
Abstract
Background:
To test contemporary rates and predictors of open conversion at minimally invasive (laparoscopic or robotic) radical prostatectomy (MIRP).
Materials and Methods:
Within the National Inpatient Sample database (2008–2015), we identified all MIRP patients and patients who underwent open conversion at MIRP. First, estimated annual percentage changes (EAPCs) tested temporal trends of open conversion. Second, multivariable logistic regression models predicted open conversion at MIRP. All models were weighted and adjusted for clustering, as well as all available patient and hospital characteristics.
Results:
Of 57,078 MIRP patients, 368 (0.6%) underwent open conversion. The rates of open conversion decreased over time (from 1.80% to 0.38%; EAPC: −26.0%; p = 0.003). In multivariable logistic regression models predicting open conversion, patient obesity (odds ratio [OR]: 2.10; p < 0.001), frailty (OR: 1.45; p = 0.005), and Charlson comorbidity index (CCI) ≥2 (OR: 1.57; p = 0.03) achieved independent predictor status. Moreover, compared with high-volume hospitals, medium-volume (OR: 2.03; p < 0.001) and low-volume hospitals (OR: 3.86; p < 0.001) were associated with higher rates of open conversion. Last but not least, when the interaction between the number of patient risk factors (obesity and/or frailty and/or CCI ≥2) and hospital volume was tested, a dose–response effect was observed. Specifically, the rates of open conversion ranged from 0.3% (patients with zero risk factors treated at high-volume hospitals) to 2.2% (patients with two to three risk factors treated at low-volume hospitals).
Conclusion:
Overall contemporary (2008–2015) rate of open conversion at MIRP was 0.6% and it was strongly associated with patient obesity, frailty, CCI ≥2, and hospital surgical volume. In consequence, these parameters should be taken into account during preoperative patients counseling, as well as in clinical and administrative decision making.
Introduction
Over the past decades, minimally invasive radical prostatectomy (MIRP: laparoscopic or robotic radical prostatectomy [RP]) has become the preferred surgical approach for patients with prostate cancer. 1,2 Compared with open retropubic RP, MIRP offers decreased postoperative pain, shorter hospital stay, and more rapid return to normal activities. 3,4 Moreover, MIRP was associated with comparable intermediate time oncologic outcomes, relative to open retropubic RP. 5,6 Despite the increased use of MIRP, open conversion may occur because of intraoperative complications, failure to progress, anatomical difficulty, or cancer control considerations. The rates of open conversion at MIRP have been poorly investigated. 7 –10 In the era of laparoscopic surgery (2000–2005), Bhayani et al. [8] and Hu et al. 7 reported conflicting results in terms of open conversion rates at MIRP, which ranged from 1.9% to 28.6%. More contemporary data were reported by Sharma and Meeks 10 and Weiner and colleagues 9 However, Sharma and Meeks 10 heavily relied on patients treated in the era of robotic RP development (2004–2010). Moreover, Weiner and colleagues 9 focused on a short time series that spanned years 2010–2011. We hypothesized lower contemporary rates of open conversion at MIRP, because of increased use of the robotic technology and higher confidence of surgeons with MIRP. Moreover, we also hypothesized that several patient and hospital characteristics could predict open conversion at MIRP. To address this void, we examined a contemporary RP series (2008–2015) within a large population-based data repository and tested rates and predictors of open conversion at MIRP.
Materials and Methods
Study population
We relied on the National Inpatient Sample (NIS) database (2008–2015) 11 that is composed of longitudinal hospital inpatient databases from the Healthcare Cost and Utilization Project and includes 20% of United States inpatient hospitalizations. We focused on patients aged ≥18 years with primary diagnosis of nonmetastatic prostate cancer (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] code 185.0), treated with RP (primary procedure ICD-9-CM code 65.0). Secondary procedure codes were used to identify laparoscopic or robotic approach (ICD-9-CM codes 54.21 and 17.42) and lymph node dissection (ICD-9-CM codes 40.3/40.5).
Outcomes of interest
We focused on open conversion rates at MIRP. Patients were considered to have undergone open conversion if the codes for open conversion (ICD-9-CM codes V64.4 and V64.41) appeared during the same admission as the code for RP. This methodology was consistent with previous studies that relied on the NIS. 12,13 Since the majority of open conversion cases were coded as open RP + open conversion, distinction between laparoscopic and robotic MIRP was not possible.
