predictive formulas for ureteral stent length have poor accuracy when compared to direct measurement, especially for patients with elevated BMI and POP. Our institution considers direct ureteral measurement the gold standard for determining ureteral stent length—a method that is universally applicable and independent of patient factors.
Introduction
Ureteral stenting to relieve or prevent ureteral obstruction is fundamental to numerous urologic procedures for the treatment of renal calculi, ureteral strictures, retroperitoneal fibrosis, malignancies, and various other pathologies. Since first described by Zimskind and colleagues in 1967, the ureteral stent has evolved from a straight catheter externalized through the urethra to the modern-day, internalized double pigtail stent. 1 Despite design advances, complications and morbidity as consequence of improper stent sizing still occur.
The generally accepted “ideal” stent length entails a full proximal curl in the renal pelvis and distal curl in the bladder, but not crossing mid-trigone. 2,3 Too short a stent increases risk of migration and need for retraction and replacement, 4,5 whereas too long a stent can cause symptoms of trigonal irritation, although the exact association between stent length and symptoms has been debated. Several studies found longer stents crossing mid-trigone were significantly associated with higher rates of urinary urgency, frequency, incontinence, dysuria, bladder pain, and worse quality of life. 3,6,7 However, other studies found no association between stent length and symptoms. 8,9 Nevertheless, proper sizing can prevent stent migration and allay concerns for stent-related morbidity.
To optimize stent length, predictive formulas to preoperatively assess ureteral length have been developed. Studies have reported excellent to near perfect correlation between predictive formula estimates and direct ureteral measurement. 10 –12 Herein we compared three predictive formulas with direct measurement, the gold standard at our institution, and evaluated for patient factors that impact their accuracy.
Methods
Institutional review board permission was obtained for this single-center, retrospective review of prospectively collected data for patients 18 years of age or older, who underwent ureteral stent placement at a tertiary care hospital. Indications for stent included renal calculi, retained stents, unspecified hydronephrosis, and genitourinary and pelvic malignancies. Patients with urinary diversions, pelvic or transplanted kidneys, were excluded. All patients underwent history and physical examination, laboratory tests, and CT of abdomen/pelvis ± intravenous contrast. Patient data included gender, age, height, weight, prior abdominal/pelvic surgery, prior abdominal/pelvic radiation therapy, and degree of pelvic organ prolapse (POP) based on the Pelvic Organ Prolapse Quantification System. 13 Procedural data included laterality, procedural indication, pre-existing stent, and degree of hydronephrosis. 14 Degree of hydronephrosis was determined intraoperatively at the time of stent placement to reflect patient's current condition and obviate time lags between prior imaging and intervention.
Patients underwent general anesthesia and received perioperative antibiotics. Procedures were performed in a specialty endourologic operating room equipped with fluoroscopy. Direct ureteral measurements were obtained with an Open-End Flexi-Tip 5F ureteral catheter (Cook Medical, Bloomington, IN). Previously placed stents were removed before retrograde pyelography (RPGs). A low-pressure RPG to identify anatomy was performed using a 22F rigid cystoscope and diluted contrast. The ureteral catheter was advanced over a guidewire to the ureteropelvic junction (UPJ) under cystoscopic and fluoroscopic visualization. In cases where the renal pelvis and proximal ureter did not form a discrete insertion, an adapted methodology described by Gupta and colleagues was used to determine UPJ (Fig. 1). 15 Positional variations of the ureteral catheter were observed during breathing, but did not ultimately affect the length of stent placed. After measurement, a fixed-length stent was placed through the port under cystoscopic and fluoroscopic visualization.
