
Abstract
Introduction:
The peritoneal interposition flap (PIF) has been shown to prevent postoperative symptomatic lymphocele (SL) formation after robot-assisted radical prostatectomy (RARP) and pelvic lymph node dissection (PLND). The PIF inhibits the mobilized bladder from resealing over its lateral dissection planes, which overly the lymphadenectomy beds. This creates a window for lymphatic fluid to drain into the peritoneal cavity where it can be absorbed. Herein, we externally validate its utility in preventing postoperative SL formation and assess its effect on postoperative urinary function.
Materials and Methods:
We retrospectively reviewed all consecutive patients who underwent RARP with bilateral PLND by a single surgeon between July 2016 and September 2019. All patients who underwent surgery before August 8, 2018 did not receive the PIF, while those who underwent surgery after August 8, 2018 received the PIF. Our PIF technique involves fixing the peritoneum overlying the lateral dome of the bladder to the ipsilateral, anterior-lateral surface of the bladder using a barbed absorbable suture. Continuous and categorical variables were compared between the two groups using independent t-tests and chi-square tests, respectively; p < 0.05 was considered significant.
Results:
Of 318 total patients, 201 did not undergo the PIF and 117 underwent the PIF. With regard to postoperative complications, patients undergoing the PIF had a lower incidence of SL compared with those not undergoing the PIF (0.0% vs 6.0%, p = 0.007). There was no difference in 30-day postoperative nonlymphocele complications (Clavien >2) between both groups (p = 0.800). With regard to urinary function, there was no difference in the rate of 3-month postoperative continence (p = 0.624), preoperative American Urological Association Symptom Score (AUASS) (p = 0.898), and postoperative AUASS (p = 0.470) between both groups.
Conclusion:
Utilization of a PIF may minimize the risk of SL formation after RARP and PLND without increasing the risk of non-SL-related complications. This technique does not adversely affect postoperative urinary function.
Introduction
According to the American Urological Association, pelvic lymph node dissection (PLND) can be considered for patients with clinically localized prostate cancer undergoing robot-assisted radical prostatectomy (RARP), and is recommended for those with unfavorable intermediate-risk or high-risk disease. 1 PLND is the most effective method for assessing lymph node metastases in patients with clinically localized prostate cancer. 2,3 Improved staging of prostate cancer allows for better risk assessment of cancer progression after RARP and identification of patients who may benefit from adjuvant therapy. 2