Variables definition
Demographic characteristics consisted of age at surgery, race (Caucasian, African American, and Others), year of surgery, Charlson comorbidity index (CCI), obesity (body mass index [BMI] ≥30), frailty, income, and insurance status (private, Medicare, Medicaid, and other). Specifically, CCI was defined according to the Deyo adaptation for ICD-9 codes-based databases 14 and categorized as CCI 0–1 vs CCI ≥2. Moreover, frailty (categorized as frail vs nonfrail patients) was defined according to the Johns Hopkins Adjusted Clinical Groups (ACG) frailty-defining diagnoses indicator and was calculated using patients' ICD-9 codes available in the NIS, as previously reported. 15,16
Hospital region (Northeast, Midwest, South, and West), hospital teaching vs nonteaching status, hospital bed size (small, medium, and large), and hospital annual volume (tertiles: low, medium, and high), which represents the number of MIRPs performed at each participating institution during each study calendar year, were considered.
Statistical analyses
First, differences in medians and proportions were assessed by, respectively, the Kruskal–Wallis and the chi-square tests. Second, estimated annual percentage changes (EAPCs) tested temporal trends of open conversion over time. Third, open conversion rates at MIRP were tested in multivariable logistic regression models. All multivariable models relied on generalized estimating equations to further adjust for clustering.
11
Subsequently, data distribution was adjusted according to the provided NIS population weights to render estimates more accurate nationally.
11
All statistical tests were two sided with a level of significance set at p < 0.05. All analyses were performed using the R software environment for statistical computing and graphics (version 3.4.1;
Results
Descriptive analyses and trends over time