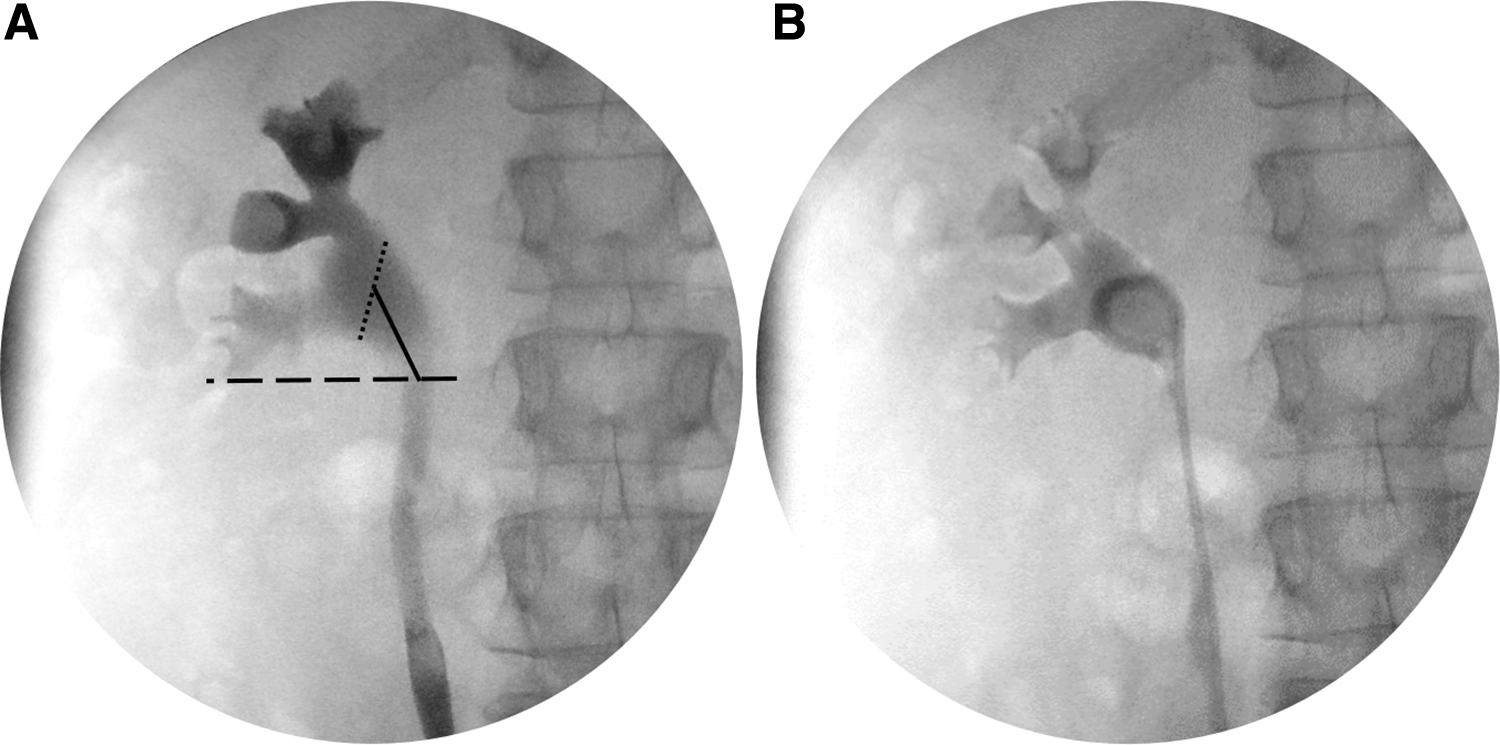
Determination of UPJ on RPG.
Original studies were reviewed after performing a literature search using words, including “ureteral stent length,” “predictive formula,” and “direct ureteral measurement.” Three predictive formulas were selected based on reproducibility and correlation with direct ureteral measurements. Table 1 summarizes parameters for formulas: PFCLIN used physical anthropometric variables that correlated most with ureteral length; PFRADIO adjusted CT measurements to account for normal ureteral anatomy; PFCOMBO used a combination of anthropometric and radiographic measurements that correlated most with ureteral length; and PFHEIGHT was based exclusively on height and has been used at our institution outside of this study when direct measurement was not practical, such as when using a flexible cystoscope. 10 –12
Predictive Formulas for Determination of Length of Stent Indicated
CT images in the coronal plane were used in lieu of intravenous urography (IVU). 12
UPJ = ureteropelvic junction; UVJ = ureterovesical junction.