Despite this, PLND may be associated with surgical complications, with postoperative lymphocele formation being the most common. 4 –6 Although most postoperative lymphoceles are clinically insignificant, symptomatic lymphoceles (SLs), which occur in 2% to 8% of patients after RARP and PLND, may be associated with significant morbidity and even mortality. 4 –6 Patients with SLs may present with fevers, lower abdominal pain, lower extremity pain and/or swelling, and/or lower urinary tract symptoms. Furthermore, compression of pelvic vasculature by lymphoceles may cause severe thromboembolic events, including deep vein thrombosis (DVT) and pulmonary embolism (PE). 7 –9
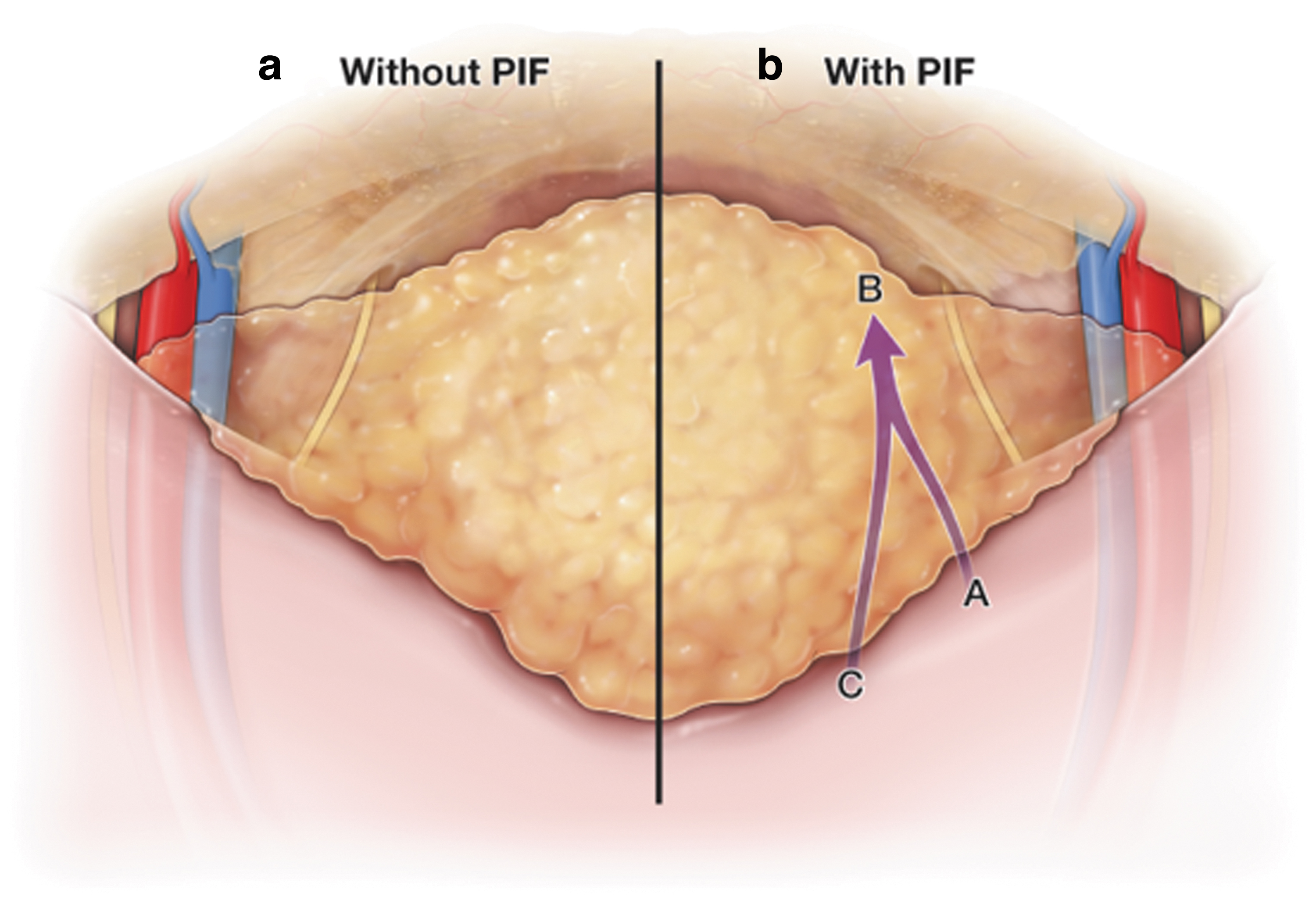
Lebeis and colleagues described the peritoneal interposition flap (PIF) and utilized it to prevent SL formation in 77 consecutive patients undergoing transperitoneal RARP with PLND. 10 The authors hypothesized that lymphoceles form after PLND when perivesical fat scars over the PLND bed and traps lymphatic fluid (Fig. 1). The PIF involves advancing a peritoneal surface between the lateral bladder and PLND bed to create an open channel between the PLND bed and peritoneal cavity, thus allowing for peritoneal reabsorption of lymphatic fluid. However, some authors have suggested that the PIF may potentially cause undue kinking of the bladder and postoperative micturition issues. 11 Herein, we externally validate the utility of the PIF in preventing SL after transperitoneal RARP with PLND in a larger patient cohort. Furthermore, we assess the effect of the PIF on postoperative urinary function.

This is a CT scan with intravenous contrast showing bilateral pelvic lymphocele formation in a patient who previously underwent RARP with bilateral PLND. Note that the bladder (B) forms the medial aspect (outlined) of the pelvic lymphoceles. We hypothesize that lymphoceles form after PLND and RARP because the perivesical fat scars over the lymphadenectomy bed and traps lymphatic fluid. PLND = pelvic lymph node dissection; RARP = robot-assisted radical prostatectomy.
Materials and Methods
We performed an Institutional Review Board approved, retrospective review of all consecutive patients who underwent anterior transperitoneal RARP and PLND by a single surgeon (D.D.E.) between July 2016 and September 2019. All consecutive patients who underwent surgery before August 8, 2018 did not receive the PIF, whereas all consecutive patients who underwent surgery after August 8, 2018 received the PIF. After grouping patients according to whether they received the PIF, perioperative outcomes were compared. Primary outcomes included SL, and American Urological Association Symptom Score (AUASS) and urinary continence at 3 months postoperatively. SL was defined as a lymphocele causing fever, abdominal pain, lower extremity pain and/or swelling, and/or lower urinary tract symptoms; and/or a lymphocele associated with a DVT and/or PE. Continence was defined as wearing 0 pads per day. Secondary outcomes included operative time and non-SL complications. All patients received one preoperative dose of 5000 units of subcutaneous heparin.