Of 57,078 MIRP patients, 368 (0.6%) underwent open conversion (Table 1). Patients who underwent open conversion more frequently were obese (15.5% vs 8.4%; p < 0.001) and frail (19.8% vs 13.6%; p < 0.001) and more frequently had CCI ≥2 (6.2% vs 3.4%; p = 0.004) and low-income status (1st quantile: 26.9% vs 21%; p = 0.02). Moreover, patients who underwent open conversion less frequently received lymph node dissection (29.3% vs 37.6%; p < 0.001). Finally, patients who underwent open conversion more frequently were treated at low-volume hospitals (45.4% vs 26.7%; p < 0.001), at nonteaching hospitals (42.7% vs 27%; p < 0.001), and at large bed size hospitals (69.3% vs 64.2%; p = 0.03).
Descriptive Characteristics of 57,078 Minimally Invasive Radical Prostatectomy Patients (Unweighted Population) Identified Within National (Nationwide) Inpatient Sample Database from 2008 to 2015 and Stratified According to Presence or Absence of Open Conversion
Boldface type indicates statistically significant p-values (p < 0.05).
CCI = Charlson comorbidity index; IQR = interquartile range.
Time trends revealed a decrease in the rates of open conversion over time (from 1.80% to 0.38%; EAPC: −26.0%; p = 0.003; Fig. 1).
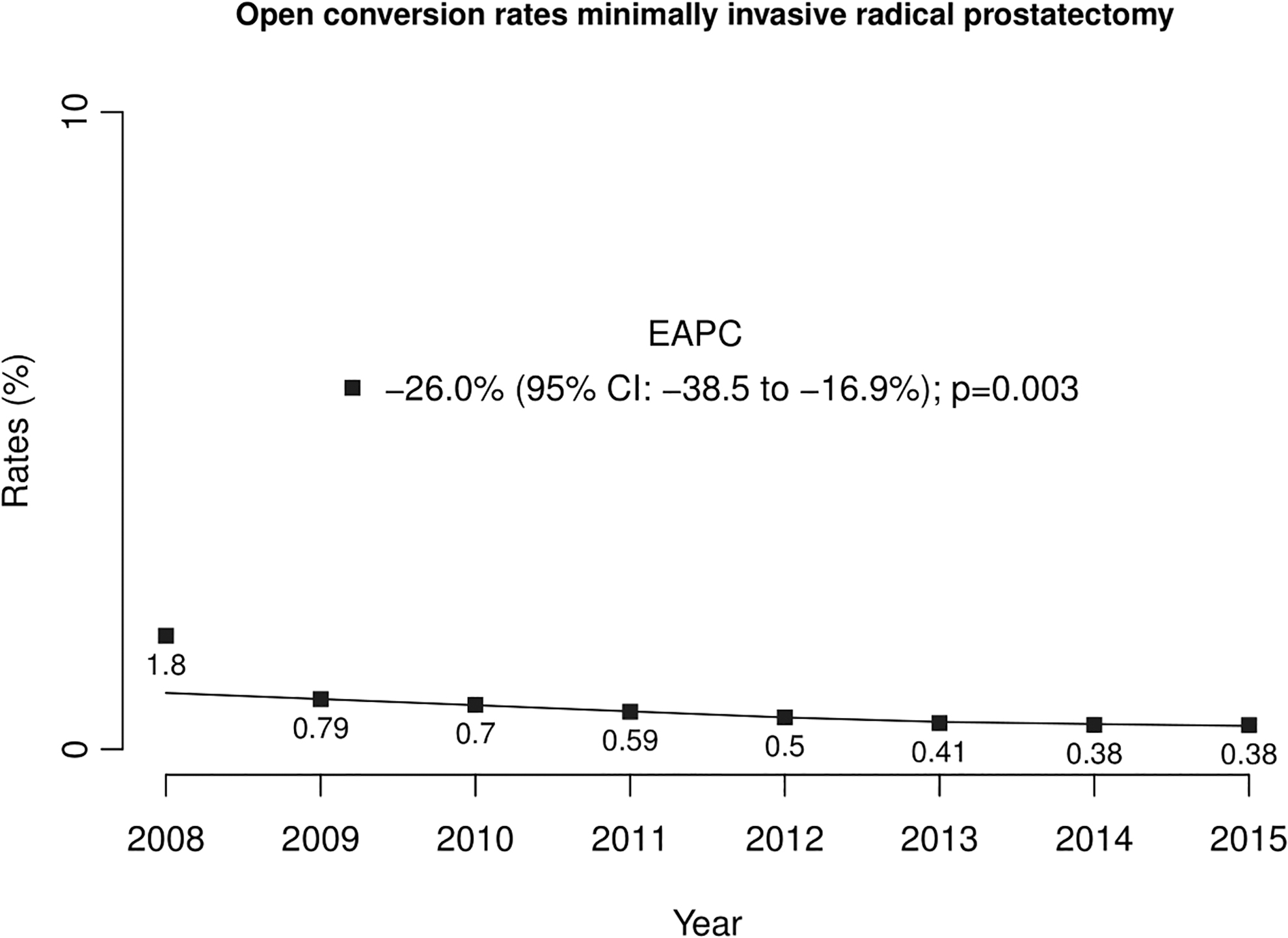
Annual rates of open conversion in patients treated with minimally invasive prostatectomy identified within the National (Nationwide) Inpatient Sample database from 2008 to 2015. EAPCs = estimated annual percentage changes; NIS = National (Nationwide) Inpatient Sample.
Crude rates of open conversion according to patient and hospital characteristics
The rates of open conversion in obese vs nonobese patients were, respectively, 1.2% vs 0.6% (p < 0.001; Fig. 2A). In addition, the rates of open conversion in frail vs nonfrail patients were, respectively, 1.0% vs 0.6% (p < 0.001; Fig. 2B). Moreover, the rates of open conversion in CCI ≥2 vs CCI 0–1 patients were, respectively, 1.2% vs 0.6% (p = 0.004; Fig. 2C). Finally, hospital volume and hospital teaching status resulted in differences in open conversion rates. Specifically, open conversion rates at low vs medium vs high-volume hospitals were, respectively, 1.1% vs 0.6% vs 0.3% (Fig. 2D). Moreover, open conversion rates at nonteaching vs teaching hospitals were, respectively, 1.0% vs 0.5% (p < 0.001; Fig. 2E). No other patient or hospital characteristics were associated with higher rates of open conversion.