Descriptive analysis and statistics were performed with R Statistical Software version 3.5.1 (R Foundation for Statistical Computin, Vienna, Austria). Quantitative data analysis was performed using Spearman's correlation coefficient to evaluate strength of correlation between predictive formula estimates and direct measurements. Univariate and multivariate logistic regression analyses were performed to evaluate patient factors associated with ≥2 cm deviation from direct measurement. A threshold of 2 cm was used because most standard ureteral stents are available in 2 cm increments.
Results
A total of 108 patients (134 ureters) were included in the study, comprising 56 males (52%) and 52 females (48%). Median age was 50 years (range 19–88), height 171 cm (range 152–191), weight 89 kg (range 45–212), and body mass index (BMI) 30 (range 15.5–77.7). Racial breakdown of patients included 90% (97/108) white, 6% (7/108) black, 1% (1/108) Asian, and 3% (3/108) other. Fifty-six percent (60/108) of patients had prior abdominal/pelvic surgery, and 4% (4/108) of patients had prior abdominal/pelvic radiation therapy. A total of 29 patients had POP: 14% (15/108) stage I, 7% (8/108) stage II, 5% (5/108) stage III, and 1% (1/108) stage IV.
Left and right ureters constituted 61% (82/134) and 39% (52/134) of cases, respectively. Indications for ureteral stenting included 38% (51/134) of patients with only renal stone(s), 50% (67/134) with ureteral stone(s) with or without renal stones, 3% (4/134) with a retained stent, 7% (9/134) with unspecified hydronephrosis, and 2% (3/134) with urothelial carcinoma. Twenty-nine percent (39/134) of ureters had pre-existing stents and underwent direct measurement for stent exchange. Sixty-three renal units had hydronephrosis: 19% (26/134) grade I, 16% (22/134) grade II, 7% (9/134) grade III, and 4% (6/134) grade IV.
Scatterplots revealed poor correlation between predictive formulas and direct ureteral measurements (Fig. 2). Spearman's correlation coefficient for PFRADIO 0.055 (p = 0.53), PFCOMBO 0.01 (p = 0.91), PFHEIGHT −0.011 (p = 0.9), and PFCLIN −0.91 (p = 0.53). On univariate and multivariate logistic regression analyses, patients with BMI ≥25 were as much as 22 times more likely to be inaccurate with PFCOMBO when compared to direct measurement. Patients with POP were as much as three times more likely to be inaccurate with PFRADIO and PFHEIGHT. Males were as much as 17.3 times more likely to be to be inaccurate with PFRADIO, although 52% less likely to be inaccurate with PFHEIGHT. Patients with pre-existing stents were as much as 85% less likely to be inaccurate with PFCOMBO. Other factors that were not significant included race, prior abdominal or pelvic surgery, prior abdominal or pelvic radiation, hydronephrosis, or laterality (Table 2).

Correlation between predictive formulas and direct ureteral measurement using scatterplot and Spearman's correlation coefficients (r).
Patient Factors That Were Significantly Associated with ≥2 cm Deviation Between Predictive Formula Estimates and Direct Ureteral Measurement on Univariate and Multivariate Logistic Regressions
BMI = body mass index; POP = pelvic organ prolapsed.
Since the impact of oversized ureteral stents is controversial, we also limited univariate and multivariate logistic regression analyses to only stents that were ≥2 cm too short when compared to direct measurement. Overall, the same patient factors were found to similarly impact predictive formulas: BMI ≥25, POP, male gender, and prestented ureters (Table 3). Findings did not drastically change when limiting scope of analyses because majority of deviations for PFRADIO, PFCOMBO, and PFHEIGHT had underestimated stent length (Fig. 3).