Aside from the PIF, our surgical technique for anterior transperitoneal RARP and PLND remained consistent throughout the study period. The decision to perform PLND was determined at time of RARP based on clinical history, preoperative imaging (when available), and intraoperative findings. When PLND was performed, it was performed bilaterally using a standard or extended template. We defined a standard template PLND as resection of the obturator and internal iliac nodal packets; and extended template PLND as resection of the obturator, internal iliac, perivesical and perirectal nodal packets. During PLND, a combination of electrocautery and absorbable Lapro-clips™ (Medtronic, Minneapolis) was utilized to seal lymphatic channels. An abdominal drain was not routinely placed at time of surgery.
Postoperative management of patients undergoing RARP and PLND remained consistent throughout the study period. All patients received 5000 units of subcutaneous heparin every 8 hours until discharge. Patients were assessed for clinical symptoms of SL at each postoperative visit. Patients with clinical symptoms of SL underwent CT scans of the abdomen and pelvis to confirm or rule out the diagnosis. Patients without clinical symptoms of SL did not undergo postoperative imaging.
Surgical technique
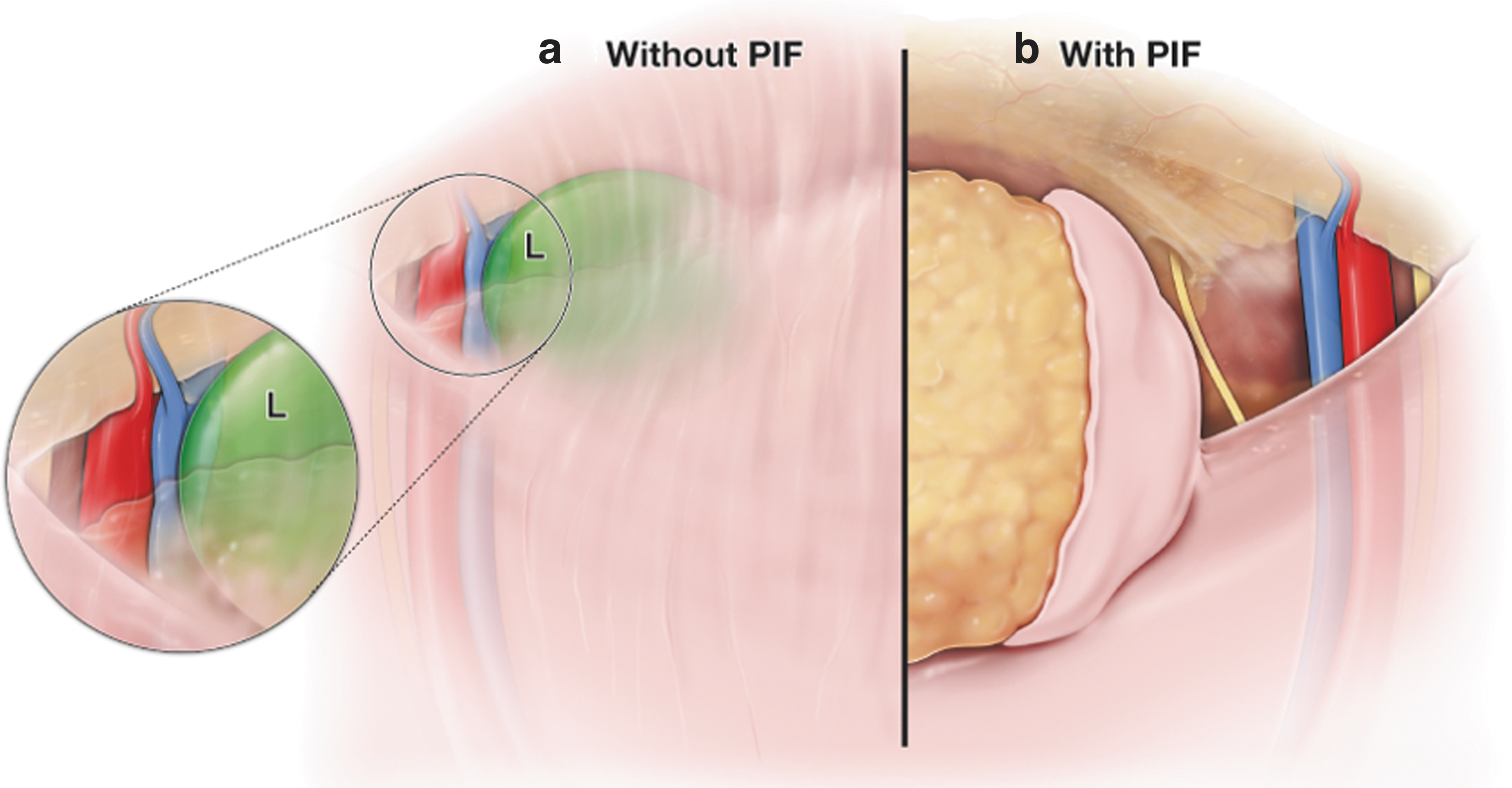
The PIF is performed after completing the RARP and bilateral PLND. Dropping the bladder from the anterior abdominal wall exposes the perivesical and preperitoneal fat, which can scar back over the PLND bed and subsequently trap lymphatic fluid. We focus our attention on the peritoneal lining of the perivesical and preperitoneal fat that was incised when dropping the bladder off the anterior abdominal wall (Fig. 2). Using a 3-0 V-Loc™ suture (Medtronic) the right-sided peritoneal lining of the perivesical and preperitoneal fat ∼6 cm from the lateral most cut edge is fixed to the right anterior-lateral bladder (Fig. 3). Care is taken to fix the peritoneal lining just anterior to the clips used to ligate the right prostatic pedicles. This landmark ensures that inadvertent injury to the right ureter is avoided. The 3-0 V-Loc is brought back through the peritoneal lining of the perivesical and preperitoneal fat ∼2 cm medial from the initial throw, and the PIF is secured in place using a Lapro-clip. This rotational eversion of the lateral peritoneal lining of the bladder prevents the lymphadenectomy bed from sealing off and results in a lymphatic drainage pathway from the right lateral gutter to the peritoneal cavity (Fig. 4). A similar technique is repeated on the left side.