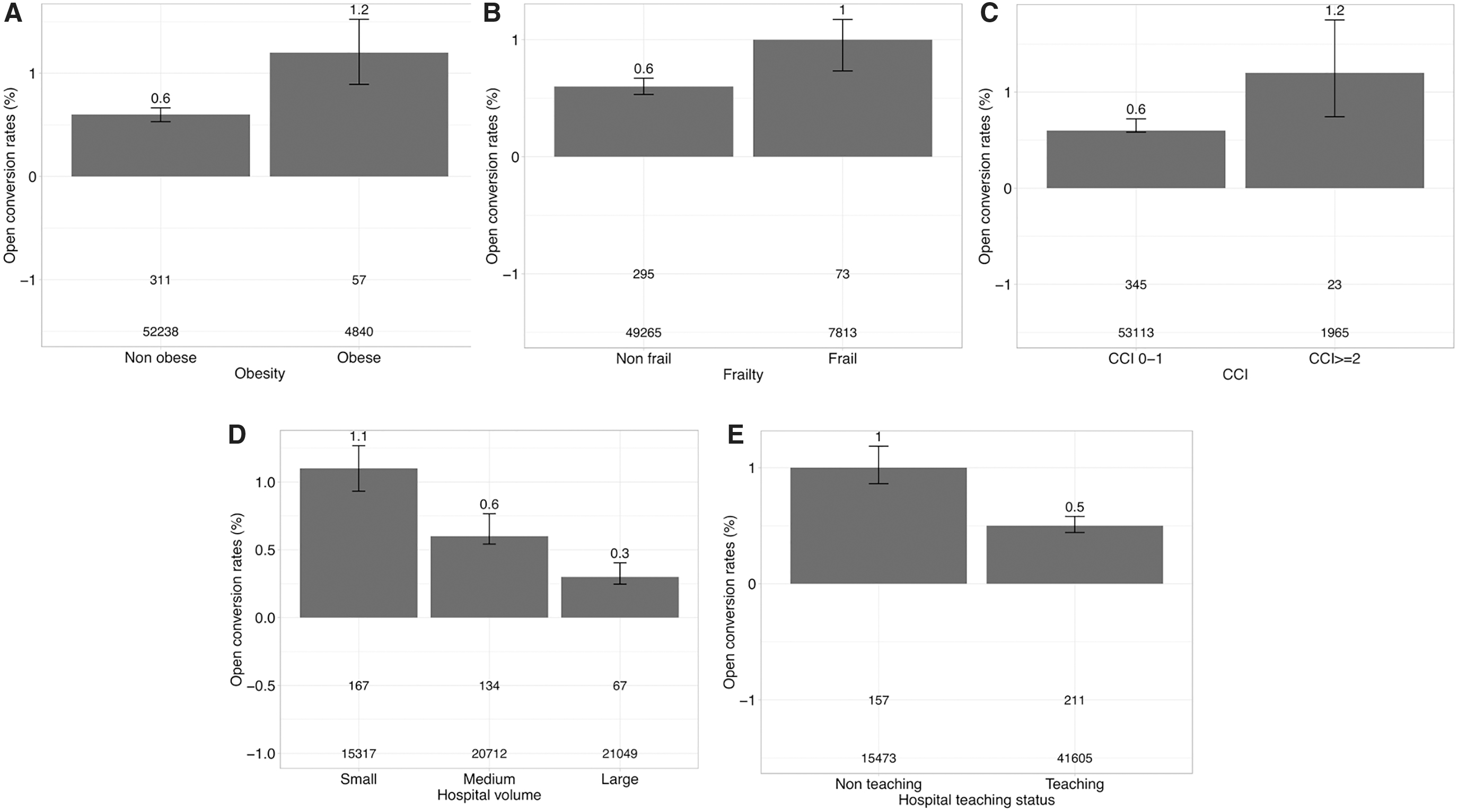
Bar plots depicting crude rates of open conversion in patients treated with minimally invasive radical prostatectomy (unweighted population) identified within the NIS database from 2008 to 2015.
Multivariable analyses predicting open conversion rates
In multivariable logistic regression models (Table 2), obesity (odds ratio [OR]: 2.10; p < 0.001), frailty (OR: 1.45; p = 0.005), and CCI ≥2 (OR: 1.57; p = 0.03) were associated with higher rates of open conversion. Moreover, MIRP at medium (OR: 2.03; p < 0.001) and low-volume hospitals (OR: 3.86; p < 0.001) was associated with higher rates of open conversion than MIRP at high-volume hospitals.
Multivariable Logistic Regression Models Predicting Open Conversion Rates in Patients Treated with Minimally Invasive Radical Prostatectomy Within the National Inpatient Sample Database (2008–2015)
Boldface type indicates statistically significant p-values (p < 0.05).
All models were weighted and adjusted for clustering.
CI = confidence interval; OR = odds ratio.