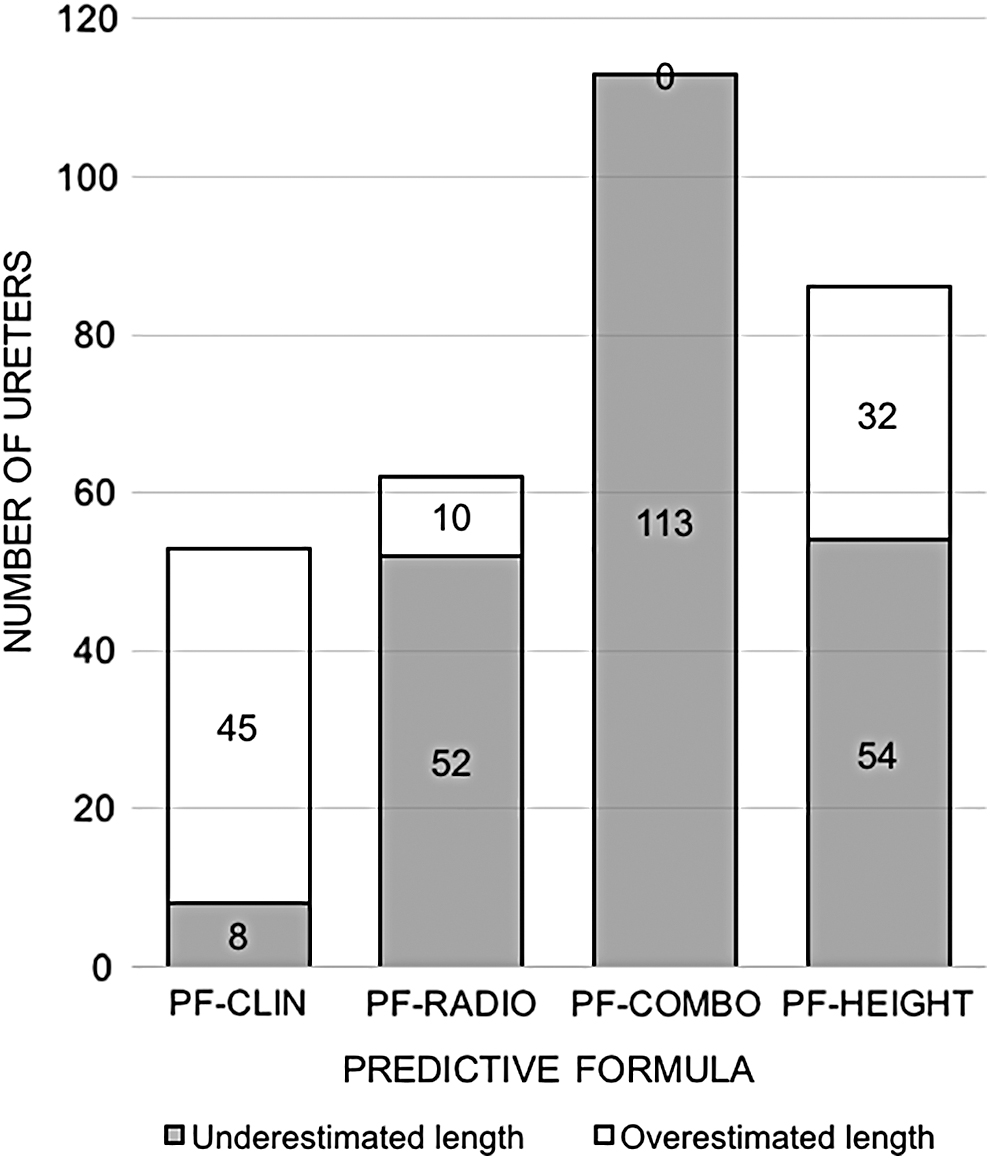
Number of deviations from direct ureteral measurement for each predictive formula, further categorized by underestimations and overestimations.