This image shows the peritoneal lining (P) surrounding the posterior bladder (B), which was previously incised during RARP when dropping the bladder off the anterior abdominal wall. This peritoneum will be used to form the PIF. PIF = peritoneal interposition flap; RPW = right pelvic wall.
In this illustration, the bladder has been dropped from the anterior abdominal wall, and the perivesical and preperitoneal fat can be seen.
Statistical analysis
Continuous and categorical variables were compared using independent t-tests and two-tailed chi-square tests, respectively. Statistical analyses were conducted using IBM SPSS® Statistics 26 (IBM, Armonk); p < 0.05 was considered statistically significant.
Results
Of 318 consecutive patients who underwent RARP and bilateral PLND, 201 did not undergo the PIF and 117 underwent the PIF. A comparison of patient demographics and perioperative variables between the non-PIF group and PIF group is shown in Table 1. With regard to preoperative parameters, there was no difference in mean age (p = 0.123), body mass index (p = 0.314), and prostate-specific antigen level (p = 0.084). With regard to operative parameters, there was no difference in mean estimated blood loss (p = 0.245) and length of hospital stay (p = 0.381). Patients undergoing the PIF had a longer mean operative time compared with patients not undergoing the PIF (196.9 ± 53.4 minutes vs 178.5 ± 44.0 minutes, respectively; p = 0.022). Two of 117 (1.7%) patients in the PIF group and 4/201 (2.0%) patients in the non-PIF group had abdominal drains placed at time of surgery (p = 0.208). In addition, patients in the PIF group underwent a higher proportion of extended PLNDs vs patients in the non-PIF group (64.1% vs 39.3%, respectively; p = <0.001). There was no difference in number of lymph nodes removed between both groups (p = 0.999). With regard to pathologic variables, there was no difference in prostate volume (p = 0.339) and proportion of patients with grade group (GG)2 (p = 0.746), GG3 (p = 0.305), and GG ≥4 (p = 0.093) disease. There was a lower proportion of patients with GG1 disease in the PIF group compared with the non-PIF group (1.7% vs 13.4%, respectively; p = <0.001). With regard to follow-up, patients undergoing the PIF had a shorter mean follow-up compared with those not undergoing the PIF (7.0 ± 2.4 months vs 14.3 ± 8.5 months, respectively; p < 0.001).