Crude rates of open conversion according to obesity, frailty, CCI, and hospital volume: dose–response effect
The association between the number of patient risk factors (namely: obesity and/or frailty and/or CCI ≥2) and hospital volume yielded different conversion rates. At small-volume hospitals, the rates of open conversion were, respectively, 0.9% versus 1.5% versus 2.2% in patients with zero versus one versus —two to three risk factors (Fig. 3). At medium-volume hospitals, the rates of open conversion were, respectively, 0.6% versus 0.9% versus 1.8% in patients with zero versus one versus two to three risk factors. Finally, at high-volume hospitals, the rates of open conversion were, respectively, 0.3% vs 0.5% vs 0.9% in patients with zero versus one versus two to three risk factors.

Bar plots depicting crude rates of open conversion in patients treated with minimally invasive radical prostatectomy (unweighted population) identified within the NIS database from 2008 to 2015. Patients are stratified according to hospital volume and according to the number of risk factors (obesity, frailty, and CCI).
Multivariable analyses predicting open conversion rates according to obesity, frailty, CCI, and hospital volume: dose–response effect
The independent predictor status of the association between the number of patient risk factors (namely: obesity and/or frailty and/or CCI ≥2) and hospital volume was confirmed in multivariable logistic regression models predicting open conversion rates, which revealed a significant and gradual dose–response effect (Table 2). Specifically, compared with patients with zero risk factors treated at high-volume hospitals, the highest OR was observed in patients with two to three risk factors treated at low-volume hospitals (OR: 9.72; p < 0.001). Conversely, the lowest OR was recorded in patients with one risk factor treated at high-volume hospitals (OR: 1.75; p = 0.01).
Discussion
Only four previous studies examined the rates of open conversion at MIRP. 7 –10 However, three of these reports heavily relied on patients treated in the era of laparoscopic MIRP and considered surgeons at the beginning of their learning curve. 7,8,10 Moreover, Weiner and colleagues 9 focused on a short time series that spanned years 2010–2011. Therefore, these data could not be representative of the current situation in the United States. Based on lack of data on contemporary rates of open conversion during MIRP, we tested temporal trends and predictors of open conversion in a large population-based MIRP cohort (n = 57,078) that spanned years 2008–2015. Our results showed several important findings.
First, open conversion occurred in 0.6% of contemporary MIRPs. Moreover, the rates of open conversion at MIRP decreased over time (from 1.80% to 0.38%; EAPC: −26.0%). Our findings are consistent with a previous temporal trend analysis (2004–2010) by Sharma and Meeks, 10 in which the rates of open conversion at MIRP decreased from 7.2% to 0.7%. However, the report of Sharma and Meeks 10 heavily relied on patients treated in the era of laparoscopic RP and, therefore, considered surgeons at the beginning of their robotic RP learning curve. In consequence, to the best of our knowledge, we are the first to show decreasing rates of open conversion at MIRP in the era of robotic RP (2008–2015). Several hypothetical explanations could justify this encouraging trend. First, robotic approach is increasingly being used for MIRP in the United States. 1,2 Oberlin et al. [ 17 reported that the performance of robotic MIRP in the United States increased from 22% of all RP in 2003 to 85% in 2013. Indeed, robotic MIRP was previously associated with lower rates of intraoperative and postoperative complications and with a shorter learning curve than laparoscopic MIRP. 18,19 Second, the technique of MIRP and surgeon experience have improved over time. Unfortunately, we were unable to validate these two specific hypotheses because of inherent limitation of the NIS database. Specifically, we were unable to distinguish between open conversions of laparoscopic and robotic MIRPs, as the majority of open conversions were coded as an open procedure. Moreover, surgeon experience is unavailable within the NIS. Therefore, the observed decreasing trends of open conversion at MIRP should be tested in other large data repositories that systematically register surgical approach and surgeon experience.