Patient Factors That Were Significantly Associated with ≥2 cm Underestimation by Predictive Formula When Compared to Direct Ureteral Measurement on Univariate and Multivariate Logistic Regressions
Discussion
Ureteral stents have become widely used as a temporary or permanent measure for urinary drainage in cases of renal calculi, ureteral strictures, malignancies, urologic reconstructions, and complications arising from other procedures. However, improper stent sizing can lead to stent migration and exacerbation of stent-related symptoms. 3,6,7 As such, proper attention to accurate stent sizing is of importance.
Despite the frequent use of ureteral stents, there is no standard method for determining optimal stent length. Several formulas for predicting ureteral length are available, but have varying degrees of simplicity, convenience, and accuracy. Perhaps, the most commonly used patient factor for prediction is height, which stems from architect Marcus Vitruvius' theory that the human body is a model of natural, proportional perfection. Pilcher and Patel were among the first to describe a predictive formula for ureteral length based on height. 2 Our study used a modified formula, PFHEIGHT, which accurately predicted only 36% (48/134) of ureteral lengths when compared to direct measurement. Applying Pilcher and Patel's original formula to our study group accurately predicted ureteral length in even fewer cases, 14% (19/134). 2 Multiple studies corroborate our low rates of accuracy and poor correlation between height and ureteral length on statistical analyses (Spearman's correlation coefficient 0.06, p = 0.5). 10 –12 Despite this, height is still commonly incorporated into many formulas.
In addition to patient height, correlation between other anthropometric measurements and ureteral length has been studied. Hruby et al. found that weight, distance from xiphoid to pubis, and distance from shoulder to head of ulna correlated with ureteral length. 10 In our study, we found a similar degree of correlation between weight and direct measurement (Spearman's correlation coefficient 0.20, p = 0.02). We also found that predictive formula estimates for patients with BMI ≥25 were 22 times more likely to be inaccurate with PFCOMBO when compared to direct measurements, further suggesting an association between weight and ureteral length.
There is no literature to our knowledge regarding the impact of weight on ureteral length. However, there is evidence that higher a BMI displaces the base of the sacrum anteriorly, leading to an increasing degree of pelvic tilt. 16 We hypothesize that lumbar hyperlordosis may distort and exaggerate the natural ureter course as it passes over the sacral promontory and lower margin of the sacroiliac joint. In support of this hypothesis, 100% (90/90) of ureters in patients with BMI ≥25 were underestimated in length by PFCOMBO. PFCOMBO did not adjust for weight and only accounted for ureteral length measured in axial and coronal CT-imaging planes, thus neglecting additional ureteral length from lumbar hyperlordosis in the third, sagittal, plane.
Furthermore, patients with POP made predictive formula estimates three times more likely to be inaccurate with PFRADIO and PFHEIGHT when compared to direct measurements. As the uterus descends into the vagina, the downward traction placed on the cardinal ligaments can cause distal ureters to descend as well. In patients undergoing vaginal hysterectomies for uterine prolapse, DeLancey and coworkers found 1 cm of ureteral descent for every 3 cm of cervical descent. 17 Bladder prolapse alone can also cause similar downward traction on distal ureters as captured on cystography and doppler ultrasonography by Minagawa and coworkers 18 Severe cases of POP have even led to ureteral obstruction, hydronephrosis, and renal dysfunction from profound distortion and kinking of ureters. 19 In our patients with prior hysterectomies, 59% (16/27) still had some degree of POP. Posthysterectomy patients with POP had higher rates of inaccuracy than posthysterectomy patients without POP, 56% (9/16) vs 18% (2/11), respectively (p = 0.05). This suggests ureteral effects are persistent after hysterectomy or develop from bladder prolapse alone. Although the degree of ureteral distortion is likely dependent on POP severity, the different POP stages were not further evaluated because of small sample size.