Comparison of Patient Demographics and Perioperative Variables
GG = grade group; PIF = peritoneal interposition flap; PSA = prostate-specific antigen; SD = standard deviation.
A comparison of postoperative complications between the non-PIF group and PIF group is shown in Table 2. Patients undergoing the PIF had a lower incidence of SL formation compared with those not undergoing the PIF (0.0% vs 6.0%, respectively; p = 0.007). None of the patients undergoing the PIF developed SL, and all patients with SL did not receive the PIF. In the non-PIF group, median time to SL detection was 27.9 ± 13.1 days postoperatively. Of the 12 patients with SL, 2 (16.7%) were managed conservatively with pain control, close observation, and serial imaging; 10 (83.3%) required percutaneous aspiration and insertion of a chronic drain. Of the 10 patients who required percutaneous aspiration and insertion of a chronic drain, 3 (30.0%) required sclerotherapy. Also, of the 12 patients with SL, 2 (16.7%) developed lower extremity DVT requiring prolonged anticoagulation, 2 (16.7%) developed lower extremity DVT and PE requiring prolonged anticoagulation and inferior vena cava filter placement, and 2 (16.7%) developed infected lymphoceles requiring prolonged antibiotics. Of the four patients in the non-PIF group who had abdominal drains placed, 1 (25.0%) developed a SL. There was no difference in the rate of postoperative non-SL-related major complications (Clavien >2) between both groups (p = 0.800).
Comparison of Postoperative Complications
SL = symptomatic lymphoceles.
A comparison of postoperative urinary function between the non-PIF group and PIF group is shown in Table 3. There was no difference in 3-month postoperative continence rate between both groups (p = 0.624). Furthermore, there was no difference in mean preoperative (p = 0.898) and postoperative AUASS (p = 0.470) between both groups.
Comparison of Postoperative Urinary Function
AUASS = American Urological Association Symptom Score.
Discussion
SL is a relatively common complication after RARP and PLND, which may be associated with significant morbidity and even mortality. As such, various strategies to prevent SL formation in this setting have been described. Surgical clipping and bipolar coagulation of lymphatic vessels are common techniques used to prevent SL formation. In a prospective, randomized single-institution study, Grande and colleagues compared lymphocele rates after titanium clipping vs bipolar coagulation of lymphatic vessels after PLND during RARP. 12 The authors found that SL occurred regardless of whether titanium clipping or bipolar coagulation was utilized. Also, there was no difference in the rate of SL formation regardless of the technique utilized (5% vs 4%, respectively; p = 0.7). 12
Waldert and colleagues evaluated the role of injecting FLOSEAL® (Baxter International Incorporated, Deerfield), a bovine-derived gelatin matrix that is mixed before use with human-derived thrombin, into the lymphadenectomy bed of patients after undergoing extraperitoneal RARP and PLND. 13 The authors hypothesized that the hemostatic matrix may prevent SL by sealing open lymphatic channels, providing a local tamponade effect, and/or facilitating the formation of a fibrin clot. Although injection of FLOSEAL into the lymphadenectomy bed resulted in a lower rate of SL compared with when FLOSEAL was not utilized, these results were not statistically significant (3.1% vs 14.5%, respectively; p = 0.149). 13
Lebeis and colleagues described the PIF, which involves fixing available peritoneum surrounding the posterior bladder to the lateral aspect of the bladder using multiple interrupted sutures. 10 The authors hypothesized that lymphoceles develop after PLND because the bladder adheres to and walls off the lymphadenectomy bed, allowing lymphatic fluid to accumulate without being able to drain into the peritoneal cavity. The PIF prevents the bladder from scarring over the lymphadenectomy bed and creates a window for lymphatic fluid to drain into the peritoneal cavity where it can be absorbed. Their study showed that SL formed in 0/77 (0.0%) patients who underwent the PIF vs 9/77 (11.6%) patients who did not undergo the PIF (p = 0.003). Also, the postoperative nonlymphocele complication rate was comparable between both groups. 10
We externally validated the PIF in 117 consecutive patients who underwent transperitoneal RARP and bilateral PLND. We found that patients undergoing the PIF had a lower risk of SL formation postoperatively compared with those not undergoing the PIF (0.0% vs 6.0%, respectively; p = 0.007). This is consistent with the results of Lebeis and colleagues, who also did not note any SL formation in patients receiving the PIF. 10 These data are encouraging and suggest that the risk of SL after RARP and bilateral PLND may be significantly minimized by implementation of the PIF.