Second, the rates of open conversion at MIRP varied according to patient and hospital characteristics. Specifically, obese (1.2% vs 0.6%; p < 0.001), frail (1.0% vs 0.6%; p < 0.001), or CCI ≥2 (1.2% vs 0.6%; p = 0.004) patients experienced higher rates of open conversion, relative to their nonobese, nonfrail, or CCI 0–1 counterparts. Moreover, patients treated at low- and medium-volume hospitals were at higher risk of open conversion than patients treated at high-volume hospitals (1.1% vs 0.6% vs 0.3%). These findings were confirmed in multivariable logistic regression models predicting open conversion rates, where obesity, frailty, CCI ≥2, and hospital volume achieved independent predictor status, even after full adjustment for all available patient and hospital characteristics. Obesity, frailty, CCI ≥2, and low hospital volume were previously associated with higher rates of perioperative complications in patients treated with RP. 20 –29 Moreover, our findings are consistent with a previous study by Sharma and Meeks 10 that reported patient obesity and low hospital volume as independent predictors of open conversion at MIRP. However, to the best of our knowledge, the association between CCI or patient frailty and higher rates of open conversion at MIRP was never previously reported.
Third, when the interaction between the number of patient risk factors (obesity and/or frailty and/or CCI ≥2) and hospital volume was tested, a dose–response effect was observed. Specifically, the rates of open conversion ranged from 0.3% (patients with zero risk factors treated at high-volume hospitals) to 2.2% (patients with two to three risk factors treated at low-volume hospitals). Moreover, when multivariable logistic regression models were refitted according to the number of patient risk factors and treatment at either low- vs medium- vs high-volume hospitals, the independent predictor status of the dose–response effect was confirmed. Specifically, a gradual increase was recorded when a higher number of risk factors and decreasing hospital volume were combined. Compared with patients with 0 risk factors treated at high-volume hospitals, the highest OR was recorded when two to three risk factors and low-volume hospital characteristics were combined (OR: 9.72). Conversely, lower ORs were recorded when patients with two to three risk factors were treated at medium- (OR: 7.69) or high-volume hospitals (OR: 3.36), as well as when patients with one risk factor were treated at low- (OR: 6.51), medium- (OR: 3.33), and high-volume hospitals (OR: 1.75). Finally, lower ORs were also recorded when patients with zero risk factors were treated at low- (OR: 3.98) or medium-volume hospitals (OR: 2.04). These results are important for preoperative patient counseling, clinical decision making, and in health care administration.
Taken together, to the best of our knowledge, we provided the first large-scale contemporary analysis addressing open conversion rates at MIRP. Our findings showed that 0.6% of contemporary MIRPs are converted to open RP and that the rates of open conversion decreased over time. Moreover, obesity, frailty, CCI ≥2, and hospital volume achieved independent predictor status in multivariable models testing open conversion rates, even after adjustment for patient and hospital characteristics. Last but not least, when patients where stratified according to the number of risk factors and hospital volume, we observed a significant dose–response effect. Specifically, the rates of open conversion at MIRP ranged from 0.3% (patients with zero risk factors treated at high-volume hospitals) to 2.2% (patients with two to three risk factors treated at low-volume hospitals). In consequence, it may be advisable to systematically record BMI, CCI, and frailty index in all MIRP candidates. Patients should be informed about the possibility of open conversion at MIRP, according to the number of their risk factors, as well as hospital surgical volume.
Despite its novelty, our study has limitations. First, the data are retrospective and, therefore, influenced by inherent selection bias. Second, as previously stated, we were unable to distinguish between open conversions of laparoscopic and robotic MIRPs, as the majority of open conversions were coded as an open procedure. Third, the NIS database 11 lacks information about surgical technique or individual surgeon experience. However, Sharma and Meeks 10 showed that hospital and surgeon MIRP volume are two highly correlated variables (R = 0.7, p < 0.001). We, therefore, believe that hospital volume could represent a good, but not perfect, surrogate of individual surgeon volume. In consequence, open conversion at MIRP should be tested in other large data repositories that systematically register surgical approach and surgeon experience. Fourth, information on performance status, ASA score, lookback period of CCI assessment, and laboratory values is not available within the NIS database. Fifth, the NIS database does not capture specific reasons for open conversion during MIRP. Open conversion may occur because of intraoperative complications, failure to progress, anatomical difficulty, cancer control considerations, or anesthesiologist's request. The impact of these specific reasons should be, therefore, tested in other large data repositories. Finally, since the NIS database does not provide tumor characteristics, such as stage and grade, we were unable to adjust our analyses for these variables.
Conclusion
Overall contemporary (2008–2015) rate of open conversion at MIRP was 0.6% and it was strongly associated with patient obesity, frailty, CCI ≥2, and hospital surgical volume. In consequence, these parameters should be taken into account during preoperative patients counseling, as well as in clinical and administrative decision making.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.