Patient gender and pre-existing ureteral stents were also found to significantly impact predictive formula estimates, but their specific influences are less evident. The studies for PFCLIN and PFCOMBO found that gender correlated with ureteral length on multilinear and multivariate regression analyses, which is reflected by their gender-specific adjustment factors. 10,12 Although we found a significant difference between male and female mean ureteral lengths (±standard deviation), 25.57 cm (±1.83) and 26.6 cm (±2.48), respectively (p = 0.007), the impacts of patient gender on predictive formulas are unclear and confounded by the different methodologies and study populations. In contrast, a cadaveric study as per Novaes and colleagues found no difference between male and female mean ureteral lengths. 20 We also did not examine effects of “fish-hook” ureteral configuration from prostatic enlargement in men. 21
Prestented ureters made PFCOMBO 85% less likely to be inaccurate. We hypothesized that decompression of a dilated collecting system decreases ureteral tortuosity and redundancy, leading to improved accuracy of predictive formulas. However, we were unable to provide further insight as 65% (22/34) of prestented ureters in our study had residual hydronephrosis. Ideally, we would compare accuracy from before the initial ureteral stent placement to when the present stent was replaced. However, not all patients had prestent imaging available to review. We were also unable to use the length of pre-existing stents as a surrogate for direct measurement because we could not differentiate whether suboptimal proximal and distal curl positions were attributable to changes in the collecting system after decompression or if a pre-existing stent was inappropriately sized at the time of initial placement.
In contrast to their original studies, the three predictive formulas did not correlate highly with direct ureteral measurements when applied to our study group. The poor correlation may be secondary to our inclusion of females, patients with POP, and patients with tortuous ureters or severe hydronephrosis, which were excluded in some studies. We purposefully included these patients as they comprise a substantial portion of patients who require a stent, therefore allowing us to examine generalizability and the effects of aberrant patient factors. Despite the poor correlation between measured ureteral length and predictive formulas, as much as 60% of ureteral lengths were accurately predicted, supporting the utility of predictive formulas in practice.
Direct ureteral measurement continues to be the gold standard at our institution. We acknowledge there are limitations inherent to direct measurement, which is performed when the patient is stationary in lithotomy position and physiologic processes such as bladder and tidal volumes are strictly controlled. This artificial environment does not represent the dynamic nature of reality, but offers acceptable outcomes. In our study group, there were no undersized stents and only 9% (12/134) of stents were oversized with the distal curl past mid-trigone based on intraoperative cystoscopic and fluoroscopic assessment. Postprocedural imaging was not routinely obtained; however, there were no complications of stent migration or need for replacement because of length discrepancy. Stent-related symptoms were not evaluated, given the contradictory evidence in the literature, which suggests a number of parameters beyond stent length serve as confounding factors. 3,6 –9
Moving forward, the significant inaccuracy of our own PFHEIGHT formula has inspired alternative methods for direct measurement, such as placing the guidewire and ureteral catheter alongside the flexible cystoscope instead of through the port or investing in longer ureteral catheters to accommodate endoscopic instruments of varying lengths. Future areas of research may include evaluating effects of patient positioning (i.e., lying, sitting, and standing) on ureteral length to better understand stent movement in situ and stent-related symptoms when patients resume normal activity. In addition, further research on multicoil or variable-length stents as a means to mitigate sizing issues associated with fixed-length stents could enhance the limited data available on clinical experiences.
Conclusion
The idea of a simple and convenient predictive formula to preoperatively assess ureteral length is attractive for optimizing stent sizing and efficiency in the operating room. However, a single predictive formula is unlikely to be universally applicable, given the complex nuances of patient factors as evidenced by our findings. Therefore, our institution considers direct ureteral measurement the gold standard for determining ureteral stent length—a method that is universally applicable and independent of patient factors. In situations where direct measurement is not feasible, predictive formulas can be useful when their limitations are understood. Our study demonstrated that predictive formulas were less likely to be accurate in patients with high BMI and POP, which is supported by this article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.