Some authors have speculated that the PIF may cause kinking of the bladder and adverse effects on postoperative micturation. Given this concern, Stolzenburg and colleagues described a technical modification to the PIF called the four-point peritoneal flap fixation (4PPFF). 11 The 4PPFF involves mobilizing perivesical and preperitoneal fat peritoneum to prevent the bladder from scarring over the lymph node dissection bed and create a pathway for lymphatic fluid to drain into the peritoneal cavity. In contrast to the PIF, the 4PPFF requires fixation of the peritoneum to the lateral pelvic wall rather than directly onto the bladder. The authors found that patients undergoing the 4PPFF had a lower incidence of SL formation after RARP and PLND compared with patients not undergoing the 4PPFF (1.0% vs 4.6%; p = 0.032). 11
Despite this theoretical concern, we found no difference in the rate of 3-month postoperative continence (p = 0.624), preoperative AUASS (p = 0.898), or postoperative AUASS (p = 0.470) between patients in the PIF group vs non-PIF group. This suggests that the PIF does not adversely affect urinary function in the postoperative setting. Although our findings do not completely rule out the possibility that the PIF may affect urinary function outcomes in the long term, it is unlikely that the PIF would result in a clinically significant detriment to urinary function in the long term if it did not adversely affect urinary function at 3 months postoperatively.
In addition, patients in the PIF group experienced longer mean operative times than those in the non-PIF group (196.9 ± 53.4 minutes vs 178.5 ± 44.0 minutes, respectively; p = 0.022). We believe that this difference may largely be attributed to the higher proportion of extended PLNDs performed in patients undergoing the PIF. The higher proportion of extended PLNDs performed in the PIF group may be explained by the higher risk prostate cancer associated with this group. There was a lower proportion of patients with GG1 disease in the PIF group compared with the non-PIF group (1.7% vs 13.4%, respectively; p = <0.001) and a higher (but not statistically significant) proportion of patients with GG ≥4 disease in the PIF group compared with the non-PIF group (25.6% vs 16.4%, respectively; p = 0.093). Although the additional time needed to perform the PIF may also contribute to higher operative times, this likely plays a secondary role as the PIF takes ∼5 minutes to perform. Furthermore, there was no significant difference in the proportion of patients with major (Clavien >2) 30-day non-SL complications between both groups (p = 0.800). This suggests that the PIF may be safely performed with minimal added morbidity.
The results of our study must be taken in the context of its limitations. First, our experience was limited by short-term follow-up, particularly in patients undergoing the PIF. Although some may argue that the shorter duration of follow-up in patients undergoing the PIF may contribute to the lower incidence of postoperative SL seen in this cohort, SL has been reported to be diagnosed at a mean of 19–32 days after RARP and PLND. 10,14,15 In our study, all patients had >3 months follow-up. Second, we did not routinely perform postoperative imaging, which may have reduced the number of lymphoceles detected. However, this limitation existed in both groups and likely did not affect our study conclusions. Third, our retrospective, nonrandomized study compared surgical outcomes before and after implementation of the PIF. However, besides the PIF, there were no major changes to the surgical technique during the study period. Also, it is unlikely that surgeon learning curve played a role in the lower incidence of SL formation in the PIF group as the primary surgeon had performed >1000 RARPs before the study period. Nevertheless, multi-institutional, randomized controlled trials are necessary to confirm the safety and effectiveness of utilizing the PIF to prevent lymphoceles after RARP and PLND.
Conclusions
Utilization of the PIF during transperitoneal RARP and bilateral PLND is a safe and effective method to decrease the risk of postoperative SL formation. The technique does not increase the risk of non-SL-related complications and does not adversely affect postoperative urinary function.
Footnotes
Author Disclosure Statement
M.L. and Z.L. have no competing financial interests. D.D.E. is a paid speaker and proctor for Intuitive surgical, consultant for Medtronic, and founder/part owner of Melzi Corp.
Funding Information
No funding was received for this article. Illustrations provided by Rob Duckwall.